Exhibit 99.1
Aprea Therapeutics Reports First Quarter 2026 Financial Results and Provides a Corporate Update
| • | Oversubscribed $30 million private placement closed, with proceeds expected to support ongoing development of APR-1051 |
| • | Two partial responses observed with continued encouraging tolerability in the ongoing Phase 1 dose escalation ACESOT-1051 trial of WEE1 inhibitor APR-1051 |
| • | Additional clinical data from ACESOT-1051 to be provided at the ASCO 2026 Annual Meeting on May 30, 2026 |
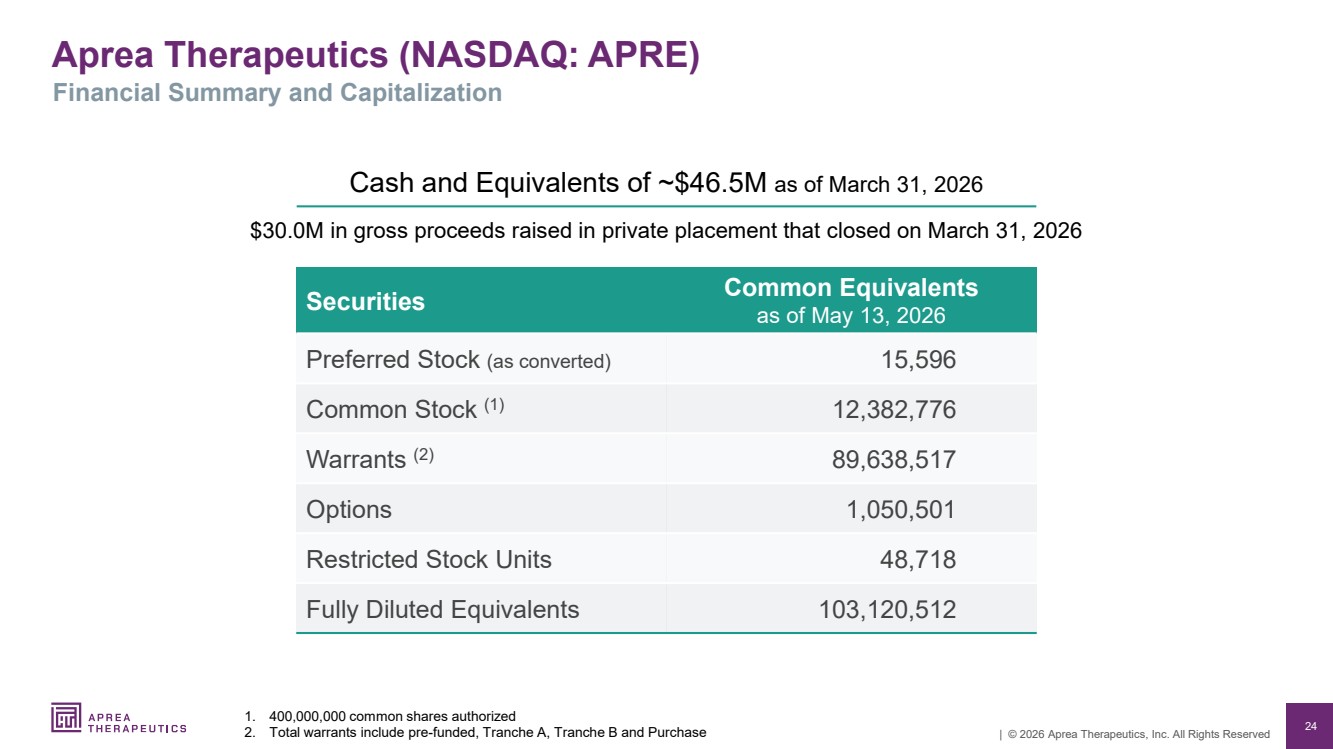
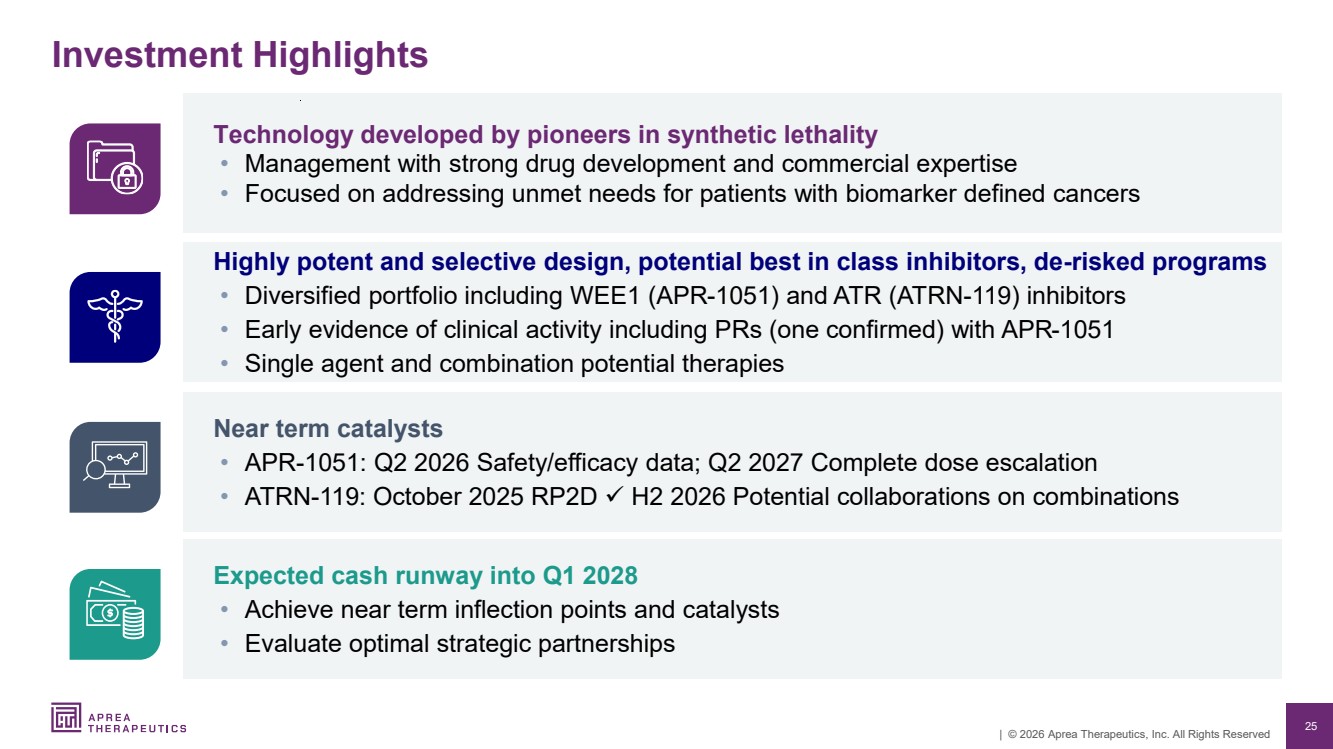
| • | $46.5 million in cash and cash equivalents as of March 31, 2026, with anticipated cash runway into Q1 2028 |
DOYLESTOWN, PA, May 13, 2026 (GLOBE NEWSWIRE) – Aprea Therapeutics, Inc. (Nasdaq: APRE) (“Aprea”, or the “Company”), a clinical-stage precision medicine oncology company focused on the discovery and development of targeted therapies for patients with biomarker-defined cancers, today reported financial results for the first quarter ended March 31, 2026, and provided a business update.
“We are very encouraged by the progress made across both our clinical and corporate priorities during the first quarter of 2026, including two partial responses observed in the ACESOT-1051 trial evaluating APR-1051. One of these has been confirmed at a second imaging assessment and this patient remains on study,” said Oren Gilad, Ph.D., President and Chief Executive Officer of Aprea. “These efficacy results, coupled with the encouraging tolerability, support our precision medicine strategy and reinforce the potential of targeted therapies for patients who have limited treatment options. We look forward to presenting an update from ACESOT-1051 at ASCO 2026 and providing additional insight into APR-1051’s emerging clinical profile. The recent $30 million private placement significantly strengthens our balance sheet and enables us to meaningfully expand patient enrollment, generating the clinical data needed to inform the future clinical path for APR-1051. We are grateful for the trust and support of both new and existing investors, whose participation reflects confidence in our development strategy and the potential of our programs.”
Key Business Updates and Upcoming Key Milestones
ACESOT-1051: A Biomarker Focused, Phase 1 Trial of Oral WEE1 inhibitor, APR-1051
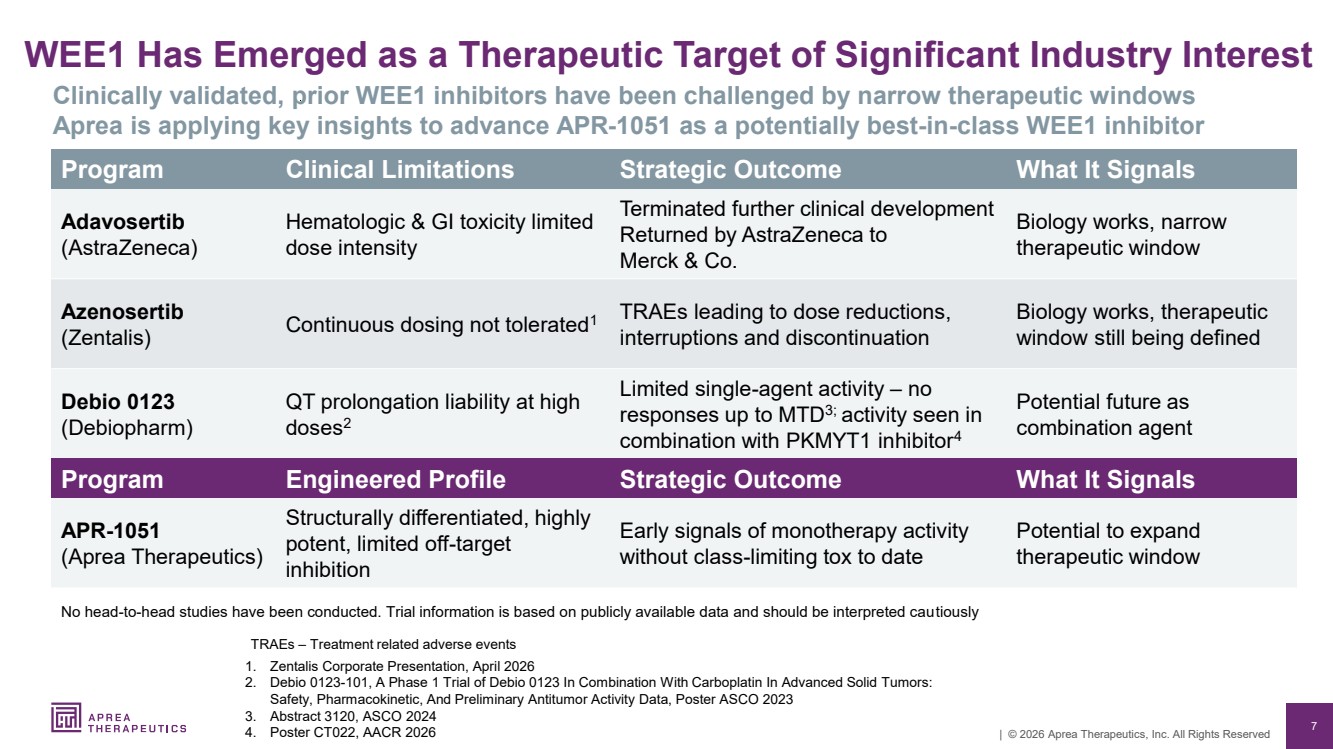
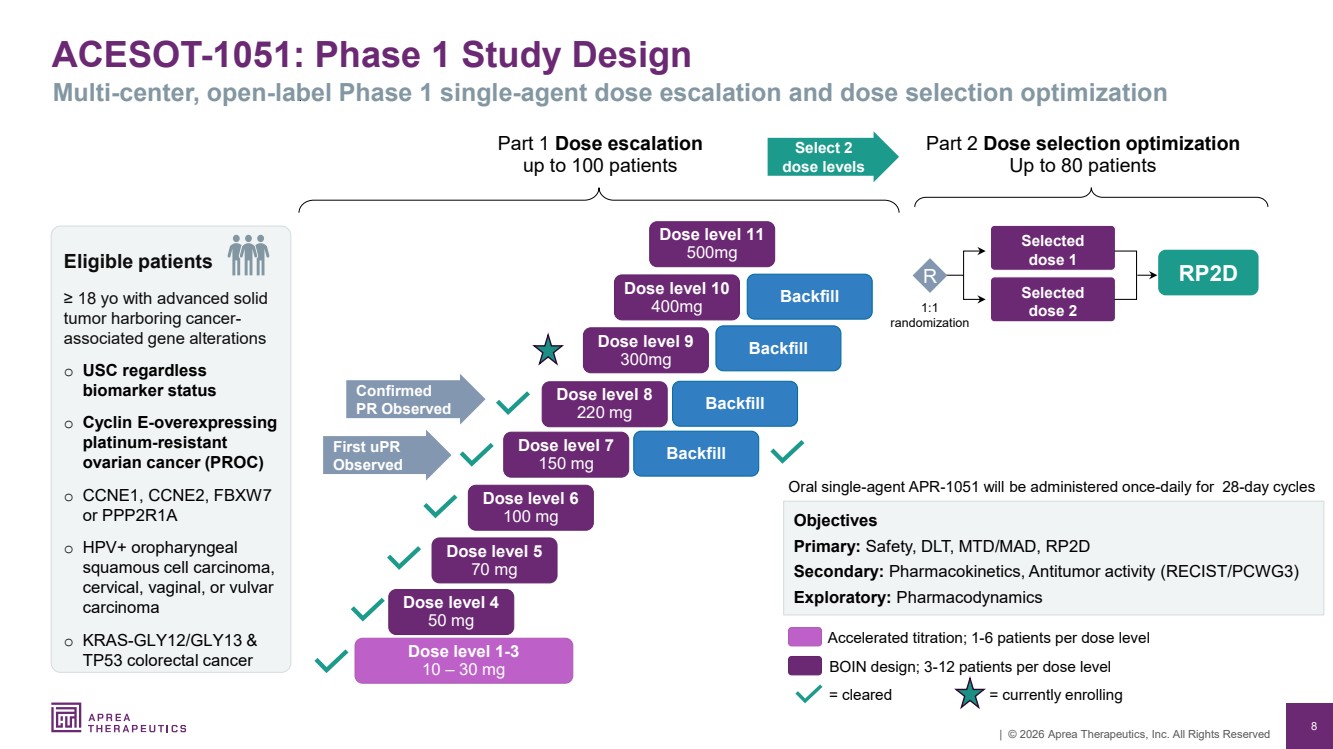
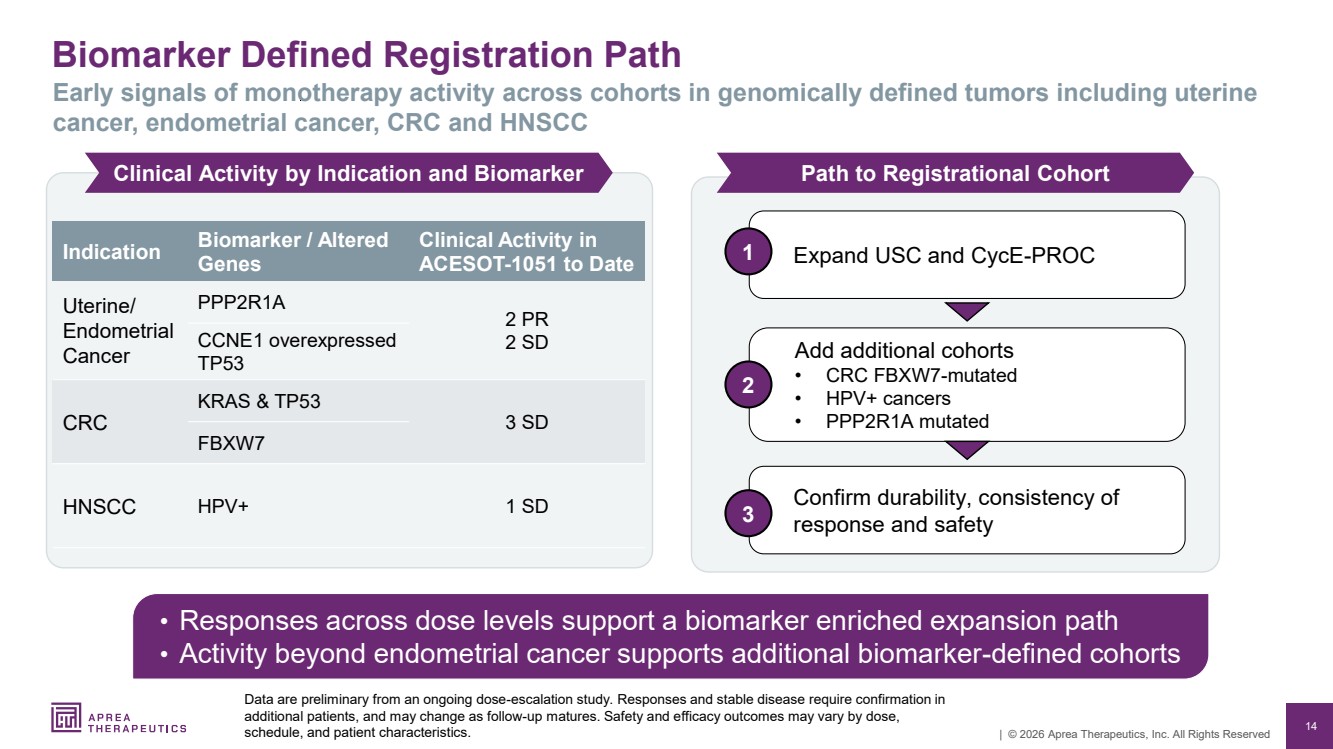
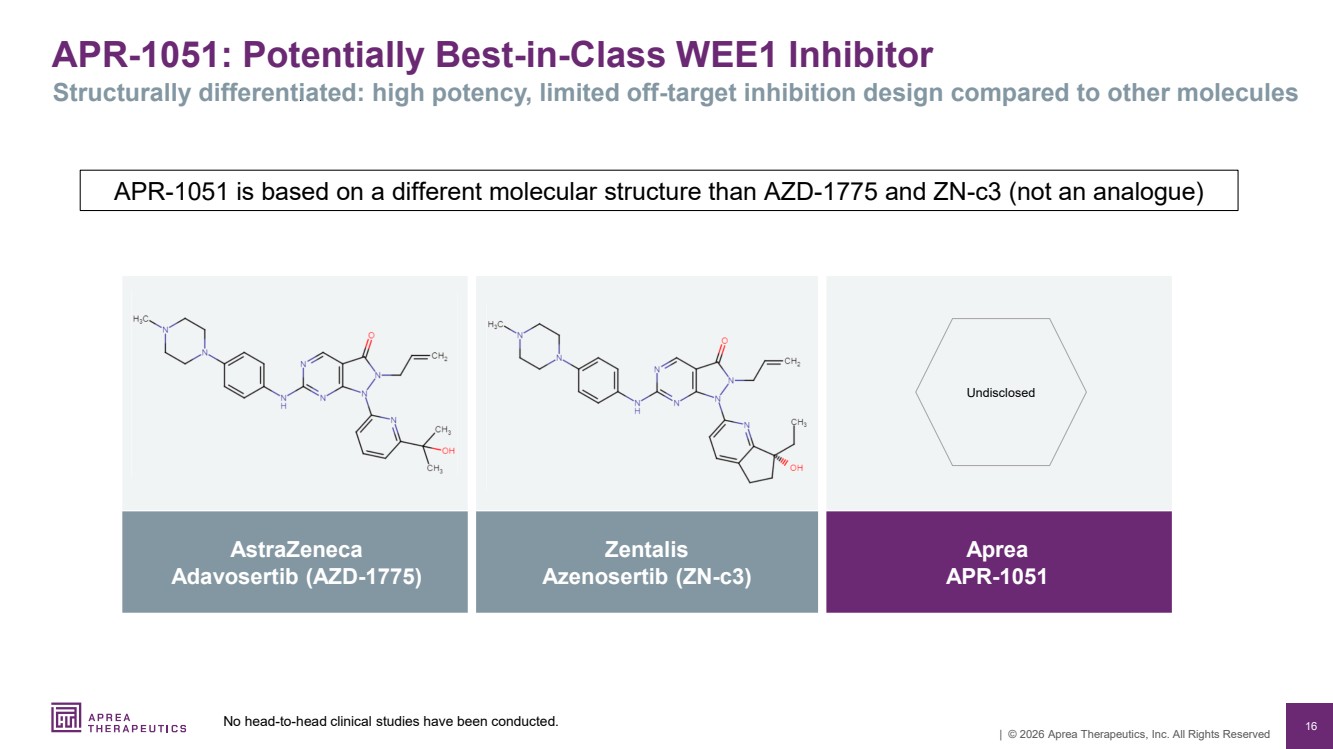
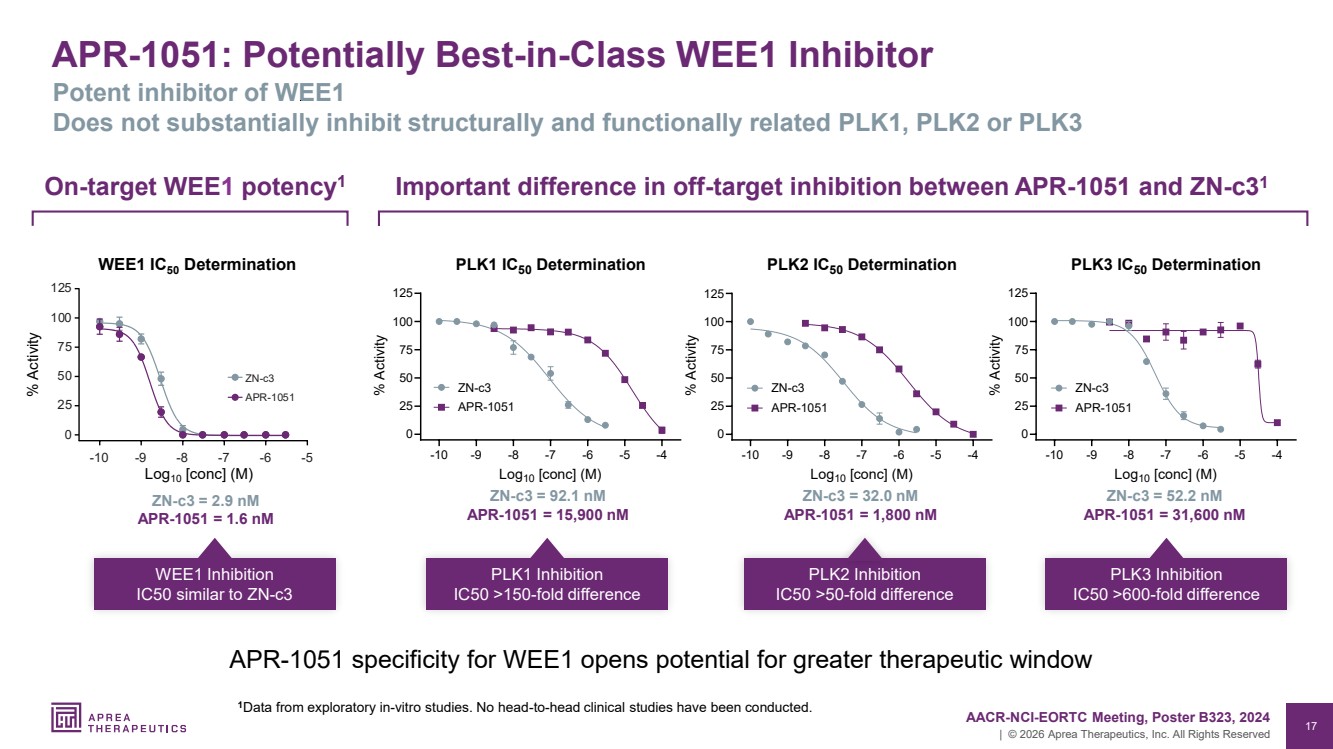
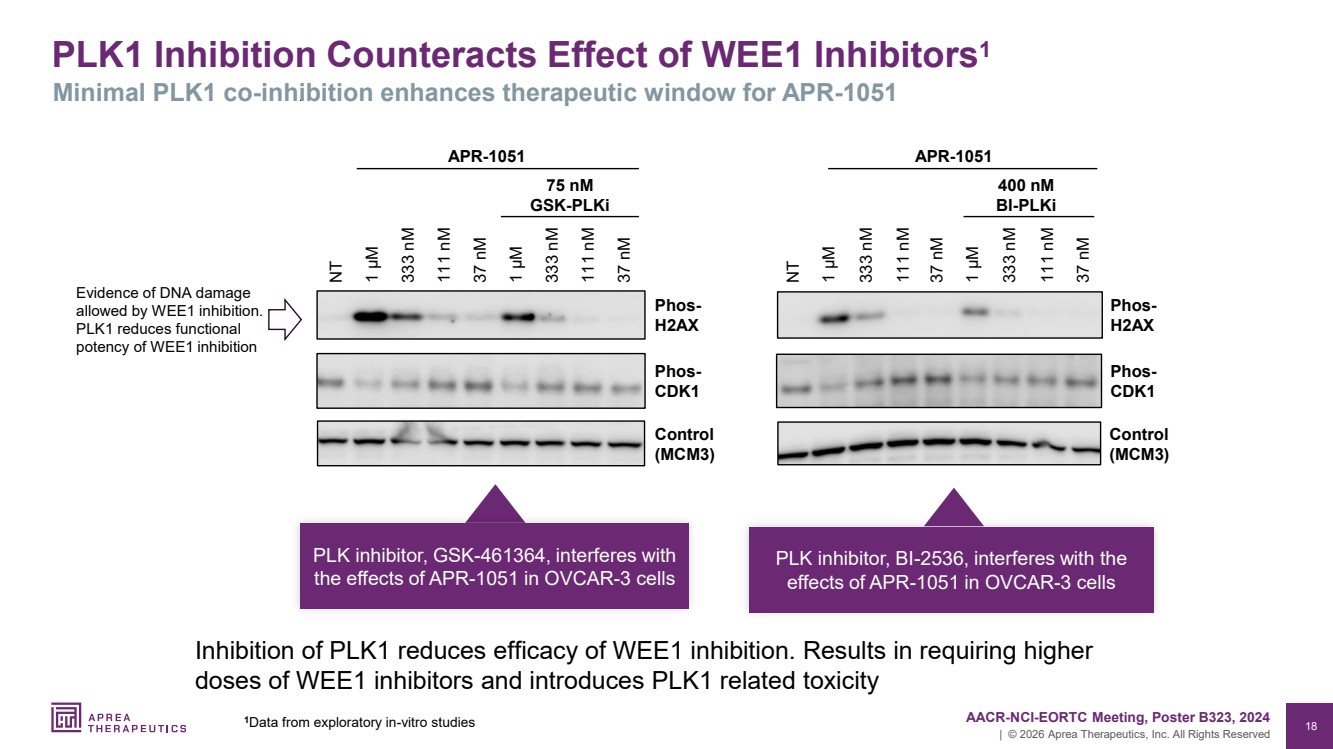
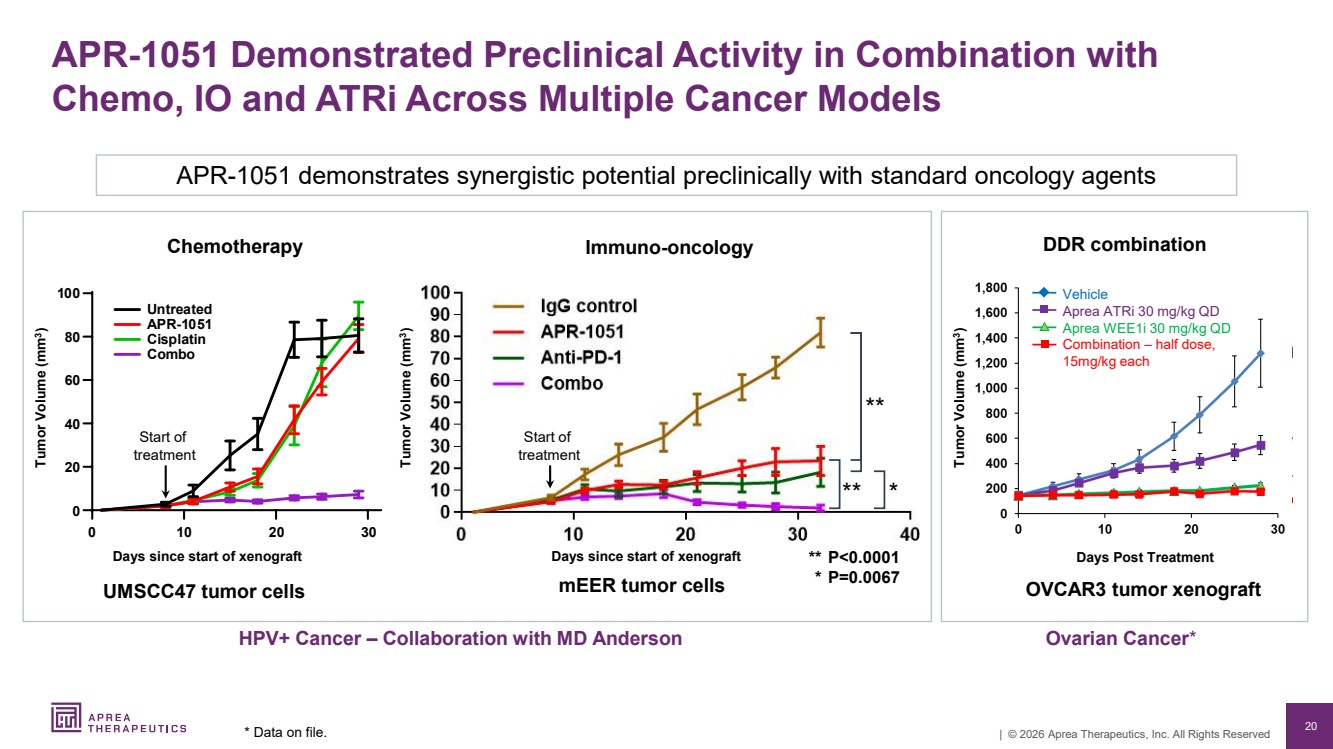
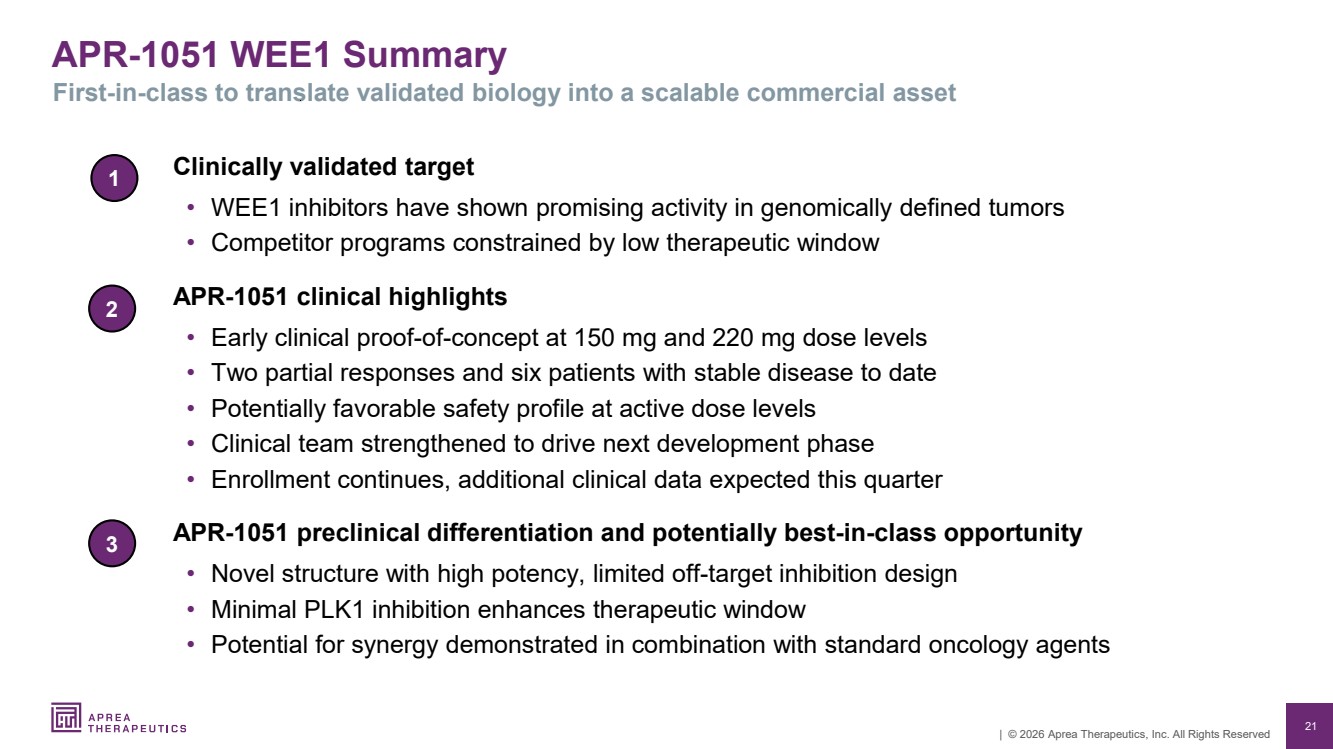
| • | APR-1051 is a potent and selective, oral small molecule WEE1 inhibitor designed to potentially address therapeutic window limitations observed with earlier WEE1 programs. APR-1051 is being evaluated as monotherapy in uterine serous carcinoma patients regardless of mutation, cyclin E-overexpressing platinum-resistant ovarian cancer, advanced solid tumors harboring CCNE1, CCNE2, PPP2R1A or FBXW7 mutations, colorectal cancer harboring KRAS & TP53 mutations and HPV+ head and neck squamous cell carcinoma. These patient populations are associated with poor prognosis and limited effective treatment options. |
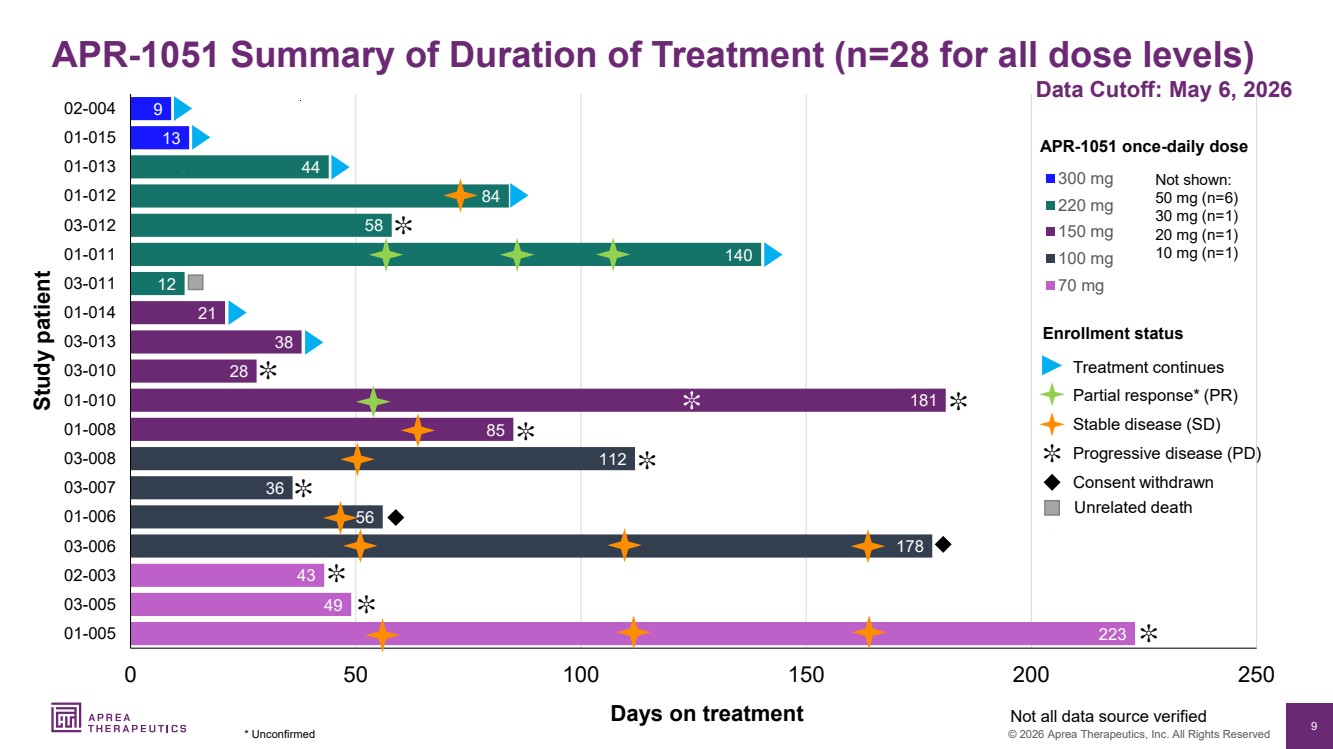
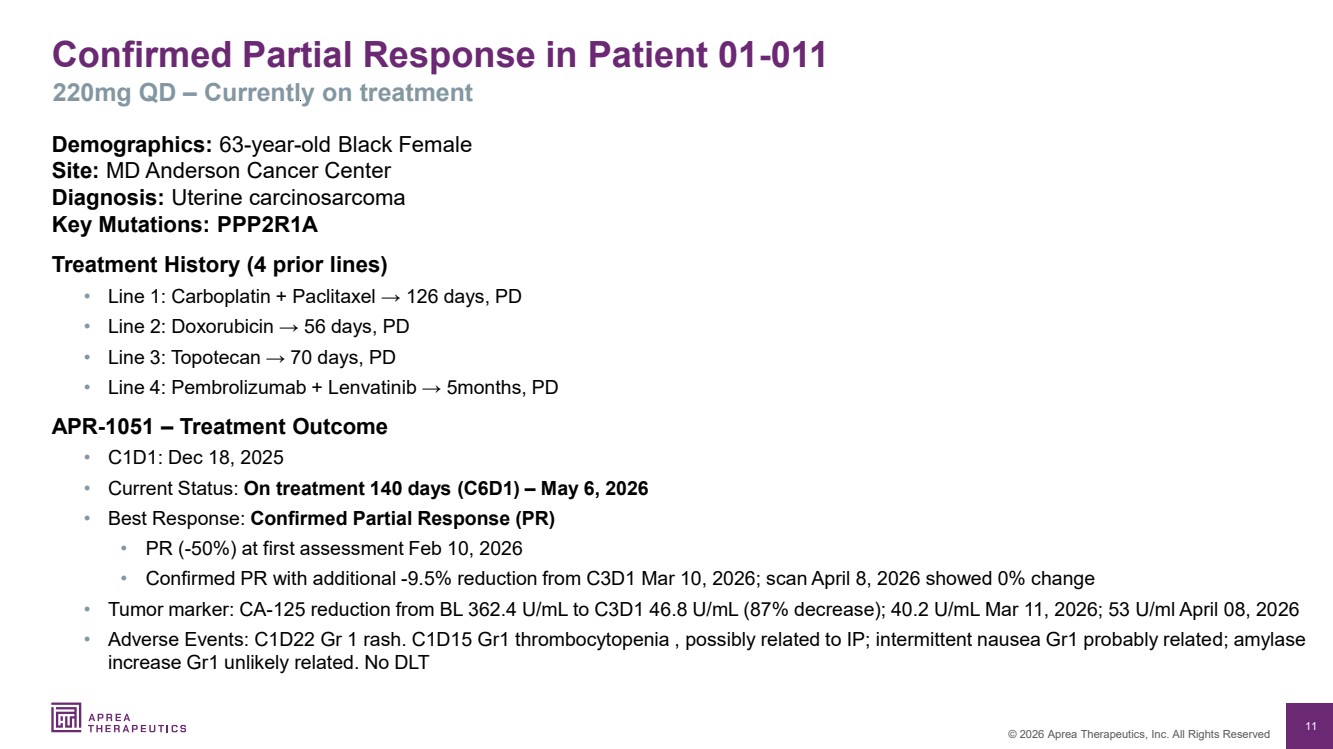
| • | To date, two patients in ACESOT-1051 have achieved partial responses (“PR”). One uterine carcinosarcoma patient with PPP2R1A-mutation treated at the 220 mg dose level achieved a 50% reduction in target lesion size per RECIST v1.1 criteria and a significant reduction in CA-125 levels at the first imaging assessment. At the confirmatory, second imaging assessment, an additional 9.5% reduction in target lesion size was observed, along with a further decline in CA-125 to 40.2 U/mL |
| from 362 U/mL at baseline. This patient remains on study with an ongoing PR. There has also been an unconfirmed PR in a second patient with PPP2R1A-mutated uterine serous carcinoma, treated at the 150 mg dose level. |
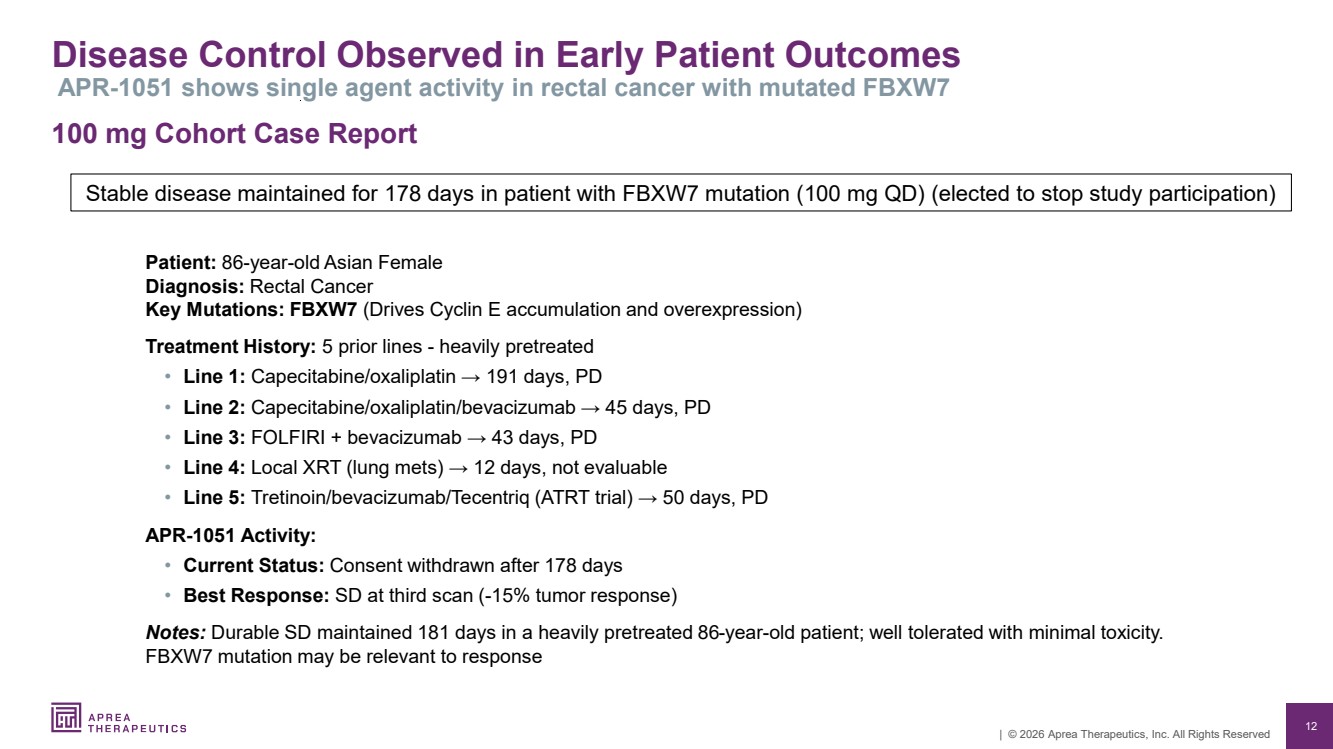
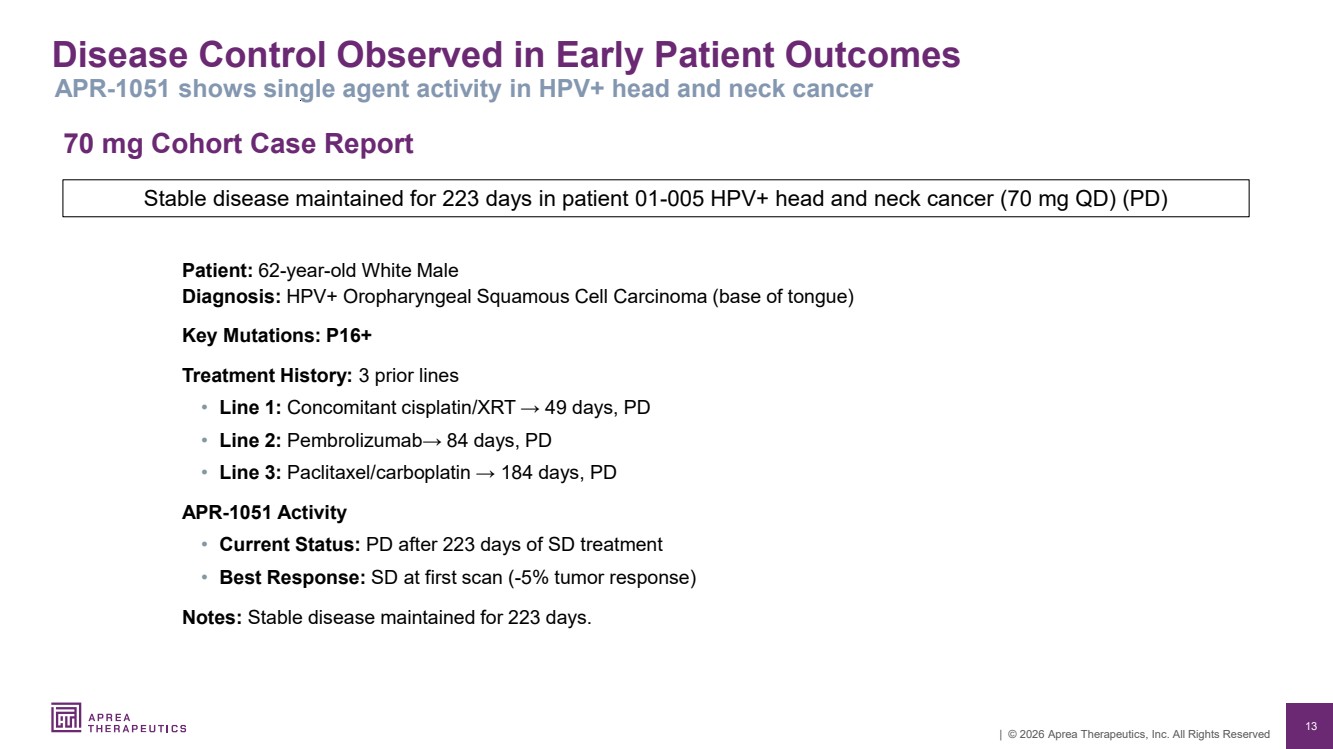
| • | A total of 28 patients have been treated in ACESOT-1051 to date at doses ranging from 10 mg to 300 mg once daily. Six patients have achieved best overall response of stable disease, including patients with colorectal cancer, HPV+ head and neck squamous cell carcinoma, and endometrial cancer. |
| • | Dose escalation is ongoing with enrollment currently underway in the 300 mg cohort (dose level 9). Additional eligible patients will be backfilled at 220 mg to further characterize safety, tolerability, and clinical activity, once dose level 9 is fully enrolled. |
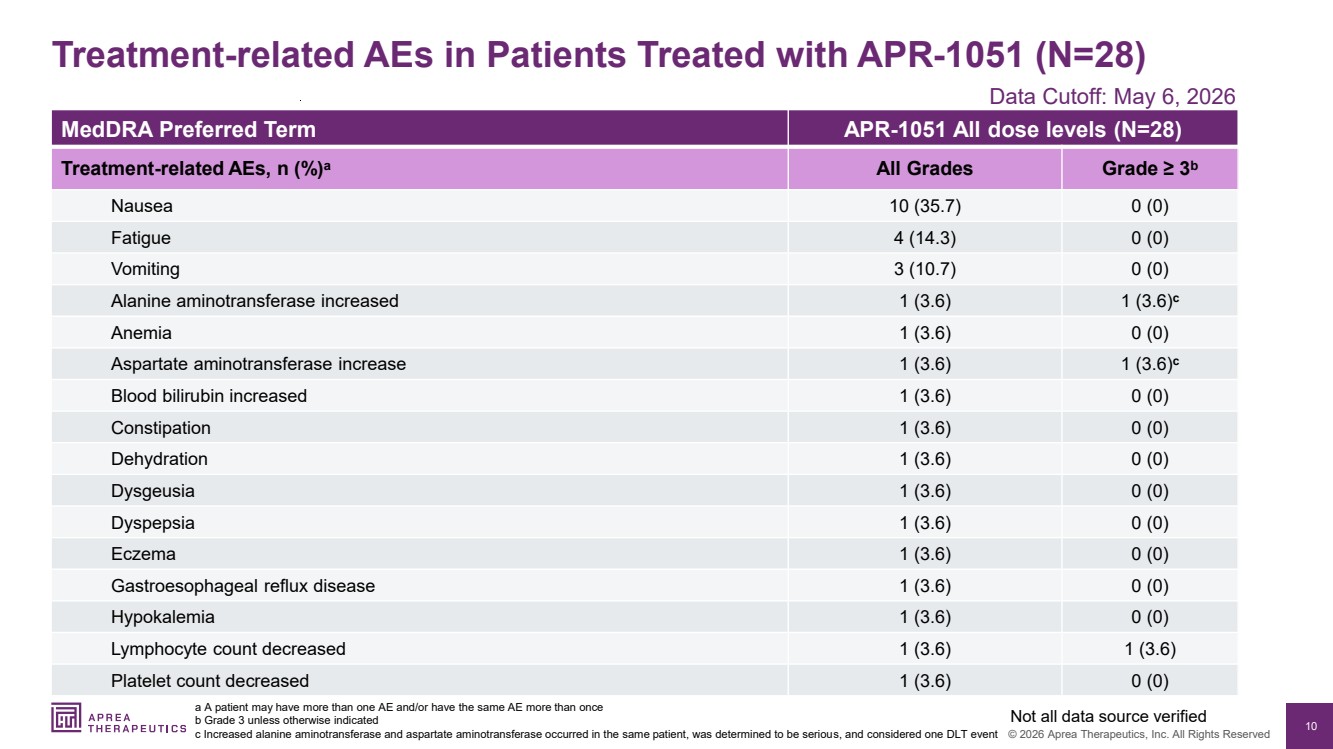
| • | APR-1051 has been shown to be well tolerated; the two most common adverse events have been Grade 1 or 2 nausea and fatigue. No treatment-related class-limiting toxicities, including severe myelosuppression or severe gastrointestinal toxicity, have been observed to date. |
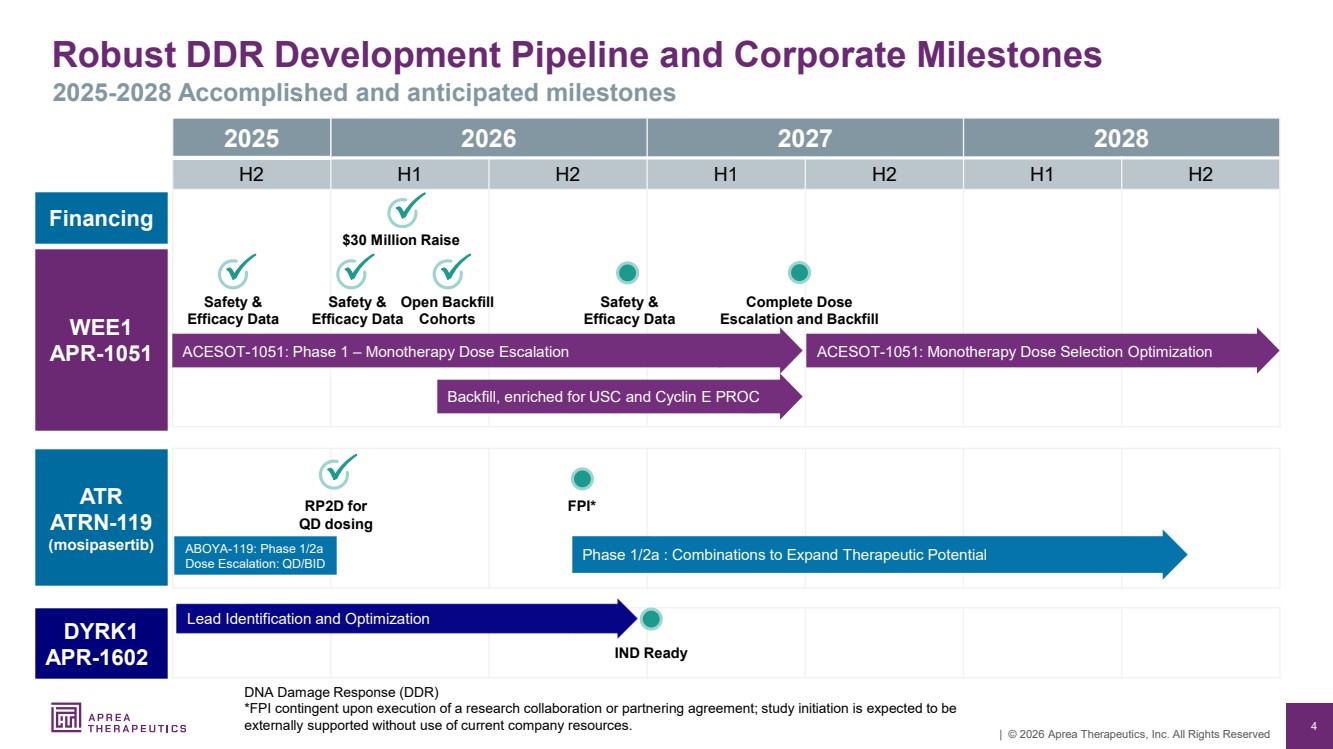
| • | Supported by the $30 million financing that closed on March 31, 2026, Aprea is expanding enrollment in ACESOT-1051 to include at least 50 patients with uterine serous carcinoma (USC), as well as patients with cyclin E-overexpressing, platinum-resistant ovarian cancer (PROC). The expansion is intended to provide additional safety, tolerability and preliminary efficacy data to inform the future clinical path for APR-1051. Completion of dose escalation is anticipated in the second quarter of 2027. |
| • | Further clinical updates from ACESOT-1051 are expected during Q2 2026. An abstract entitled “Early results from the first-in-human phase 1 study of WEE1 inhibitor APR-1051 in patients with advanced solid tumors (ACESOT-1051)” has been accepted for the 2026 American Society of Clinical Oncology (ASCO) Annual Meeting. The poster will be presented on May 30, 2026, 1:30 – 4:30pm CT. |
| • | For more information on ACESOT-1051, refer to ClinicalTrials.gov NCT06260514. |
ABOYA-119: Clinical Trial Evaluating ATR inhibitor, ATRN-119
| • | ATRN-119 is a potent and highly selective first-in-class macrocyclic ATR inhibitor, designed and developed to be used in patients with tumors harboring mutations in DDR-related genes. Cancers with mutations in DDR-related genes represent a high unmet medical need. These patients often have a poor prognosis and currently lack effective therapeutics options. |
| • | During 2025 Aprea established 1,100 mg once daily as the recommended Phase 2 dose (RP2D) in the ABOYA-119 clinical trial. The Company strategically paused further enrollment and has started an orderly wind-down of certain clinical trial site activities associated with the monotherapy, as the Company explores ATRN-119 in potential combination approaches that may unlock greater clinical benefit. The Company is currently in discussions with leading academic institutions to evaluate ATRN-119 in combination with radiation in HPV+ head and neck cancer. Additional investigator-led studies evaluating ATRN-119 with immuno-oncology therapies and antibody-drug conjugates are also being explored. |
| • | For more information on ABOYA-119, please refer to clinicaltrials.gov NCT04905914. |
Corporate
| • | On March 31, 2026, the Company closed an oversubscribed private placement, raising gross proceeds of $30 million. The private placement was led by Soleus Capital with participation from other new investors, including Vestal Point Capital and Squadron Capital Management, existing investors and certain insiders of the Company. Net proceeds will be used for general corporate purposes and research and development expenses, including the addition of more patients with USC (regardless of mutation status) into the ACESOT-1051 study and expansion into cyclin E-overexpressing PROC patients. |
| • | In February 2026, the Company appointed Eugene (Gene) Kennedy, MD, as Chief Medical Advisor. Dr. Kennedy is a highly accomplished physician scientist and biopharmaceutical executive with more than 20 years of experience spanning oncology clinical development, regulatory strategy, and senior corporate leadership across public and private biotechnology companies. |
Select Financial Results for the First Quarter Ended March 31, 2026
As of March 31, 2026, the Company reported cash and cash equivalents of $46.5 million compared to $14.6 million as of December 31, 2025. The Company believes that its cash and cash equivalents as of March 31, 2026 will be sufficient to meet its currently projected operating expenses and capital expenditure requirements into the first quarter of 2028.
For the first quarter ended March 31, 2026, the Company reported an operating loss of $3.4 million, compared to an operating loss of $4.1 million in the first quarter of 2025.
Research and Development (R&D) expenses were $1.6 million for the quarter ended March 31, 2026, compared to $2.5 million for the first quarter of 2025. The decrease in R&D expense was primarily related to a decrease of $0.8 million related to the ABOYA-119 clinical trial to evaluate ATRN-119, our clinical-stage oral small molecule inhibitor of ATR, which was voluntarily paused in October 2025.
General and Administrative (G&A) expenses were $1.8 million for each of the quarters ended March 31, 2026 and 2025.
The Company reported a net loss of $3.3 million or ($0.22) loss per basic share on approximately 14.7 million weighted-average common shares outstanding for the quarter ended March 31, 2026, compared to a net loss of $3.9 million ($0.66) per basic share on approximately 6.0 million weighted average common shares outstanding for the comparable period in 2025.
About Aprea
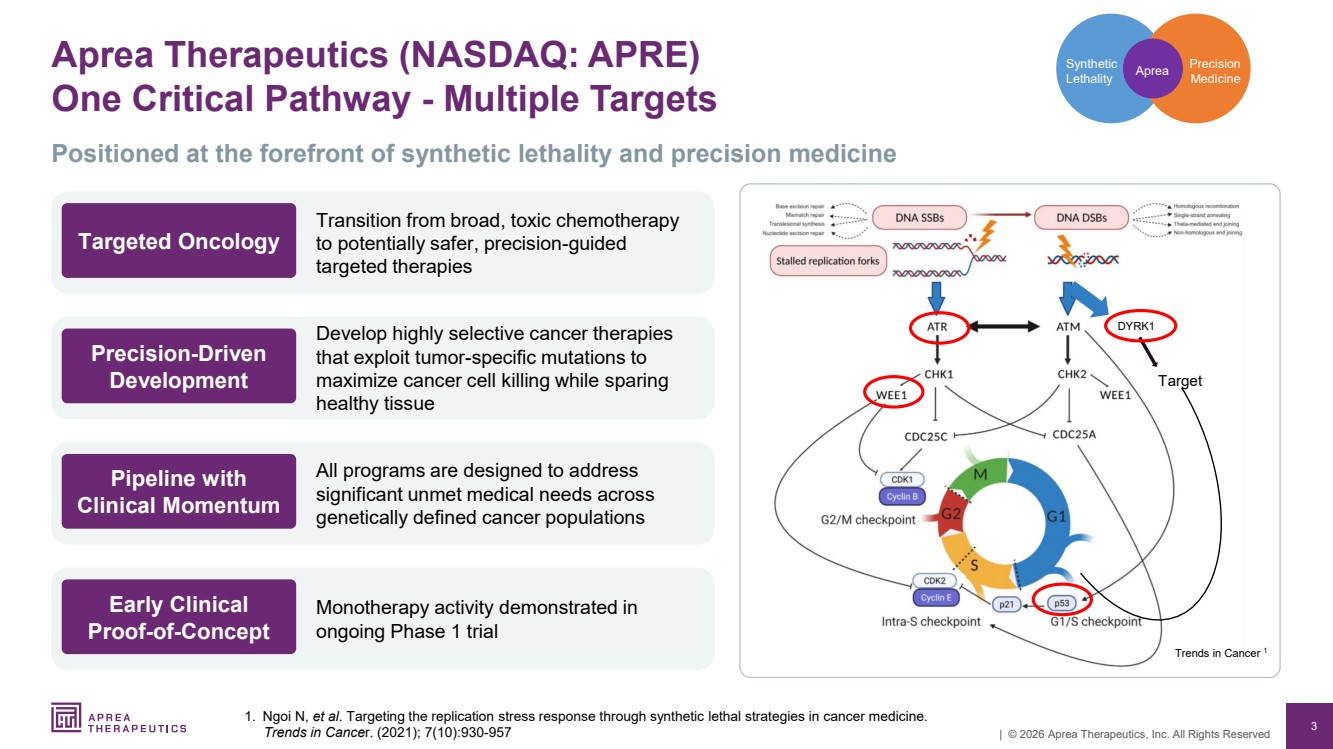
Aprea is a clinical-stage precision medicine oncology company focused on the discovery and development of targeted therapies for patients with biomarker-defined cancers. The Company is pioneering a new approach to treat cancer by exploiting vulnerabilities associated with cancer cell mutations. This approach was developed to kill tumors while minimizing the effect on normal, healthy cells. Aprea’s technology has potential applications across multiple cancer types, enabling it to target a range of tumors, including ovarian, endometrial, colorectal and head and neck squamous cell carcinoma. The Company’s lead programs are APR-1051, an oral, small-molecule inhibitor of WEE1 kinase, and
ATRN-119, a small molecule ATR inhibitor, both in clinical development for solid tumor indications. For more information, please visit the Company website at www.aprea.com.
The Company may use, and intends to use, its investor relations website at https://ir.aprea.com/ as a means of disclosing material nonpublic information and for complying with its disclosure obligations under Regulation FD.
Forward-Looking Statement
Certain information contained in this press release includes “forward-looking statements”, within the meaning of Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended related to our study analyses, clinical trials, regulatory submissions, and projected cash position. We may, in some cases use terms such as “future,” “predicts,” “believes,” “potential,” “continue,” “anticipates,” “estimates,” “expects,” “plans,” “intends,” “targeting,” “confidence,” “may,” “could,” “might,” “likely,” “will,” “should” or other words that convey uncertainty of the future events or outcomes to identify these forward-looking statements. Our forward-looking statements are based on current beliefs and expectations of our management team and on information currently available to management that involve risks, potential changes in circumstances, assumptions, and uncertainties. All statements contained in this press release other than statements of historical fact are forward-looking statements, including statements regarding our ability to develop, commercialize, and achieve market acceptance of our current and planned products and services, our research and development efforts, including timing considerations and other matters regarding our business strategies, use of capital, results of operations and financial position, and plans and objectives for future operations. Any or all of the forward-looking statements may turn out to be wrong or be affected by inaccurate assumptions we might make or by known or unknown risks and uncertainties. These forward-looking statements are subject to risks and uncertainties including, without limitation, risks related to the success, timing, and cost of our ongoing clinical trials and anticipated clinical trials for our current product candidates, including statements regarding the timing of initiation, pace of enrollment and completion of the trials (including our ability to fully fund our disclosed clinical trials, which assumes no material changes to our currently projected expenses), futility analyses, presentations at conferences and data reported in an abstract, and receipt of interim or preliminary results (including, without limitation, any preclinical results or data), which are not necessarily indicative of the final results of our ongoing clinical trials, our understanding of product candidates mechanisms of action and interpretation of preclinical and early clinical results from its clinical development programs, and our ability to predict clinical outcomes based on such preclinical and early clinical results, and the other risks, uncertainties, and other factors described under “Risk Factors,” “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and elsewhere in the documents we file with the U.S. Securities and Exchange Commission. For all these reasons, actual results and developments could be materially different from those expressed in or implied by our forward-looking statements. You are cautioned not to place undue reliance on these forward-looking statements, which are made only as of the date of this press release. We undertake no obligation to update such forward-looking statements for any reason, except as required by law.
Aprea Therapeutics, Inc. | ||||||
Consolidated Balance Sheets | ||||||
| March 31, 2026 | | December 31, 2025 | |||
Assets |
| (unaudited) |
|
| ||
Current assets: |
|
|
|
| ||
Cash and cash equivalents | $ | 46,466,202 | $ | 14,599,347 | ||
Prepaid expenses and other current assets |
| 779,238 |
| 961,899 | ||
Total current assets |
| 47,245,440 |
| 15,561,246 | ||
Property and equipment, net |
| 54,379 | 59,807 | |||
Restricted cash |
| 41,406 | 41,186 | |||
Other noncurrent assets |
| 271,162 |
| 271,162 | ||
Total assets | $ | 47,612,387 | $ | 15,933,401 | ||
Liabilities and Stockholders’ Equity |
|
|
|
| ||
Current liabilities: |
|
|
|
| ||
Accounts payable | $ | 2,940,756 | $ | 713,668 | ||
Accrued expenses | 2,355,890 | 2,050,690 | ||||
Total current liabilities |
| 5,296,646 |
| 2,764,358 | ||
Commitments and contingencies |
|
|
|
| ||
Series A convertible preferred stock, $0.001 par value, 40,000,000 shares authorized; 31,194 shares issued and outstanding at March 31, 2026 and December 31, 2025 |
| 727,361 |
| 727,361 | ||
Stockholders’ equity: |
|
|
|
| ||
Common stock, $0.001 par value, 400,000,000 shares authorized, 11,982,776 and 8,192,538 shares issued and outstanding at March 31, 2026 and December 31, 2025, respectively |
| 11,983 |
| 8,192 | ||
Additional paid-in capital |
| 389,631,454 |
| 356,709,645 | ||
Subscription Receivable | (499,999) |
| — | |||
Accumulated other comprehensive loss |
| (10,625,700) |
| (10,634,714) | ||
Accumulated deficit |
| (336,929,358) |
| (333,641,441) | ||
Total stockholders’ equity |
| 41,588,380 |
| 12,441,682 | ||
Total liabilities and stockholders' equity | $ | 47,612,387 | $ | 15,933,401 | ||
Aprea Therapeutics, Inc. | ||||||
Consolidated Statements of Operations and Comprehensive Loss | ||||||
(Unaudited) | ||||||
Three Months Ended March 31, | ||||||
| 2026 | | 2025 | |||
Grant revenue |
| $ | — | $ | 162,463 | |
Operating expenses: |
|
|
|
| ||
Research and development | 1,611,167 | 2,483,066 | ||||
General and administrative |
| 1,819,245 |
| 1,764,979 | ||
Total operating expenses |
| 3,430,412 |
| 4,248,045 | ||
Loss from operations |
| (3,430,412) |
| (4,085,582) | ||
Other income (expense): |
|
| ||||
Interest income, net |
| 134,784 | 204,726 | |||
Foreign currency gain (loss) |
| 7,711 |
| (51,803) | ||
Total other income |
| 142,495 |
| 152,923 | ||
Net loss | $ | (3,287,917) | $ | (3,932,659) | ||
Other comprehensive loss: |
|
| ||||
Foreign currency translation |
| 9,014 |
| 643 | ||
Total comprehensive loss | $ | (3,278,903) | $ | (3,932,016) | ||
Net loss per share attributable to common stockholders, basic and diluted | $ | (0.22) | $ | (0.66) | ||
Weighted-average common shares outstanding, basic and diluted |
| 14,685,448 |
| 5,993,866 | ||