Exhibit 99.1

AtaiBeckley Announces Positive Topline Results from an Exploratory Phase 2a Trial of EMP-01 (oral R-MDMA) in Social Anxiety Disorder
| • |
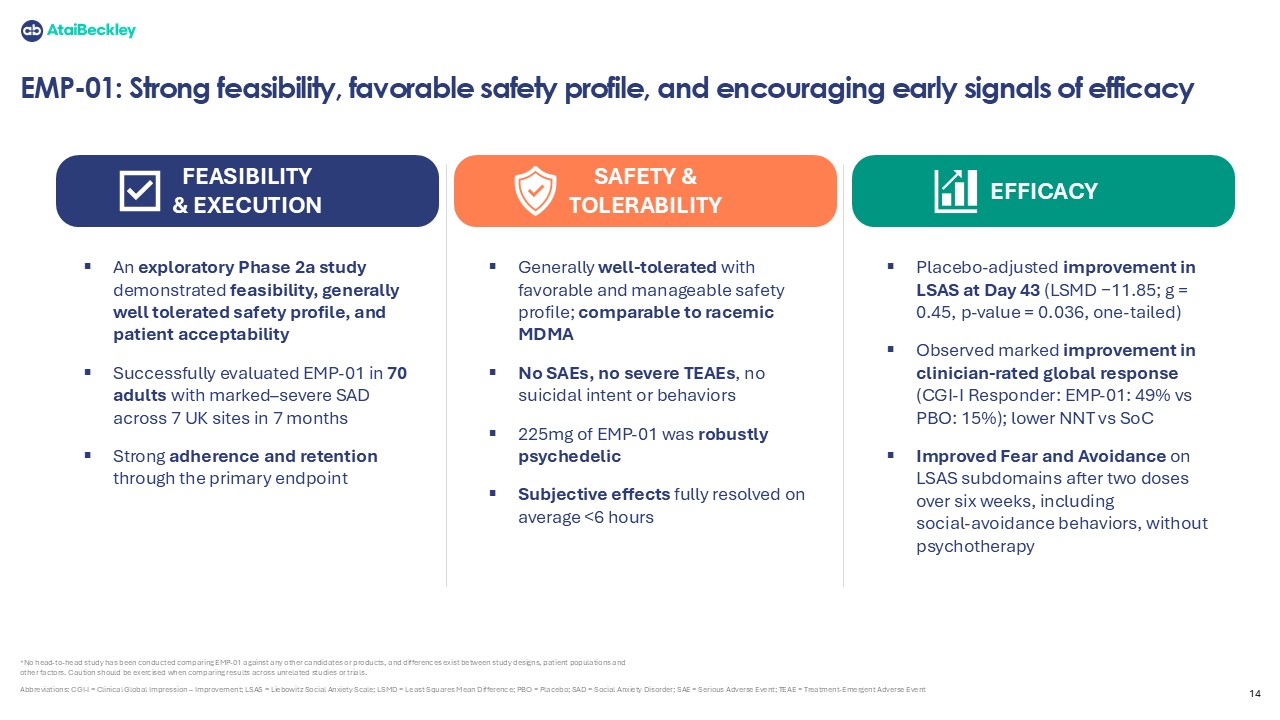
EMP-01 met its primary objective on safety and tolerability, demonstrating a generally favorable and manageable safety and tolerability profile
|
| • |
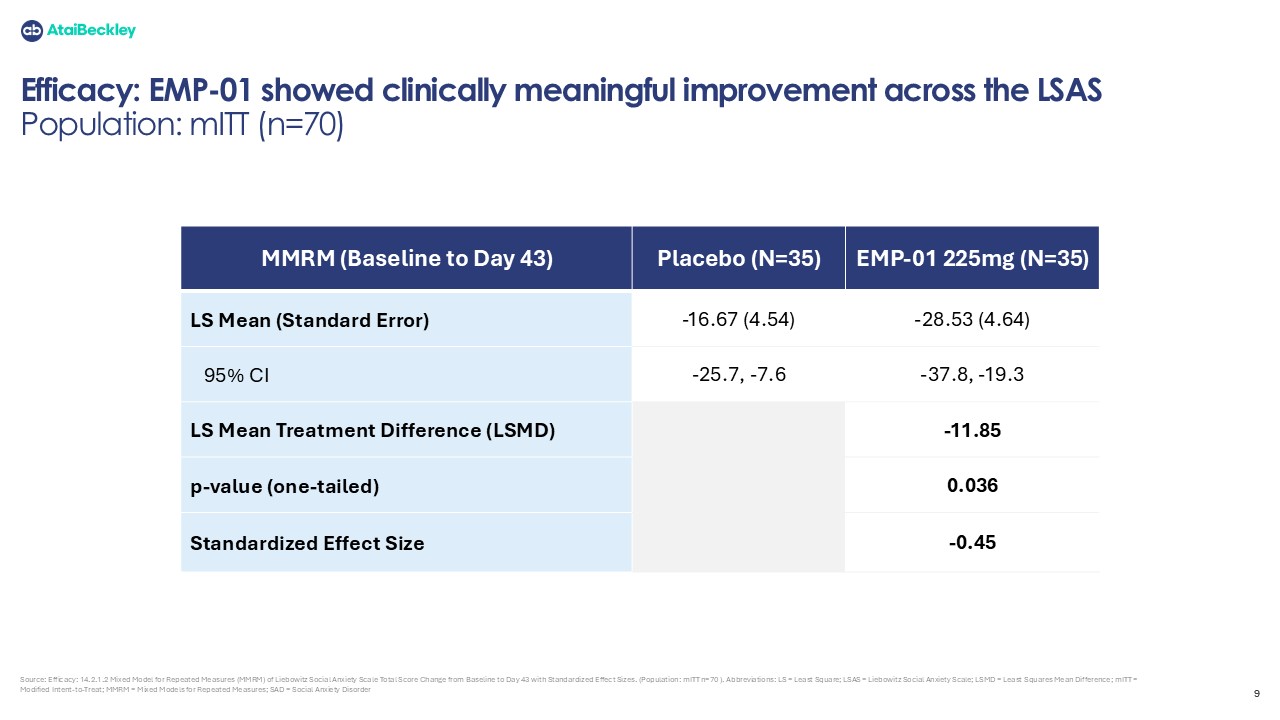
EMP-01 demonstrated a clinically meaningful placebo-adjusted least squares mean reduction of 11.85 points on the Liebowitz Social Anxiety Scale (LSAS) at Day 43 (Hedges’ g = 0.45; p-value = 0.036, one-tailed)
|
| • |
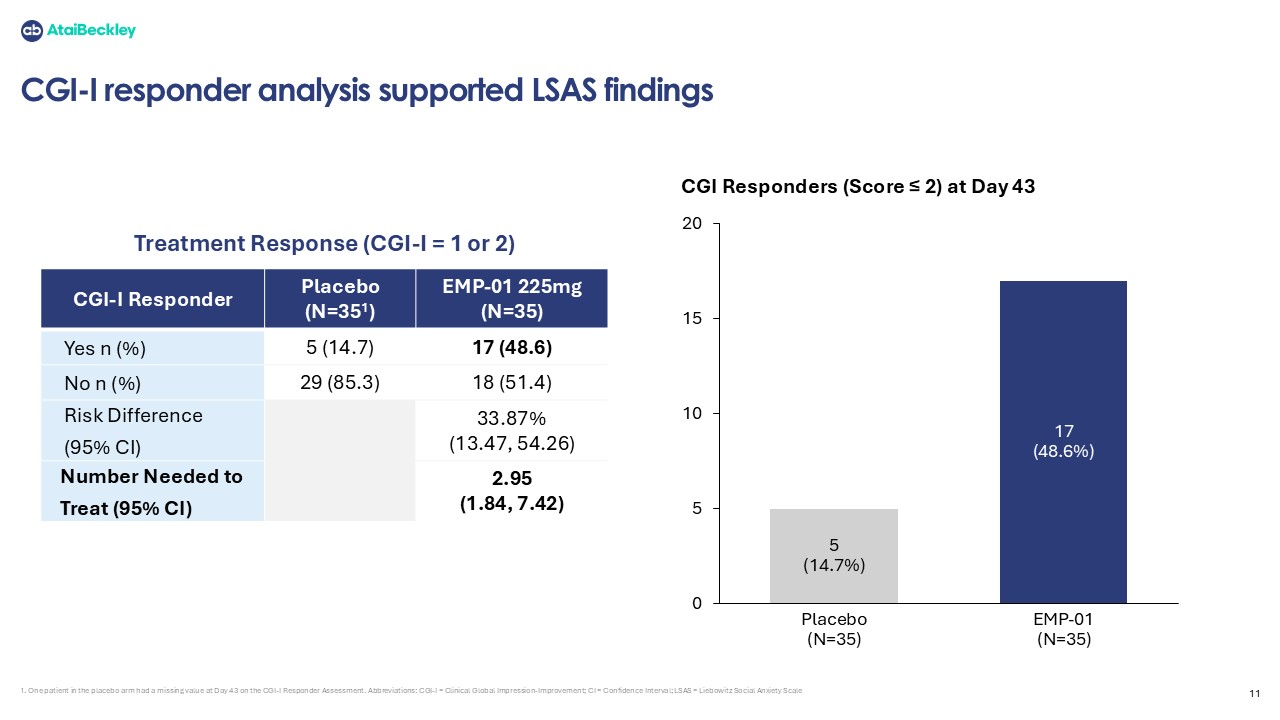
EMP-01 demonstrated a robust separation from placebo on the Clinician Global Impression–Improvement (CGI-I) assessment: 49% responders vs. 15% for placebo, corresponding to a Number Needed to Treat (NNT) of 2.95
|
| • |
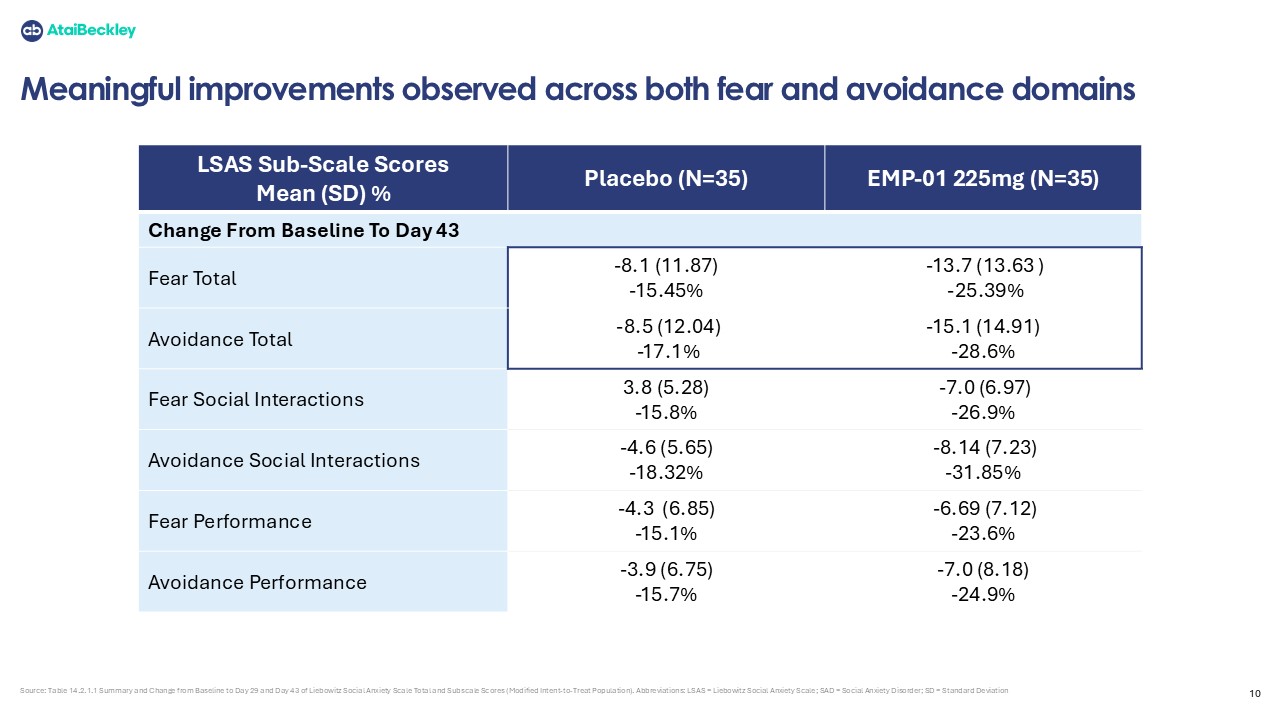
EMP-01 demonstrated improvements across both Fear and Avoidance sub-domains of the LSAS, including improvement in social avoidance behaviors after two administrations over six weeks, and without adjunctive psychotherapy
|
| • |
More detailed analyses of the data will be described in upcoming scientific venues and will guide subsequent development
|
| • |
Conference call scheduled for 8:00 a.m. ET today, February 26, 2026
|
NEW YORK, UNITED STATES – FEBRUARY 26, 2026 - AtaiBeckley Inc. (NASDAQ: ATAI) (“AtaiBeckley” or the “Company”), a clinical‑stage biotechnology company on a mission to transform patient outcomes by developing rapid‑acting, durable and convenient treatments for mental
health conditions, today announced topline results from its exploratory, double‑blind, placebo‑controlled, first-in-patient Phase 2a study (NCT06693609) evaluating EMP‑01 (oral R‑MDMA) in adults with Social Anxiety Disorder (SAD). The study
met its primary safety objective and generated encouraging secondary and exploratory efficacy signals in a highly severe, difficult‑to‑treat
population.
Commenting on the results, Professor Murray Stein, Distinguished Professor of Psychiatry and Public Health at the University of California San Diego
(UCSD), and consultant to AtaiBeckley, said: “The initial findings from this trial of R-MDMA (EMP-01) are remarkable. Social Anxiety Disorder is a serious, often chronic and disabling
condition affecting millions of Americans, and there have been no therapeutic advances in its pharmacological treatment in over 20 years. While preliminary, this study suggests that EMP-01 has the potential to make a tremendous impact on the lives
of patients and their families. I hope future trials will be conducted to confirm these very exciting findings.”
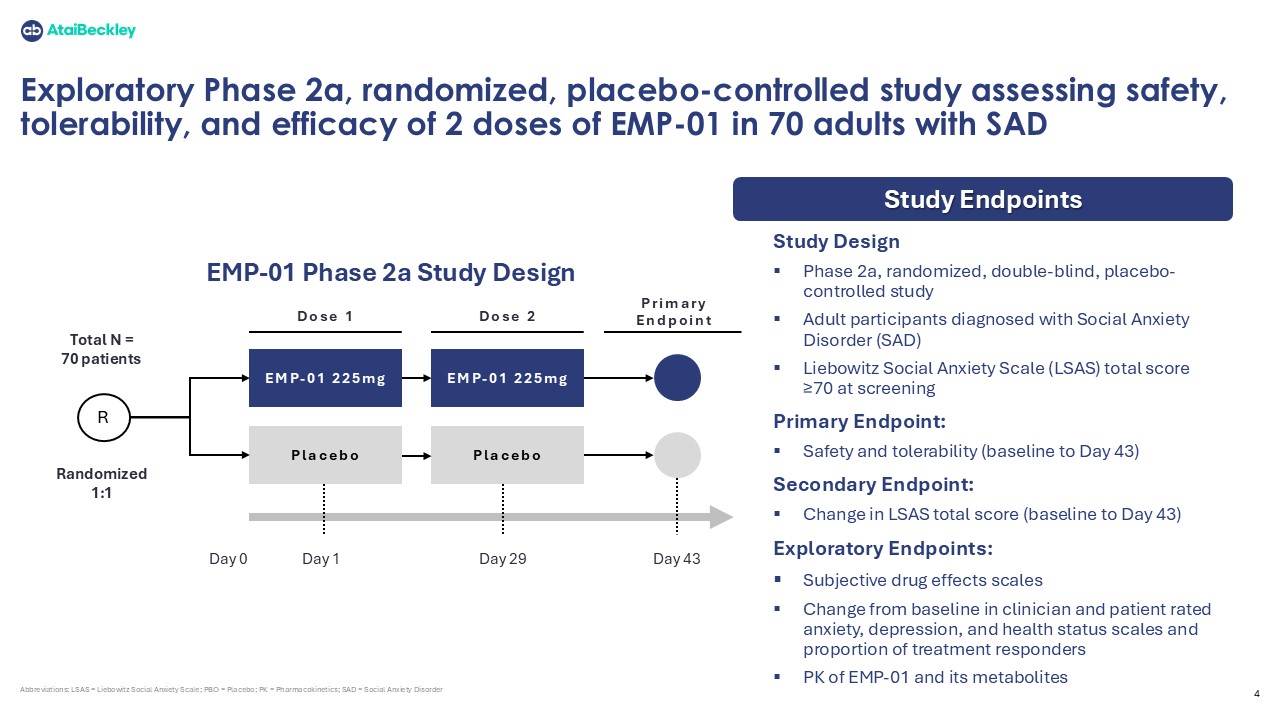
The
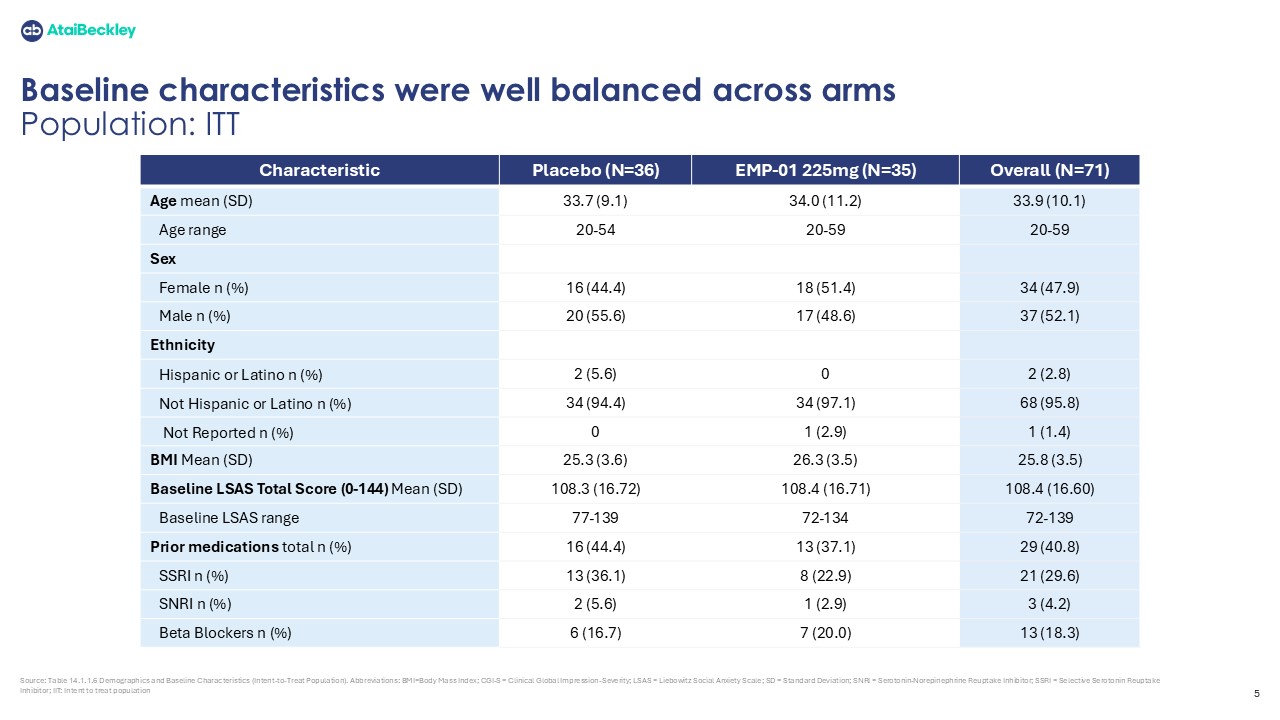
multi-center study enrolled 71 adults with moderate-to-severe SAD across 7 clinical sites in the UK. Participants were randomized to receive two in-clinic administrations of EMP-01 (225 mg) or placebo, given 28 days apart, with no adjunctive
psychotherapy. 70 participants received at least one dose of study drug, and 69 completed the Day 43 efficacy assessments, indicating high patient acceptability and retention. All clinician-rated assessments were conducted by blinded central
raters.
Both treatment
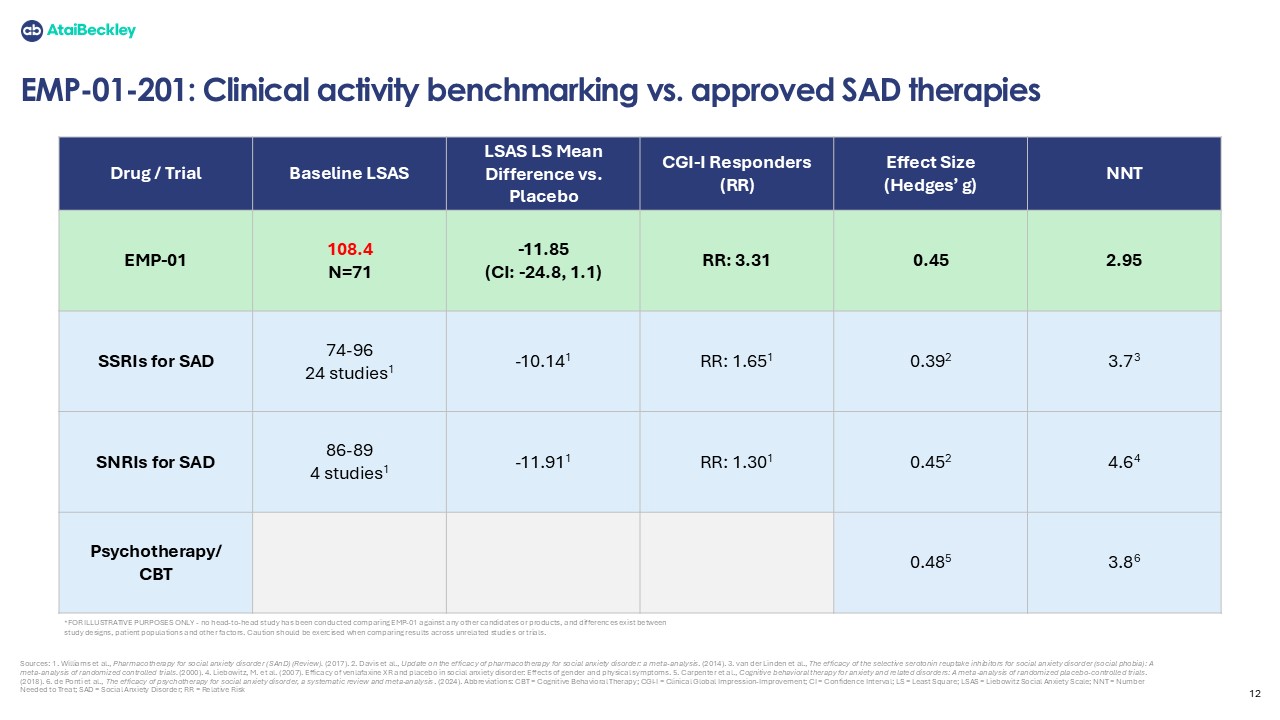
arms reflected a severely affected patient population (~108 baseline LSAS score out of a maximum of 144), with all other baseline characteristics well-balanced across groups including demographics, comorbidities, prior SSRI/SNRI exposure, and
CGI-Severity. The primary endpoint was safety and tolerability through Day 43 and the secondary endpoint was change in social anxiety symptoms from baseline to Day 43, using the Liebowitz Social Anxiety Scale (LSAS). The LSAS is a 24-item
clinician-rated scale that evaluates both fear responses and real-world avoidance behaviors across social and performance situations. An additional exploratory endpoint included changes on the Clinician-Rated Global Impression-Improvement (CGI-I)
scale, a 7-point scale used to measure changes in a patient’s overall condition compared to baseline.
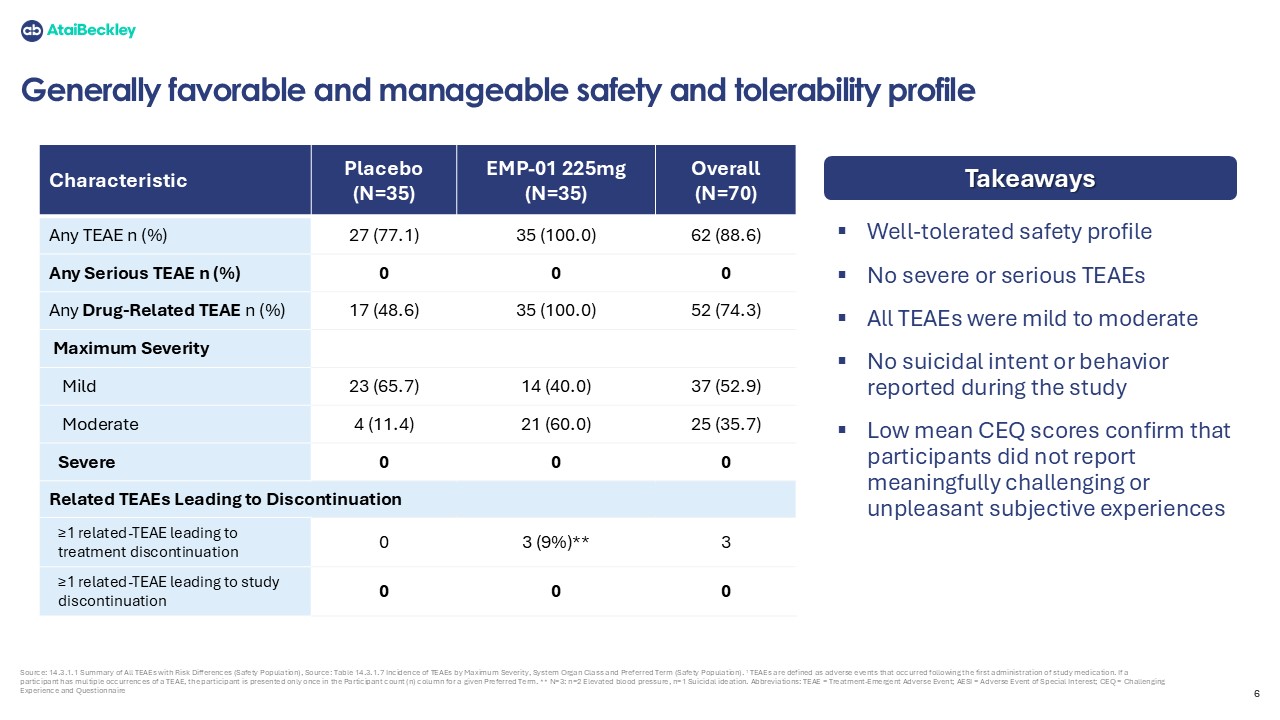
With respect to the trial’s primary objective, EMP-01 demonstrated a favorable and manageable safety and tolerability profile. No serious adverse events and no
treatment-emergent suicidal behaviour or intent were observed. Most adverse events were mild or moderate and resolved without intervention.
Secondary and exploratory efficacy endpoints showed encouraging signals. EMP-01 produced a numerically greater symptom reduction than placebo, as measured by LSAS, at Day 43 relative to baseline (least squares mean:
-28.53 points vs. -16.67 points, respectively). Although the study was not powered for statistical significance, the placebo-adjusted least squares mean reduction for EMP-01 of 11.85 points on the LSAS at Day 43 (Hedges’ g = 0.45; p-value = 0.036,
one-tailed) is consistent with a clinically meaningful improvement and a moderate treatment effect size. The relatively early reduction in symptoms, as measured by LSAS, at the 6-week study endpoint, after two doses of EMP-01, was comparable in
magnitude in a cross-trial comparison to that typically reported after 8 - 12 weeks of daily SSRI/SNRI therapy in registration trials.
On the CGI-I scale, which reflects a global impression of overall patient improvement, 49% of patients receiving EMP-01 were rated as “very much
improved” or “much improved” compared to 15% in the placebo group. This 34-percentage-point difference corresponds to a Number Needed to Treat (NNT) of 2.95 (95% CI: 1.84, 7.42), indicating a clinically meaningful level of global improvement in the
EMP-01 group.
The LSAS
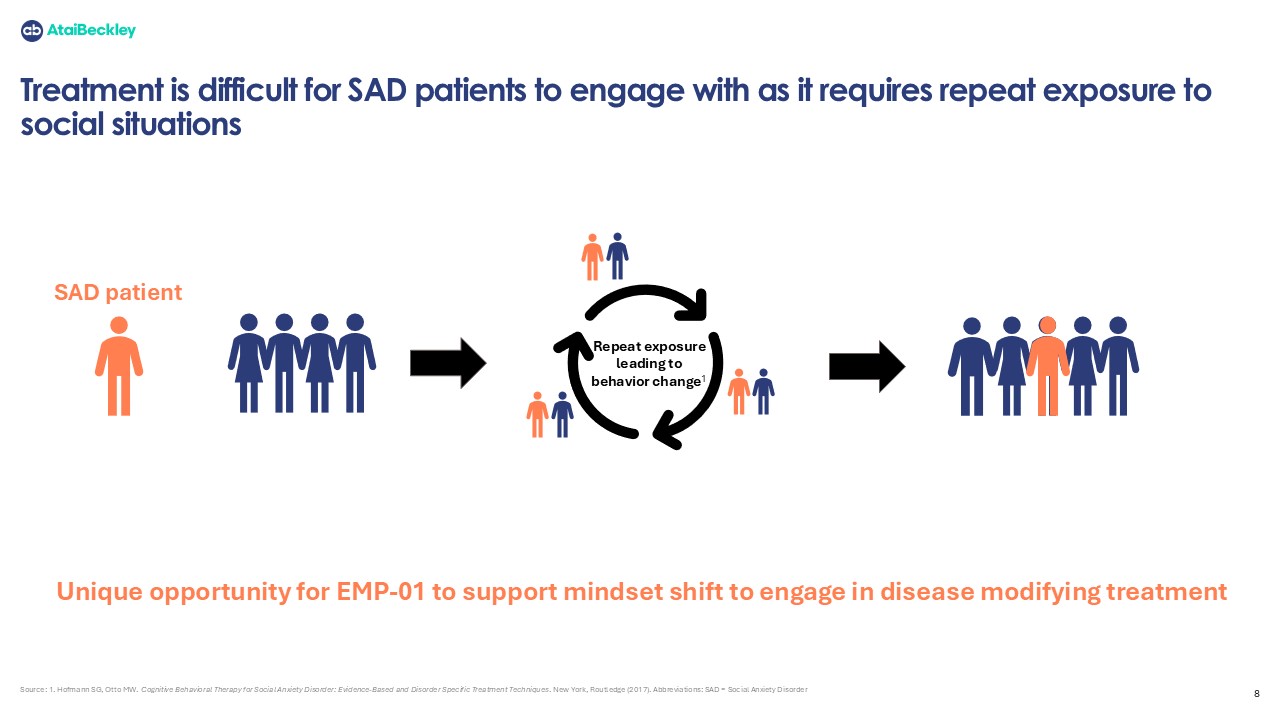
comprises two subscales - Fear and Avoidance - which often show different timelines of improvement in SAD pharmacotherapy trials, with Fear typically improving first. In this study, EMP‑01 produced simultaneous gains across both domains. By Day 43,
LSAS Fear improved by −13.7 points (−25.4%) vs. −8.1 (−15.5%) on placebo, and LSAS Avoidance improved by −15.1 points (−28.6%) vs. −8.5 (−17.1%) on placebo. Because avoidance behaviors typically change gradually and often require prolonged
real‑world exposure, the early, parallel improvements in both Fear and Avoidance - after two dosing sessions and without psychotherapy - suggest that EMP‑01 could influence both the emotional and behavioral dimensions of social anxiety disorder.
Dr. David Feifel, Professor Emeritus of Psychiatry at the University of California, San Diego, Founder and President of the Kadima Neuropsychiatry
Institute, and consultant to AtaiBeckley, said, "Several findings from this preliminary study are highly encouraging, particularly that LSAS improvements became apparent after dosing
was completed and the drug was no longer present, suggesting a sustained biological therapeutic effect. If confirmed in larger trials, this would represent a meaningful departure from current first-line pharmacotherapies like SSRIs, which require
continuous daily dosing and frequently produce tolerability concerns. An intervention delivering durable symptom improvement with intermittent drug exposure would be a potentially transformative development for patients with this disorder.”
“We are
encouraged by both the strength of the signal and our ability to deliver the topline results from this exploratory Phase 2a study on time and with a robust dataset,” said Srinivas Rao, Chief Executive Officer and Co-Founder of AtaiBeckley. “As the
first patient trial of R-MDMA in Social Anxiety Disorder, this study demonstrated our ability to rapidly enroll a highly severe population, deliver two in-clinic administrations with strong adherence, and maintain exceptional retention of patients
through the primary endpoint assessment. The consistent pattern of improvement observed across secondary and exploratory efficacy endpoints, together with a generally favorable safety and tolerability profile, provides meaningful validation of both
the compound and our clinical development model as we assess the next phase of advancement. We are very grateful to the patients who participated in this trial and to the investigators and site teams whose high-quality trial execution made these
insights possible.”
Conference Call
AtaiBeckley will host a conference call and live webcast today February 26, 2026, at 8:00 a.m. ET. The conference call can be accessed by dialing (800)
715-9871 for participants in the US and +1-646-307-1963 for international callers, with the Conference ID: 1459387. The webcast and presentation can be accessed on the Investors section of AtaiBeckley’s corporate website under Events. The
presentation and an archived replay of the webcast will be available in the same section of the website for a minimum of 30 days following the event.
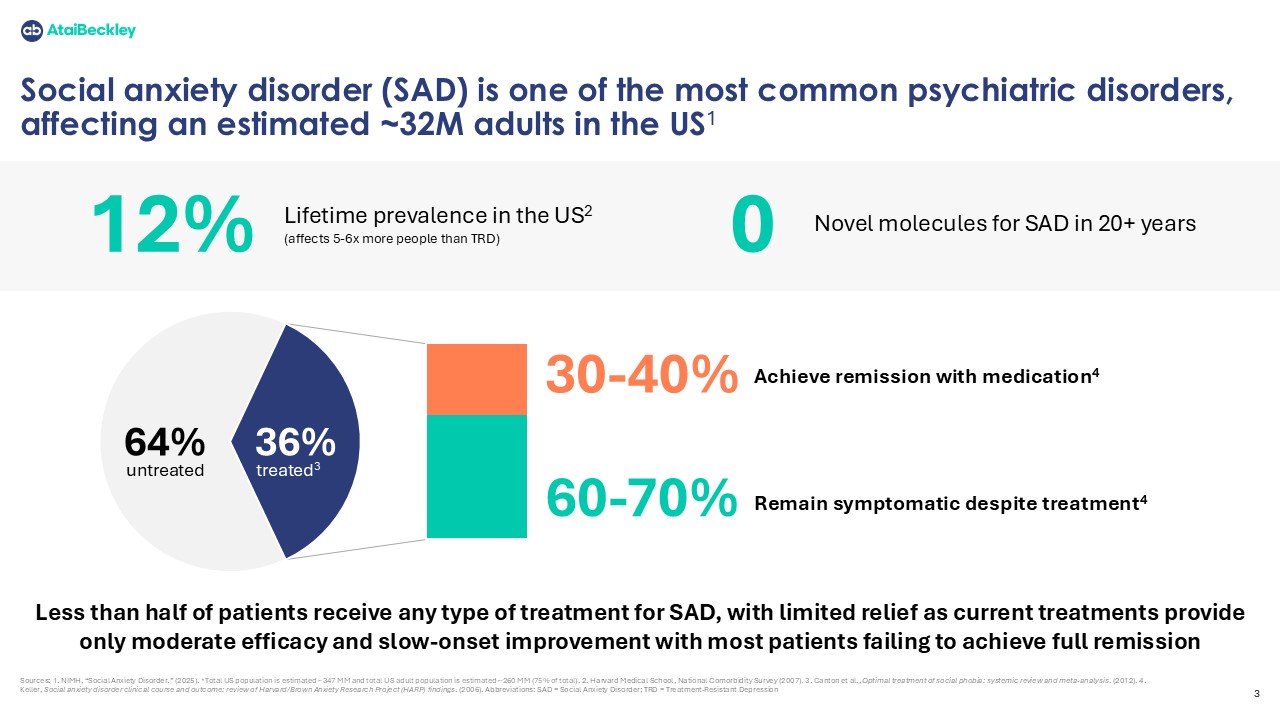
About Social Anxiety Disorder (SAD)
Social Anxiety Disorder (SAD) is one of the most prevalent psychiatric conditions worldwide, affecting an estimated 400–800 million individuals with a
lifetime prevalence of approximately 12%. The disorder is characterized by persistent and debilitating fear, self-consciousness, and heightened anxiety during social interactions. SAD is frequently co-morbid with major depressive disorder,
generalized anxiety disorder, obsessive–compulsive disorder, attention deficit/hyperactivity disorder, bipolar disorder, and substance use disorders, contributing to substantial functional impairment and reduced quality of life. In the United States
alone, roughly 30 million adults are affected by SAD; however, only about 50% of affected individuals receive treatment. Even among patients who access care, treatment adequacy remains suboptimal, and around 50% of SAD patients do not achieve
adequate response to first line therapies and often deal with chronic medication side effects.
About EMP-01 (Oral R-MDMA)
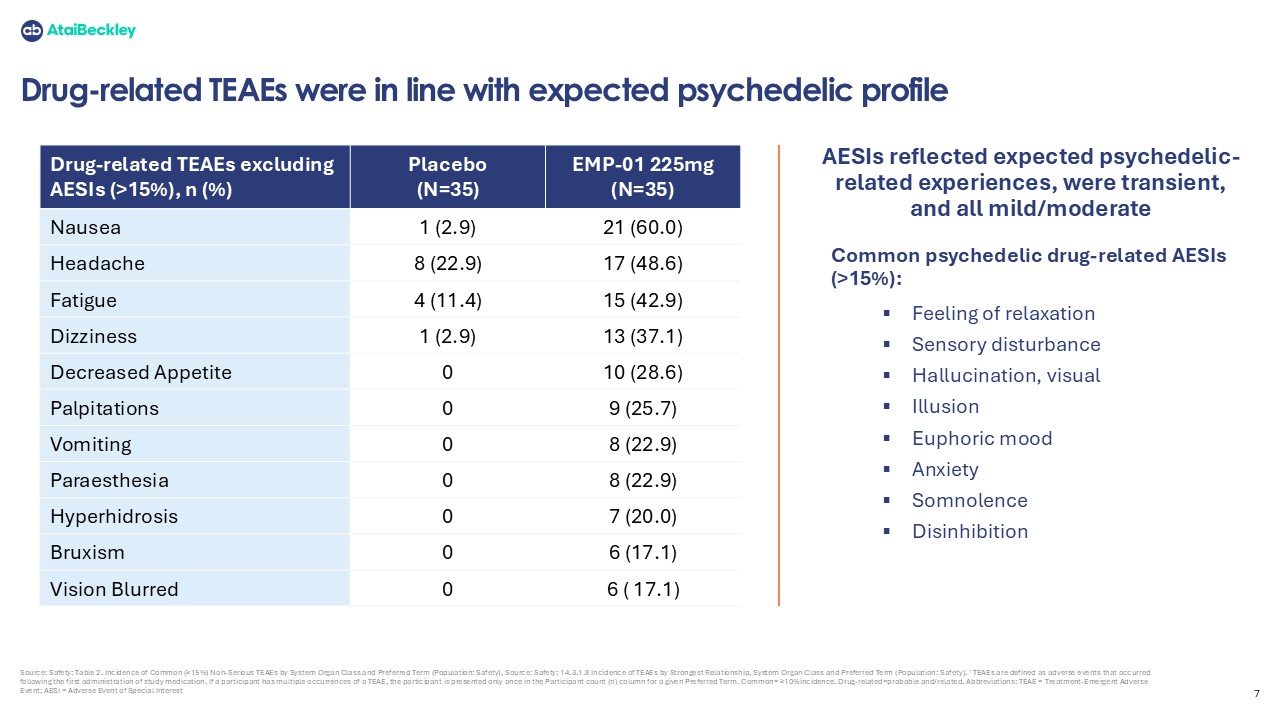
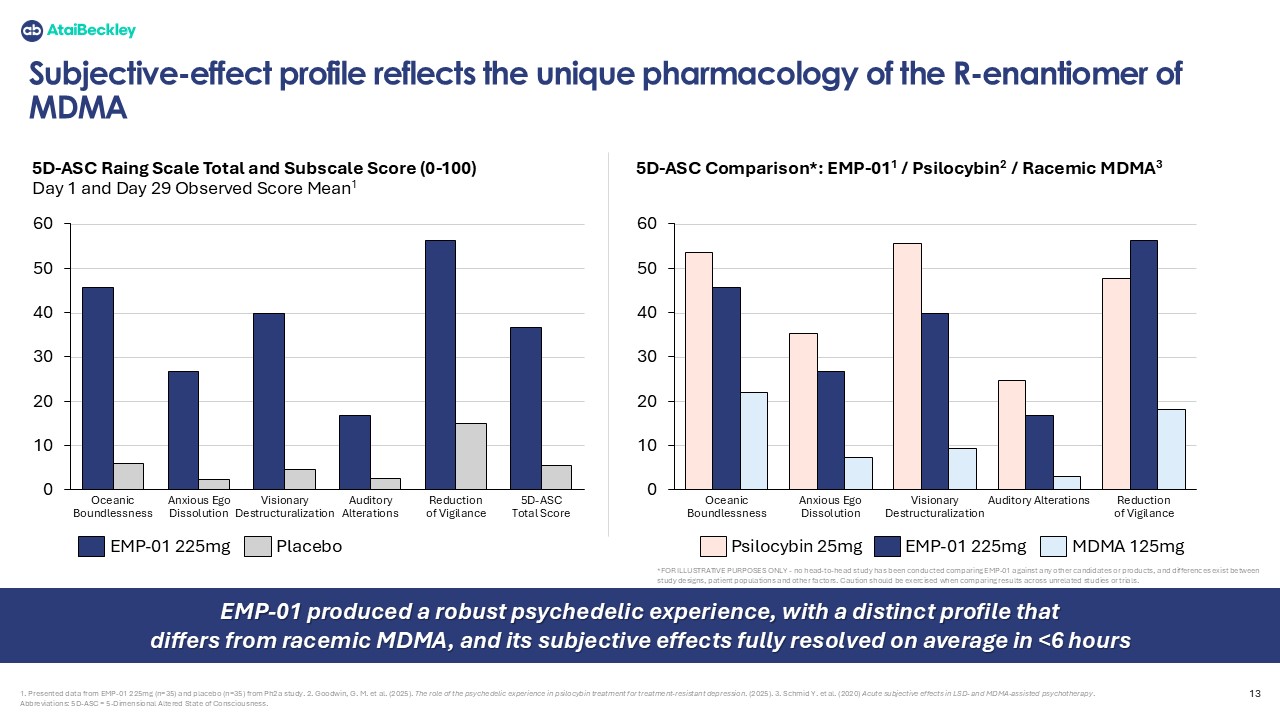
EMP-01 is an oral, single-enantiomer R‑MDMA candidate being developed as a potential treatment for people living with Social Anxiety Disorder (SAD). It has
been designed to elicit entactogenic and psychedelic subjective effects, with reduced dopaminergic and noradrenergic activity compared with racemic MDMA in order to support safe, scalable outpatient administration for individuals with SAD, who
currently have a high unmet medical treatment need. EMP-01 is an investigational product and has not been approved by the FDA.
About AtaiBeckley
Inc.
AtaiBeckley is a clinical-stage
biotechnology company on a mission to transform patient outcomes by developing rapid-acting, durable and convenient mental health treatments. AtaiBeckley’s pipeline of novel investigational therapies includes BPL-003 (mebufotenin benzoate nasal
spray) for treatment-resistant depression (TRD), VLS-01 (DMT buccal film) for TRD and EMP-01 ((R)-MDMA HCI) for social anxiety disorder. BPL-003 is in Phase 3 planning, VLS-01 and EMP-01 are in Phase 2 clinical development. The Company is also
advancing a drug discovery program to identify novel, non-hallucinogenic 5-HT2AR agonists for opioid use disorder and TRD. These programs aim to create breakthroughs in mental health through transformative interventional psychiatry therapies that can
integrate seamlessly into healthcare systems.
For the latest updates and to learn
more about the AtaiBeckley mission, visit www.ataibeckley.com or follow the Company on LinkedIn and on X.
Forward-Looking Statements
This press release contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995, as amended. We intend such forward-looking
statements to be covered by the safe harbor provisions for forward-looking statements contained in Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended. The words “believe,”
“may,” “will,” “estimate,” “continue,” “anticipate,” “intend,” “expect,” “anticipate,” “initiate,” “could,” “would,” “project,” “plan,” “potentially,” “preliminary,” “likely,” and similar expressions are intended to identify forward-looking
statements, although not all forward-looking statements contain these words. Forward-looking statements include express or implied statements relating to, among other things: our business strategy and plans; progress and results of our EMP-01
trials; the timing of further data on EMP-01; the therapeutic potential of EMP-01; and the potential benefits of EMP-01 for patients with SAD. Additionally, topline results AtaiBeckley reports is based on preliminary analysis of key efficacy and safety data, and such data may
change following a more comprehensive review of the data related to the clinical trial and such topline data may not accurately reflect the complete results of a clinical trial.
Forward-looking statements are neither promises nor guarantees, but involve known and unknown risks and uncertainties that could cause actual results to differ
materially from those projected, including, without limitation, the important factors described in the section titled “Risk Factors” in Atai Beckley N.V.’s our most recent Annual Report on Form 10-K or Quarterly Reports on Form 10-Q filed with
the Securities and Exchange Commission (“SEC”), as such factors may be updated from time to time in AtaiBeckley’s other filings with the SEC. AtaiBeckley disclaims any obligation to update or revise any forward-looking statements contained in
this press release, other than to the extent required by applicable law.
Contact Information:
Investors:
Jason Awe, PhD
VP, Investor Relations
Media:
Charlotte Chorley
Associate Director, Communications