JULY 29, 2025 CRDF-004 Trial Update 1st Line RAS-mutated mCRC

Forward-looking statements Certain statements in this presentation are forward-looking within the meaning of the Private Securities Litigation Reform Act of 1995. These statements may be identified by the use of words such as "anticipate," "believe," "forecast," "estimated" and "intend" or other similar terms or expressions that concern our expectations, strategy, plans or intentions. These forward-looking statements are based on our current expectations and actual results could differ materially. There are several factors that could cause actual events to differ materially from those indicated by such forward-looking statements. These factors include, but are not limited to, clinical trials involve a lengthy and expensive process with an uncertain outcome, and results of earlier studies and trials may not be predictive of future trial results; our clinical trials may be suspended or discontinued due to unexpected side effects or other safety risks that could preclude approval of our product candidate; results of preclinical studies or clinical trials for our product candidate could be unfavorable or delayed; our need for additional financing; risks related to business interruptions, including the outbreak of COVID-19 coronavirus and cyber-attacks on our information technology infrastructure, which could seriously harm our financial condition and increase our costs and expenses; uncertainties of government or third party payer reimbursement; dependence on key personnel; limited experience in marketing and sales; substantial competition; uncertainties of patent protection and litigation; dependence upon third parties; and risks related to failure to obtain FDA clearances or approvals and noncompliance with FDA regulations. There are no guarantees that our product candidate will be utilized or prove to be commercially successful. Additionally, there are no guarantees that future clinical trials will be completed or successful or that our product candidate will receive regulatory approval for any indication or prove to be commercially successful. Investors should read the risk factors set forth in our Form 10-K for the year ended December 31, 2024, and other periodic reports filed with the Securities and Exchange Commission. While the list of factors presented here is considered representative, no such list should be considered to be a complete statement of all potential risks and uncertainties. Unlisted factors may present significant additional obstacles to the realization of forward-looking statements. Forward-looking statements included herein are made as of the date hereof, and we do not undertake any obligation to update publicly such statements to reflect subsequent events or circumstances.

Mark Erlander, PhD Chief Executive Officer

Onvansertib specifically targets PLK1, a well-established cancer target Onvansertib First oral, well-tolerated PLK1-selective inhibitor ENZYME IC50 (µM) PLK1 0.002 PLK2 >10.000 PLK3 >10.000 CK2 0.400 FLT3 0.400 CDK1/CycB >10.000 42 other kinases�and >140 in the Millipore panel >10.000 Exquisitely specific for PLK1 SPECIFICITY PROPERTIES Small molecule Oral dosing 24-hour half-life

We designed the CRDF-004 trial to address four objectives 2024 2025 CRDF-004 Ph2 trial�RAS-mut mCRC shift from�2nd line to 1st line Aug 7, 2023 INTENT 1. Select a Ph3 dose – per FDA’s Project Optimus 2. Assess efficacy signal 3. Characterize safety profile in 1st line setting 4. Basis for meeting with FDA to agree Ph3 trial 2023 mCRC, metastatic colorectal cancer; mut, mutated

Dr. Sidhu brings a wealth of clinical development experience Dr. Sidhu served as Executive Vice President and Chief Medical Officer at Roivant Sciences. He was also the Chief Medical Officer at Eterna Therapeutics, Inc. and Cell Design Labs, up until its acquisition by the Gilead subsidiary Kite, where he subsequently served as VP, Clinical Development. He was most recently the Chief Medical Officer and acting CEO at Treadwell Therapeutics. Dr. Sidhu is a Fellow of the Royal College of Physicians and Surgeons of Canada in both internal medicine and medical oncology. He earned his medical degree from Queen’s University in Kingston, Ontario Canada and his bachelor’s degree in biochemistry from the University of Alberta in Edmonton, Alberta. Dr. Sidhu trained in internal medicine at Queen’s University and medical oncology at the British Columbia Cancer Agency in Vancouver, British Columbia and the Cross Cancer Institute in Edmonton, Alberta. CAREER Deep Expertise in mCRC �and Drug Development PRACTICAL EXPERIENCE AT AMGEN Advanced multiple therapeutic candidates in oncology and hematology Led multiple Ph3 clinical trials of panitumumab (Vectibix®, approved US and globally) Dr. Sidhu is a leader in advancing RAS biology and therapeutics in mCRC, with publications in peer-reviewed journals, including the New England Journal of Medicine. A LEADER IN mCRC RAS BIOLOGY

Roger Sidhu, MD Chief Medical Officer

ORR efficacy and safety PFS analyses Registrational program path forward AGENDA 1st line RAS-mut mCRC program update mCRC, metastatic colorectal cancer; Mut, mutant; ORR, objective response rate; PFS, progression free survival

CRC: High unmet need with limited therapies for RAS-mut mCRC COLORECTAL CANCER 3rd most common cancer worldwide 150,000 Annually in the United States new cases 50,000 deaths 15% 5-year relative OS Less than 12 months Median PFS For patients with metastatic CRC 1st LINE STANDARD of CARE RAS-mutated mCRC 1990 2000 2010 2020 1996 FOLFOX 2002 FOLFIRI 2004 Bevacizumab�(Avastin®) Morris et al., J Clin Oncol 2023, Shi et al., J Clin Oncol 2025. CRC, colorectal cancer; mCRC, metastatic colorectal cancer; mut, mutant; OS, overall survival; PFS, progression free survival 2014 FOLFOXIRI

Prior 1st line Ph3 mCRC trials provide benchmarks for current SoC Targeted agent Trial Mechanism of action Trial population Sample size ORR Exp. vs Ctrl. ORR delta PFS (months) Exp. vs Ctrl. Hazard�ratio Bevacizumab IFL/bev vs IFL Antiangiogenic KRAS WT or mutant All ITT patients Mutant only1 813 78 45% vs 35% 43% vs 41% 10% 2% 10.6 vs 6.2 9.3 vs 5.5 0.54 p<0.0001 0.41 FOLFOXIRI/bev (TRIBE trial) FOLFOXIRI/bev�vs FOLFIRI/bev Chemo RAS WT or mutant All ITT patients Mutant only1 508 236 65% vs 54% 66% vs 55% 11% 11% 12.3 vs 9.7 12.0 vs 9.5 0.77 p=0.006 0.78 Data from Positive 1st line mCRC Chemo/bev Phase 3 Clinical Trials by RAS-mut Status* * Source: Bevacizumab: USPI from accessdata.fda.gov, Hurwitz H, et al. The Oncologist 2009. FOLFOXIRI: Cremolini C, et al. Lancet Oncol 2015. 1. RAS mutation was evaluated retrospectively and tumor samples for RAS analysis were not available for all patients. mCRC, metastatic colorectal cancer; SoC, standard of care; ORR, objective response rate; ITT, intent-to-treat; Exp, experimental arm; Ctrl, control arm; PFS, progression free survival; WT, wild type; bev, bevacizumab; p, p-value

Trial design of CRDF-004: 1st line RAS-mutated mCRC Phase 2 trial 1st line SoC: �Chemo + bevacizumab 1st line SoC: �Chemo + bevacizumab 28 DAY CYCLE 6 7 8 9 10 11 12 13 14 20 21 22 23 24 25 26 27 28 ONVANSERTIB ONVANSERTIB ENROLLMENT CRITERIA ENDPOINTS* Primary: Secondary: ORR DoR and PFS KRAS+/NRAS+ Unresectable First-line mCRC N=90 R No prior bev Onv 30mg + Onv 20mg + SoC alone 6 RANDOMIZATION ARMS * Assessed by blinded independent central review (BICR) Patient’s tumors are scanned every 8 weeks 1. FOLFIRI/bev 2. FOLFOX/bev 3. FOLFIRI/bev 4. FOLFOX/bev 5. FOLFIRI/bev 6. FOLFOX/bev mCRC, metastatic colorectal cancer; ORR, objective response rate; DoR, duration of response; PFS, progression free survival; SoC, standard of care; onv, onvansertib; bev, bevacizumab

As of July 8, 2025, a majority of CRDF-004 patients remain on treatment Population, n Control (SoC alone) Onv 20mg + SoC Onv 30mg + SoC Total Intent-to-treat (ITT) 37 36 37 110 Safety population (dosed) 34 34 36 104 Patients still on trial 18 19 23 60 Patients with only a 2-month scan and remain on trial 3 2 1 6 Median follow up time for all patients is ~6 months * CRDF-004 population data as of July 8, 2025 from an ongoing trial and unlocked database. SoC, standard of care; onv, onvansertib Study Populations as of July 8, 2025*

Dose-dependent increase in objective response rates observed with onvansertib+SoC Intent-to-treat (ITT) (N=110) Control (SoC alone) (n=37) Onv 20mg + SoC (n=36) Onv 30mg + SoC (n=37) Onv 30mg vs. Control Confirmed ORR1 n, [95% CI] 30% n=11 [16-47] 42% n=15 [26–59] 49% n=18 [32–66] 19% p=0.018 Confirmed ORR at 6 months 22% n=8 33% n=12 46% n=17 * Radiographic response determined per RECIST 1.1 by blinded independent central review as of July 8, 2025 from an ongoing trial and unlocked database. 1. Confirmed ORR includes positively confirmed CRs and PRs per RECIST 1.1. SoC, standard of care; ORR, objective response rate; CI, confidence interval; p, p-value; onv, onvansertib Objective Response Rates per RECIST 1.1*

Dose-dependent increase in objective response rates observed with onvansertib+SoC Intent-to-treat (ITT) (N=110) Control (SoC alone) (n=37) Onv 20mg + SoC (n=36) Onv 30mg + SoC (n=37) Onv 30mg vs. Control Confirmed ORR1 n, [95% CI] 30% n=11 [16-47] 42% n=15 [26–59] 49% n=18 [32–66] 19% p=0.018 Confirmed ORR at 6 months 22% n=8 33% n=12 46% n=17 ORR2 n, [95% CI] 43% n=16 [27–61] 50% n=18 [33–67] 59% n=22 [42–75] Best response on trial Complete Response (CR) 1 (3%) 1 (3%) 2 (5%) Partial Response (PR) 15 (41%) 17 (47%) 20 (54%) Unconfirmed (will not confirm) PR/CR 3 (8%) 3 (8%) 1 (3%) Stable Disease (SD) 9 (24%) 10 (28%) 8 (22%) Progressive Disease (PD) 0 0 1 (3%) Death 1 (3%) 0 1 (3%) Not evaluable 8 (22%) 5 (14%) 4 (11%) * Radiographic response determined per RECIST 1.1 by blinded independent central review as of July 8, 2025 from an ongoing trial and unlocked database. 1. Confirmed ORR includes positively confirmed CRs and PRs per RECIST 1.1. 2. ORR includes positively confirmed CRs and PRs and unconfirmed PRs who were still on treatment and may yet be confirmed. SoC, standard of care; ORR, objective response rate; CI, confidence interval; p, p-value; onv, onvansertib Objective Response Rates per RECIST 1.1*

Deeper tumor regression observed with onvansertib+SoC Best Radiographic Response BY ONVANSERTIB DOSE* Best % Change from Baseline Best Response CR PR PD SD Confirmed CR Confirmed PR Patient number FOLFIRI FOLFOX Unconfirmed PR Intent-to-treat (ITT) Control �(SoC alone) Onv 20mg�+ SoC Onv 30mg�+ SoC Confirmed ORR1 30% 42% 49% ORR2 43% 50% 59% > On treatment Onvansertib 20mg plus SoC Onvansertib 30mg plus SoC SoC Experimental Arms Control Arm * Radiographic response determined per RECIST 1.1 by blinded independent central review as of July 8, 2025 from an ongoing trial and unlocked database. A PR with no circle above is an unconfirmed PR with treatment discontinued (will never confirm) and is not considered a responder for ORR calculation. Patients 1003-065 (unconfirmed PR) and 1011-106 (Non-CR/Non-PD) do not appear on the waterfall plot as they had no target lesions. 1. Confirmed ORR includes positively confirmed CRs and PRs per RECIST 1.1. 2. ORR includes positively confirmed CRs and PRs and unconfirmed PRs who were still on treatment and may yet be confirmed. SoC, standard of care; ORR, objective response rate; onv, onvansertib; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease

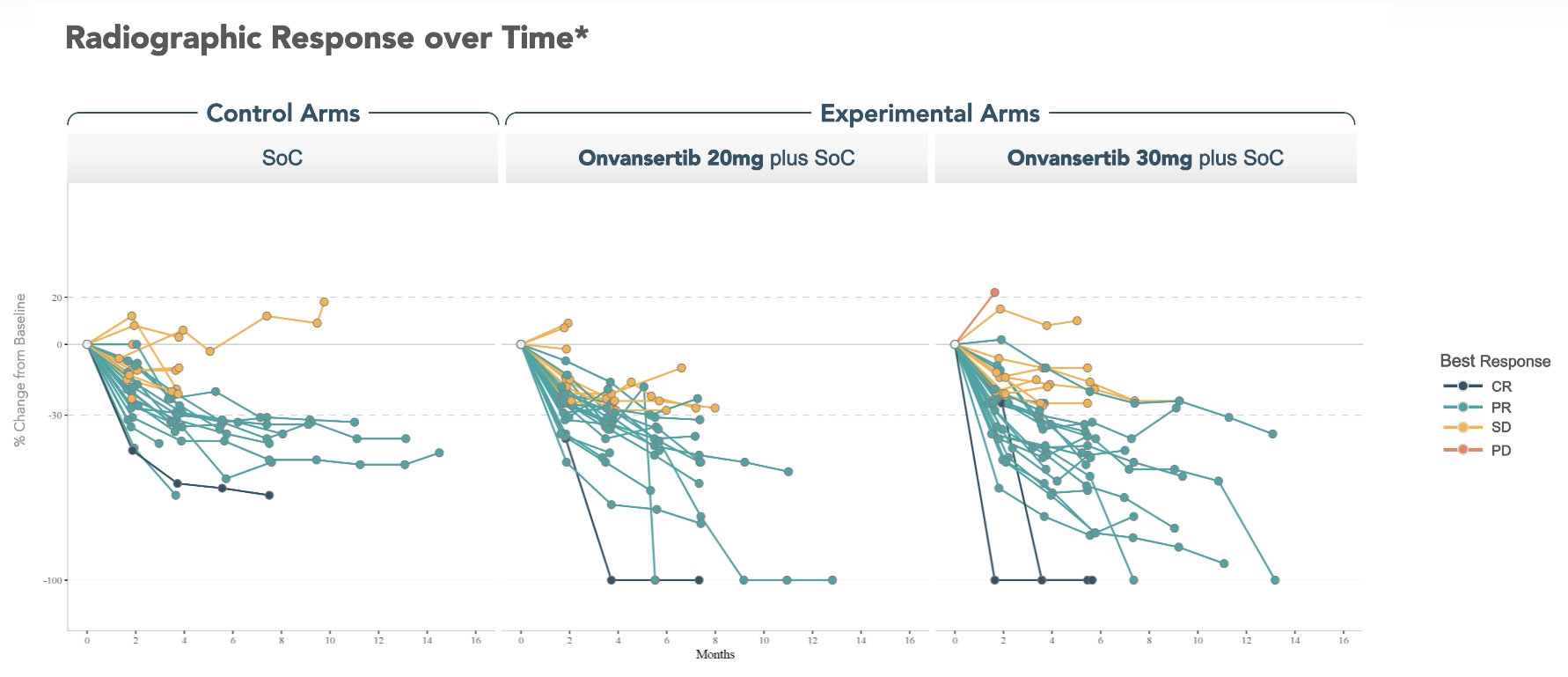
Best Response Progressive Disease Stable Disease Partial Response Complete Response Progressive Disease Stable Disease Partial Response Complete Response Scan Response Onvansertib 20mg plus SoC Onvansertib 30mg plus SoC SoC Experimental Arms Control Arms % Change from Baseline Deeper tumor regression over time observed with onvansertib+SoC Radiographic Response over Time* Best Response CR PR PD SD * Radiographic response determined per RECIST 1.1 by blinded independent central review as of July 8, 2025 from an ongoing trial and unlocked database. SoC, standard of care; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease

Deeper tumor regression observed when adding onvansertib to either chemo backbone vs SoC alone Best Radiographic Response BY CHEMO BACKBONE* Best Response CR PR PD SD Confirmed CR Confirmed PR Patient number Onv 20mg+SoC Onv 30mg+SoC Unconfirmed PR Best % Change from Baseline Intent-to-treat (ITT) Control SoC + Onv Control SoC + Onv Confirmed ORR1 26% 44% 33% 46% ORR2 47% 50% 39% 59% FOLFIRI FOLFOX > On treatment FOLFIRI / bev (Control) FOLFIRI / bev / onvansertib (Experimental) FOLFIRI Arms FOLFOX / bev / onvansertib (Experimental) FOLFOX Arms FOLFOX / bev (Control) * Radiographic response determined per RECIST 1.1 by blinded independent central review as of July 8, 2025 from an ongoing trial and unlocked database. A PR with no circle above is an unconfirmed PR with treatment discontinued (will never confirm) and is not considered a responder for ORR calculation. Patients 1003-065 (unconfirmed PR) and 1011-106 (Non-CR/Non-PD) do not appear on the waterfall plot as they had no target lesions. 1. Confirmed ORR includes positively confirmed CRs and PRs per RECIST 1.1. 2. ORR includes positively confirmed CRs and PRs and unconfirmed PRs who were still on treatment and may yet be confirmed. SoC, standard of care; ORR, objective response rate; onv, onvansertib; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease

Higher number of 30mg onvansertib patients remain on trial vs. control Radiographic Response over Time* Onv 20mg + SoC Control arms Onv 30mg + SoC Time on Trial by Best Response CR/PR PD SD CR PR FOLFOX FOLFIRI First response scan > On treatment Safety Population (Dosed) Control �(SoC alone) Onv 20mg�+ SoC Onv 30mg�+ SoC Patients on treatment 18 (53%) 19 (56%) 23 (64%) Patients discontinued treatment: 16 (47%) 15 (44%) 13 (36%) To pursue surgery 3 3 5 Progressive disease 5 6 3 Adverse events/toxicity1 1 3 2 Median follow up time for all patients is ~6 months Adverse event To pursue surgery Progressive disease Physician decision Patient decision Reason for discontinuation�(per EDC) * Radiographic response determined per RECIST 1.1 by blinded independent central review as of July 8, 2025 from an ongoing trial and unlocked database. 1. One control, one 20mg and two 30mg patients discontinued due to adverse events / toxicity prior to their first post-baseline scan and are not included in the swimmer plot. SoC, standard of care; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; onv, onvansertib; EDC, electronic data capture system On follow up

Several patients in onvansertib arms achieved deep responses, CR, and surgery referrals* 47-year-old female Metastatic disease on enrollment. Right sided colon cancer. Target lesions in peritoneum �(SLD 27mm) with non-target lesions throughout peritoneum. Achieved CR and went to curative surgery after 6 cycles of treatment. 30mg onv + FOLFIRI/bev 69-year-old male Adjuvant FOLFOX for stage 3 colon cancer 1 year prior to study. Right sided colon cancer. Target lesions paracolic gutter and peritoneum (SLD 39 mm) with non-target lesions peritoneal nodules throughout abdomen. Achieved CR of target lesions and confirmed 100% PR. Continues on treatment. 20mg onv + FOLFOX/bev 49-year-old male Neoadjuvant CAPOX for stage 3 colon cancer 1 year prior to study. Bilateral disease (right and left) colon cancer. Target lesions in lung and seminal vesicles (SLD 50 mm) with non-target lesions in retroperitoneum and liver. Achieved CR after 4 cycles of treatment. Continues on treatment. 20mg onv + FOLFOX/bev 62-year-old male Metastatic disease. Right sided colon cancer. Target lesions in liver (SLD 32mm), non-target lesions in liver and adrenal gland. Achieved CR after 6 cycles. Referred for curative surgery. 30mg onv + FOLFIRI/bev * Radiographic response determined per RECIST 1.1 by blinded independent central review as of July 8, 2025 from an ongoing trial and unlocked database. SLD, sum of the longest diameters; onv, onvansertib; bev, bevacizumab; CR, complete response; PR, partial response

CRDF-004 demographics and baseline characteristics* * Demographics and baseline characteristics are as of July 8, 2025 from an ongoing trial and unlocked database. Bev, bevacizumab; onv, onvansertib Safety Population (Dosed) FOLFIRI/bev FOLFIRI/bev/onv 20 FOLFIRI/bev/onv 30 FOLFOX/bev FOLFOX/bev/onv 20 FOLFOX/bev/onv 30 Total (n=17) (n=17) (n=18) (n=17) (n=17) (n=18) (n=104) Age (years) Median 53 (32, 81) 52 (30, 78) 60 (34, 81) 57 (34, 82) 66 (34, 79) 59.5 (39, 86) 57 (30, 86) Gender, n (%) Male 10 (58.8) 10 (58.8) 10 (55.6) 11 (64.7) 7 (41.2) 11 (61.1) 59 (56.7) Female 7 (41.2) 7 (41.2) 8 (44.4) 6 (35.3) 10 (58.8) 7 (38.9) 45 (43.3) Race, n (%) White 13 (76.5) 15 (88.2) 15 (83.3) 12 (70.6) 13 (76.5) 13 (72.2) 81 (77.9) Black or African American 2 (11.8) 0 1 (5.6) 1 (5.9) 0 2 (11.1) 6 (5.8) Asian 1 (5.9) 0 1 (5.6) 1 (5.9) 2 (11.8) 1 (5.6) 6 (5.8) Native Hawaiian or Other Pacific Islander 0 1 (5.9) 0 1 (5.9) 0 0 2 (1.9) Not reported 0 1 (5.9) 0 2 (11.8) 1 (5.9) 1 (5.6) 5 (4.8) Unknown 1 (5.9) 0 1 (5.6) 0 1 (5.9) 1 (5.6) 4 (3.8) ECOG, n (%) 0 6 (35.3) 14 (82.4) 11 (61.1) 7 (41.2) 10 (58.8) 11 (61.1) 59 (56.7) 1 11 (64.7) 3 (17.6) 7 (38.9) 10 (58.8) 7 (41.2) 7 (38.9) 45 (43.3) Stage at Initial Diagnosis, n (%) STAGE I 0 1 (5.9) 0 0 1 (5.9) 1 (5.6) 3 (2.9) STAGE II 3 (17.6) 2 (11.8) 2 (11.1) 2 (11.8) 3 (17.6) 1 (5.6) 13 (12.5) STAGE III 4 (23.5) 4 (23.5) 2 (11.1) 6 (35.3) 2 (11.8) 3 (16.7) 21 (20.2) STAGE IV 9 (52.9) 10 (58.8) 14 (77.8) 9 (52.9) 11 (64.7) 13 (72.2) 66 (63.5) Missing 1 (5.9) 0 0 0 0 0 1 (1.0) Side of Tumor, n (%) Bilateral 6 (35.3) 2 (11.8) 6 (33.3) 4 (23.5) 2 (11.8) 7 (38.9) 27 (26.0) Left 6 (35.3) 7 (41.2) 6 (33.3) 5 (29.4) 8 (47.1) 4 (22.2) 36 (34.6) Right 5 (29.4) 8 (47.1) 6 (33.3) 8 (47.1) 7 (41.2) 7 (38.9) 41 (39.4) Liver metastasis at study entry, n (%) No 7 (41.2) 8 (47.1) 5 (27.8) 9 (52.9) 5 (29.4) 4 (22.2) 38 (36.5) Yes 10 (58.8) 9 (52.9) 13 (72.2) 8 (47.1) 12 (70.6) 14 (77.8) 66 (63.5) Liver only disease, n (%) No 15 (88.2) 15 (88.2) 11 (61.1) 14 (82.4) 16 (94.1) 15 (83.3) 86 (82.7) Yes 2 (11.8) 2 (11.8) 7 (38.9) 3 (17.6) 1 (5.9) 3 (16.7) 18 (17.3) Number of organs involved at baseline, n (%) <3 organs 13 (76.5) 9 (52.9) 10 (55.6) 12 (70.6) 11 (64.7) 8 (44.4) 63 (60.6) >=3 organs 4 (23.5) 7 (41.2) 8 (44.4) 5 (29.4) 6 (35.3) 10 (55.6) 40 (38.5) Missing 0 1 (5.9) 0 0 0 0 1 (1.0) Prior adjuvant or neo-adjuvant chemotherapy, n (%) No 13 (76.5) 12 (70.6) 14 (77.8) 12 (70.6) 12 (70.6) 16 (88.9) 79 (76.0) Yes 4 (23.5) 5 (29.4) 4 (22.2) 5 (29.4) 5 (29.4) 2 (11.1) 25 (24.0)

Safety Population (Dosed) All Control Arms�(N=34) Onv 20mg + SoC (N=34) Onv 30mg + SoC�(N=36) N (% of total) All Grades Gr >=3 All Grades Gr >=3 All Grades Gr >=3 Any Adverse Events 33 ( 97.1) 21 ( 61.8) 34 (100.0) 24 ( 70.6) 36 (100.0) 28 ( 77.8) Fatigue 16 ( 47.1) 2 ( 5.9) 24 ( 70.6) 1 ( 2.9) 21 ( 58.3) 0 Nausea 17 ( 50.0) 1 ( 2.9) 25 ( 73.5) 0 17 ( 47.2) 0 Diarrhoea 17 ( 50.0) 1 ( 2.9) 19 ( 55.9) 2 ( 5.9) 16 ( 44.4) 0 Neutrophil count decreased 18 ( 52.9) 11 ( 32.4) 13 ( 38.2) 6 ( 17.6) 17 ( 47.2) 11 ( 30.6) Hypertension 7 ( 20.6) 1 ( 2.9) 12 ( 35.3) 4 ( 11.8) 12 ( 33.3) 3 ( 8.3) Vomiting 8 ( 23.5) 1 ( 2.9) 13 ( 38.2) 0 8 ( 22.2) 0 Constipation 5 ( 14.7) 1 ( 2.9) 13 ( 38.2) 0 10 ( 27.8) 0 Epistaxis 7 ( 20.6) 0 11 ( 32.4) 0 9 ( 25.0) 0 Peripheral sensory neuropathy 8 ( 23.5) 0 10 ( 29.4) 2 ( 5.9) 9 ( 25.0) 1 ( 2.8) Abdominal pain 5 ( 14.7) 2 ( 5.9) 10 ( 29.4) 1 ( 2.9) 11 ( 30.6) 1 ( 2.8) Anaemia 7 ( 20.6) 1 ( 2.9) 8 ( 23.5) 0 11 ( 30.6) 4 ( 11.1) Decreased appetite 9 ( 26.5) 0 11 ( 32.4) 0 6 ( 16.7) 0 Platelet count decreased 9 ( 26.5) 2 ( 5.9) 8 ( 23.5) 0 9 ( 25.0) 1 ( 2.8) Alopecia 7 ( 20.6) 0 8 ( 23.5) 0 8 ( 22.2) 0 Headache 8 ( 23.5) 0 10 ( 29.4) 0 3 ( 8.3) 0 White blood cell count decreased 10 ( 29.4) 0 4 ( 11.8) 0 7 ( 19.4) 1 ( 2.8) Dizziness 6 ( 17.6) 0 7 ( 20.6) 0 7 ( 19.4) 0 Dysgeusia 6 ( 17.6) 0 6 ( 17.6) 0 8 ( 22.2) 0 Weight decreased 8 ( 23.5) 1 ( 2.9) 4 ( 11.8) 0 8 ( 22.2) 0 Hypokalaemia 5 ( 14.7) 1 ( 2.9) 6 ( 17.6) 2 ( 5.9) 8 ( 22.2) 3 ( 8.3) Stomatitis 8 ( 23.5) 0 8 ( 23.5) 0 2 ( 5.6) 0 Insomnia 1 ( 2.9) 0 9 ( 26.5) 0 7 ( 19.4) 0 Paraesthesia 3 ( 8.8) 0 7 ( 20.6) 0 6 ( 16.7) 0 Lymphocyte count decreased 5 ( 14.7) 0 3 ( 8.8) 0 7 ( 19.4) 2 ( 5.6) Cough 5 ( 14.7) 0 4 ( 11.8) 0 5 ( 13.9) 0 Pyrexia 4 ( 11.8) 0 6 ( 17.6) 1 ( 2.9) 4 ( 11.1) 1 ( 2.8) Blood alkaline phosphatase increased 7 ( 20.6) 0 1 ( 2.9) 0 4 ( 11.1) 0 Dyspepsia 2 ( 5.9) 0 5 ( 14.7) 0 5 ( 13.9) 0 Proteinuria 2 ( 5.9) 0 6 ( 17.6) 0 4 ( 11.1) 0 * Data consists of all adverse events entered into the electronic data capture (EDC) system as of July 8, 2025, from an ongoing trial and unlocked EDC database. N: number of patients; events shown occurred in ≥10% of total patients; numbers indicate number of patients experiencing the event, (regardless of causality); each patient is only counted once and only for the highest grade of a given event. Columns show the absolute # of patients and (%) of the population. Onv, onvansertib; SoC, standard of care CRDF-004 treatment emergent adverse events (TEAE) data*

Dose intensity is similar and high across all trial arms Safety Population (Dosed) FOLFIRI/bev�(n=17) FOLFIRI/bev/onv 20�(n=17) FOLFIRI/bev/onv 30�(n=18) FOLFOX/bev�(n=17) FOLFOX/bev/onv 20�(n=17) FOLFOX/bev/onv 30�(n=18) Relative dose intensity (%) Mean (Std) 91.84 (12.8) 90.37 (12.6) 91.39 (9.8) 91.34 (11.0) 93.34 (9.1) 86.89 (15.1) Median 96.93 96.32 93.24 93.24 96.5 91.22 * Data as of July 8, 2025 from an ongoing trial and unlocked database. Bev, bevacizumab; onv, onvansertib; Std, standard deviation Relative Dose Intensity: actual amount of study drug a patient receives over time compared to the planned dose and schedule*

AGENDA 1st line RAS-mut mCRC program update ORR efficacy and safety PFS analyses Registrational program path forward mCRC, metastatic colorectal cancer; mut, mutant; ORR, objective response rate; PFS, progression free survival

PFS as of July 8, 2025 data cutoff shows initial separation between 30mg onv and control arms * Progression determined per electronic data capture system as of July 8, 2025 from an ongoing trial and unlocked database. SoC, standard of care; PFS, progression free survival; HR, hazard ratio; CI, confidence interval; onv, onvansertib Progression Free Survival – Median PFS Not Reached* Onv 30mg + SoC Strata Control arm Onv 20mg + SoC PFS Probability Number at risk Onv 30mg + SoC Control arm Onv 20mg + SoC Hazard Ratio (HR) HR 95% CI Control vs. all onv arms 0.69 0.25, 1.90 Control vs. onv 20mg + SoC Control vs. onv 30mg + SoC 0.89 0.52 0.28, 2.77 0.15,1.83 Median follow up is ~6 months Censored patients: Control (23/29); 20mg onv+SoC (25/31); 30mg onv+SoC (29/33)

In 1st line mCRC, two response metrics predict PFS and OS Early Depth Tumor Shrinkage (ETS) of Response (DpR) ≥20% reduction in tumor size at 2-month scan Deepest reduction in tumor size while on therapy on trial Proof-of-Principle Meta Analysis Validation Oct, 2013 Feb, 2015 Use of Early Tumor Shrinkage to Predict Long-Term Outcome in mCRC Treated With Cetuximab Piessevaux, et. al. Early Tumor Shrinkage and Depth of Response Predict Long-term Outcome in mCRC Patients Treated with 1st-line Chemo+bev Cremolini, et. al. Apr, 2025 Bando, et. al. Associations Between Early Tumor Shrinkage/Depth of Response and Survival from the ARCAD Database TRIBE FOLFOXIRI+bev vs. FOLFIRI+bev CRYSTAL�FOLFIRI+cetux.�vs FOLFIRI OPUS FOLFOX-4+cetux. vs. FOLFOX-4 8 randomized trials Ph3 TRIAL DATA* * First-line mCRC trials in which ETS and/or DpR were evaluated as predictors of PFS and OS comparing a control arm of chemo alone vs. an experimental arm of chemo + an active agent including bevacizumab (TRIBE) and cetuximab (CRYSTAL and OPUS). mCRC, metastatic colorectal cancer; PFS, progression free survival; OS, overall survival; bev, bevacizumab; cetux, cetuximab.

Greater number of onvansertib 30mg dose patients achieved Early Tumor Shrinkage 1. First-line mCRC trials in which ETS and/or DpR were evaluated as predictors of PFS and OS comparing a control arm of chemo alone vs. an experimental arm of chemo + an active agent including bevacizumab (TRIBE) and cetuximab (CRYSTAL and OPUS). Piessevaux, et al, J Clin Oncol 2013; Cremolini, et al, Ann Oncol 2015; Van Cutsem, et. al, N Engl J Med 2009 (HR for CRYSTAL); Bokemeyer et al, Ann Oncol 2011 (HR for OPUS). ETS, early tumor shrinkage; mCRC, metastatic colorectal cancer; WT, wild type; mut., mutated; PFS, progression free survival; bev, bevacizumab; onv, onvansertib. Control Arm Early Tumor Shrinkage (ETS) ≥20% reduction in tumor size at 2-month scan. Final data: All patients on trial have had a 2-month scan. ETS Delta p-value % of patients with ETS TRIBE CRYSTAL OPUS 63% 62% 69% 13% 23% 11% Hazard Ratio 0.79 0.68 0.57 Improvement in PFS 2.0 mo 4.4 mo 3.7 mo 0.025 0.02 0.006 Experimental Arm 63% 69% 52% 49% 46% 41% 22% 28% 0.114 0.038 (19/30) (22/32) (11/27) Onv 20mg Onv 30mg CRDF-004 Previous Ph3 �1st Line mCRC Trials1 RAS WT/mut. RAS WT RAS WT RAS mut.

Best Response Progressive Disease Stable Disease Partial Response Complete Response Progressive Disease Stable Disease Partial Response Complete Response Scan Response Tumor regression vs. baseline is deeper over time with onv 30mg dose Control Onv�20mg Onv�30mg Radiographic Response over Time* Onvansertib 20mg plus SoC Onvansertib 30mg plus SoC SoC Experimental Arms Control Arms Best % Change from Baseline Best Response CR PR PD SD % Change from Baseline * Radiographic response determined per RECIST 1.1 by blinded independent central review as of July 8, 2025 from an ongoing trial and unlocked database. SoC, standard of care; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; onv, onvansertib; p, p-value

Depth of Response is deeper for the onv 30mg dose arm Depth of �Response (DpR) Maximum tumor shrinkage at nadir on trial Interim data: Patients on trial may achieve deeper tumor regression Control Arm DpR Delta p-value % Tumor Shrinkage 43% 51% 58% 18% 27% 5% Hazard Ratio 0.79 0.68 0.57 Improvement in PFS 2.0 mo 4.4 mo 3.7 mo Experimental Arm 41% 48% 38% 33% 31% 32% 9% 16% 0.066 0.011 Onv 20mg Onv 30mg TRIBE CRYSTAL OPUS CRDF-004 Previous Ph3 �1st Line mCRC Trials1 RAS WT/mut. RAS WT RAS WT RAS mut. 1. First-line mCRC trials in which ETS and/or DpR were evaluated as predictors of PFS and OS comparing a control arm of chemo alone vs. an experimental arm of chemo + an active agent including bevacizumab (TRIBE) and cetuximab (CRYSTAL and OPUS). 1. Cremolini, et al, Ann Oncol 2015; Piessevaux, et al, J Clin Oncol 2013; Mansmann, et al, Ann Oncol 2013 ; Van Cutsem, et. al, N Engl J Med 2009 (HR for CRYSTAL); Bokemeyer et al, Ann Oncol 2011 (HR for OPUS). DpR, depth of response; mCRC, metastatic colorectal cancer; WT, wild type; mut., mutated; PFS, progression free survival; onv, onvansertib.

AGENDA 1st line RAS-mut mCRC program update ORR efficacy and safety PFS analyses Registrational program path forward mCRC, metastatic colorectal cancer; Mut, mutant; ORR, objective response rate; PFS, progression free survival

Current CRDF-004 trial data are supportive of a 30mg dose 2024 2025 INTENT 1. Select a Ph3 dose – per FDA’s Project Optimus 2. Assess efficacy signal 3. Characterize safety profile in first-line setting 4. Basis for meeting with FDA to agree Ph3 trial 2026 Progress to date Data supports focus on onvansertib 30mg dose CRDF-004 Ph2 trial 1st line RAS-mut mCRC mCRC, metastatic colorectal cancer; mut., mutated

Dose response observed across ORR, ETS and DpR efficacy signals and may predict longer PFS 2024 2025 INTENT 1. Select a Ph3 dose – per FDA’s Project Optimus 2. Assess efficacy signal 3. Characterize safety profile in first-line setting 4. Basis for meeting with FDA to agree Ph3 trial 2026 Progress to date ORR: meaningful deltas in context of 1st line mCRC PFS: early PFS separation and correlative response signals Dose-dependent response CRDF-004 Ph2 trial 1st line RAS-mut mCRC mCRC, metastatic colorectal cancer; mut., mutated; ORR, objective response rate; PFS, progression free survival

Onvansertib in combination with SoC is generally well-tolerated 2024 2025 INTENT 1. Select a Ph3 dose – per FDA’s Project Optimus 2. Assess efficacy signal 3. Characterize safety profile in first-line setting 4. Basis for meeting with FDA to agree Ph3 trial 2026 Progress to date Onvansertib is generally well-tolerated in combination with both chemo backbones and bev CRDF-004 Ph2 trial 1st line RAS-mut mCRC SoC, standard of care; mCRC, metastatic colorectal cancer; mut., mutated; bev, bevacizumab

We intend to discuss our registrational trial protocol with FDA 2024 2025 INTENT 1. Select a Ph3 dose – per FDA’s Project Optimus 2. Assess efficacy signal 3. Characterize safety profile in first-line setting 4. Basis for meeting with FDA to agree Ph3 trial 2026 Seek FDA Agreement for Ph3 CRDF-005�registrational protocol 4 Progress to date Totality of data supports moving forward with FDA interactions on the registrational program CRDF-004 Ph2 trial 1st line RAS-mut mCRC mCRC, metastatic colorectal cancer; mut., mutated

We believe CRDF-004 data positions onvansertib for registrational trial PHASE 2 DOSE-CONFIRMATION TRIAL PHASE 3 REGISTRATIONAL TRIAL 1st line RAS-mutated mCRC clinical development program Agreed with FDA June 2023 Type C meeting Designed for accelerated and full-approval Endpoint for accelerated approval:�- ORR with DoR Endpoint for full approval:�- PFS / lack of detriment on OS mCRC, metastatic colorectal cancer; ORR, objective response rate; DoR, duration of response; PFS, progression free survival; OS, overall survival

APPENDIX

Dec 2024: Initial data showed deeper tumor shrinkage with onvansertib that appeared dose-dependent Radiographic Response over Time* – as of November 26, 2024 Onvansertib 20mg plus SoC Onvansertib 30mg plus SoC SoC Experimental Arms Control Arms Initial 30 patients data disclosed�Dec 10, 2024 * Radiographic response determined per RECIST 1.1 by blinded independent central review as of November 26, 2024 from an ongoing trial and unlocked database. Response data for one control arm patient changed from the November 26, 2024 data cut as a result of the radiologist at the blinded independent central review modifying the target lesions. SoC, standard of care; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease % Change from Baseline Best Response CR PR PD SD

July 2025: Data for same 30 patients continued to show deeper dose-dependent responses in onvansertib arms Radiographic Response over Time* – as of July 8, 2025 Initial 30 patients data disclosed�July 29, 2025 Onvansertib 20mg plus SoC Onvansertib 30mg plus SoC SoC Experimental Arms Control Arms % Change from Baseline * Radiographic response determined per RECIST 1.1 by blinded independent central review as of July 8, 2025 from an ongoing trial and unlocked database. SoC, standard of care; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease Best Response CR PR PD SD

Swimmer Plot for Stable Disease patients still on trial Radiographic Response over Time* Onv 20mg + SoC Control arms Onv 30mg + SoC Best Response # Stable Disease # indicates % change from baseline > On Treatment Chemotherapy Backbone FOLFIRI FOLFOX * Radiographic response determined per RECIST 1.1 by blinded independent central review as of July 8, 2025 from an ongoing trial and unlocked database. Patient 1011-106 in the onvansertib 20mg arm has only non-target lesions. SoC, standard of care; onv, onvansertib

No baseline characteristic has a significant impact on ORR * Radiographic response determined per RECIST 1.1 by blinded independent central review as of July 8, 2025 from an ongoing trial and unlocked database. SoC, standard of care; ECOG, Eastern Cooperative Oncology Group Forest Plot of the Treatment Effect on ORR by Baseline Characteristic*

Baseline measures of tumor burden (by sum of longest diameters) * Radiographic response determined per RECIST 1.1 by blinded independent central review as of July 8, 2025 from an ongoing trial and unlocked database. 1. Kruskal-Wallis rank sum test; Pearson's Chi-squared test; Fisher's exact test. SLD, sum of longest diameters; SoC, standard of care Safety population - Baseline Sum of Longest Dimensions* (SLD) Characteristic Control Arm (SoC) �N = 34 SoC + onvansertib 20 mg �N = 34 SoC + onvansertib 30 mg �N = 36 p-value1 Baseline sum of longest dimensions: Mean (Min, Max) Median (Q1,Q3) 91 (15, 281) 75 (39,121) 90 (10, 298) 67 (28,134) 83 (16, 270) 74 (43,114) 0.921 Unknown 6 4 3 The mean and median sum of the longest diameters was similar (not significantly different) for control, onvansertib 20mg and onvansertib 30mg arms

CRDF-004 treatment emergent adverse events (TEAE) data* * Data consists of all adverse events entered into the electronic data capture (EDC) system as of July 8, 2025, from an ongoing trial and unlocked EDC database. N: number of patients; events shown occurred in ≥10% of total patients; numbers indicate number of patients experiencing the event, (regardless of causality); each patient is only counted once and only for the highest grade of a given event. Columns show the absolute # of patients and (%) of the population. Bev, bevacizumab; onv, onvansertib Safety Population (Dosed) N (% of total) FOLFIRI/bev �(n=17) FOLFIRI/bev/onv 20mg �(n=17) FOLFIRI/bev/onv 30mg �(n=18) FOLFOX/bev �(n=17) FOLFOX/bev/onv 20mg �(n=17) FOLFOX/bev/onv 30mg �(n=18) All Control Arms�(n=34) All Experimental Arms�(n=70) All Grades Gr >=3 All Grades Gr >=3 All Grades Gr >=3 All Grades Gr >=3 All Grades Gr >=3 All Grades Gr >=3 All Grades Gr >=3 All Grades Gr >=3 Any Adverse Events 17 (100.0) 12 ( 70.6) 17 (100.0) 14 ( 82.4) 18 (100.0) 15 ( 83.3) 16 ( 94.1) 9 ( 52.9) 17 (100.0) 10 ( 58.8) 18 (100.0) 13 ( 72.2) 33 ( 97.1) 21 ( 61.8) 70 (100.0) 52 ( 74.3) Fatigue 7 ( 41.2) 0 12 ( 70.6) 0 11 ( 61.1) 0 9 ( 52.9) 2 ( 11.8) 12 ( 70.6) 1 ( 5.9) 10 ( 55.6) 0 16 ( 47.1) 2 ( 5.9) 45 ( 64.3) 1 ( 1.4) Nausea 6 ( 35.3) 1 ( 5.9) 13 ( 76.5) 0 9 ( 50.0) 0 11 ( 64.7) 0 12 ( 70.6) 0 8 ( 44.4) 0 17 ( 50.0) 1 ( 2.9) 42 ( 60.0) 0 Diarrhea 10 ( 58.8) 1 ( 5.9) 12 ( 70.6) 1 ( 5.9) 9 ( 50.0) 0 7 ( 41.2) 0 7 ( 41.2) 1 ( 5.9) 7 ( 38.9) 0 17 ( 50.0) 1 ( 2.9) 35 ( 50.0) 2 ( 2.9) Neutrophil count decreased 8 ( 47.1) 4 ( 23.5) 4 ( 23.5) 1 ( 5.9) 6 ( 33.3) 3 ( 16.7) 5 ( 29.4) 5 ( 29.4) 6 ( 35.3) 3 ( 17.6) 7 ( 38.9) 4 ( 22.2) 13 ( 38.2) 9 ( 26.5) 23 ( 32.9) 11 ( 15.7) Neutropenia 2 ( 11.8) 1 ( 5.9) 1 ( 5.9) 0 4 ( 22.2) 4 ( 22.2) 3 ( 17.6) 1 ( 5.9) 2 ( 11.8) 2 ( 11.8) 0 0 5 ( 14.7) 2 ( 5.9) 7 ( 10.0) 6 ( 8.6) Hypertension 4 ( 23.5) 1 ( 5.9) 8 ( 47.1) 3 ( 17.6) 6 ( 33.3) 1 ( 5.6) 3 ( 17.6) 0 4 ( 23.5) 1 ( 5.9) 6 ( 33.3) 2 ( 11.1) 7 ( 20.6) 1 ( 2.9) 24 ( 34.3) 7 ( 10.0) Vomiting 5 ( 29.4) 1 ( 5.9) 7 ( 41.2) 0 6 ( 33.3) 0 3 ( 17.6) 0 6 ( 35.3) 0 2 ( 11.1) 0 8 ( 23.5) 1 ( 2.9) 21 ( 30.0) 0 Constipation 3 ( 17.6) 1 ( 5.9) 5 ( 29.4) 0 5 ( 27.8) 0 2 ( 11.8) 0 8 ( 47.1) 0 5 ( 27.8) 0 5 ( 14.7) 1 ( 2.9) 23 ( 32.9) 0 Epistaxis 4 ( 23.5) 0 8 ( 47.1) 0 6 ( 33.3) 0 3 ( 17.6) 0 3 ( 17.6) 0 3 ( 16.7) 0 7 ( 20.6) 0 20 ( 28.6) 0 Peripheral sensory neuropathy 4 ( 23.5) 0 2 ( 11.8) 0 1 ( 5.6) 0 4 ( 23.5) 0 8 ( 47.1) 2 ( 11.8) 8 ( 44.4) 1 ( 5.6) 8 ( 23.5) 0 19 ( 27.1) 3 ( 4.3) Abdominal pain 3 ( 17.6) 2 ( 11.8) 4 ( 23.5) 1 ( 5.9) 6 ( 33.3) 1 ( 5.6) 2 ( 11.8) 0 6 ( 35.3) 0 5 ( 27.8) 0 5 ( 14.7) 2 ( 5.9) 21 ( 30.0) 2 ( 2.9) Anaemia 4 ( 23.5) 1 ( 5.9) 6 ( 35.3) 0 4 ( 22.2) 1 ( 5.6) 3 ( 17.6) 0 2 ( 11.8) 0 7 ( 38.9) 3 ( 16.7) 7 ( 20.6) 1 ( 2.9) 19 ( 27.1) 4 ( 5.7) Decreased appetite 6 ( 35.3) 0 5 ( 29.4) 0 4 ( 22.2) 0 3 ( 17.6) 0 6 ( 35.3) 0 2 ( 11.1) 0 9 ( 26.5) 0 17 ( 24.3) 0 Platelet count decreased 2 ( 11.8) 1 ( 5.9) 1 ( 5.9) 0 2 ( 11.1) 0 7 ( 41.2) 1 ( 5.9) 7 ( 41.2) 0 7 ( 38.9) 1 ( 5.6) 9 ( 26.5) 2 ( 5.9) 17 ( 24.3) 1 ( 1.4) Alopecia 5 ( 29.4) 0 4 ( 23.5) 0 6 ( 33.3) 0 2 ( 11.8) 0 4 ( 23.5) 0 2 ( 11.1) 0 7 ( 20.6) 0 16 ( 22.9) 0 Headache 4 ( 23.5) 0 6 ( 35.3) 0 2 ( 11.1) 0 4 ( 23.5) 0 4 ( 23.5) 0 1 ( 5.6) 0 8 ( 23.5) 0 13 ( 18.6) 0 White blood cell count decreased 4 ( 23.5) 0 4 ( 23.5) 0 5 ( 27.8) 0 6 ( 35.3) 0 0 0 2 ( 11.1) 1 ( 5.6) 10 ( 29.4) 0 11 ( 15.7) 1 ( 1.4) Dizziness 3 ( 17.6) 0 3 ( 17.6) 0 2 ( 11.1) 0 3 ( 17.6) 0 4 ( 23.5) 0 5 ( 27.8) 0 6 ( 17.6) 0 14 ( 20.0) 0 Dysgeusia 2 ( 11.8) 0 1 ( 5.9) 0 3 ( 16.7) 0 4 ( 23.5) 0 5 ( 29.4) 0 5 ( 27.8) 0 6 ( 17.6) 0 14 ( 20.0) 0 Weight decreased 6 ( 35.3) 1 ( 5.9) 2 ( 11.8) 0 5 ( 27.8) 0 2 ( 11.8) 0 2 ( 11.8) 0 3 ( 16.7) 0 8 ( 23.5) 1 ( 2.9) 12 ( 17.1) 0 Hypokalaemia 3 ( 17.6) 0 3 ( 17.6) 2 ( 11.8) 4 ( 22.2) 2 ( 11.1) 2 ( 11.8) 1 ( 5.9) 3 ( 17.6) 0 4 ( 22.2) 1 ( 5.6) 5 ( 14.7) 1 ( 2.9) 14 ( 20.0) 5 ( 7.1) Stomatitis 3 ( 17.6) 0 6 ( 35.3) 0 1 ( 5.6) 0 5 ( 29.4) 0 2 ( 11.8) 0 1 ( 5.6) 0 8 ( 23.5) 0 10 ( 14.3) 0 Insomnia 0 ( 0.0) 0 4 ( 23.5) 0 3 ( 16.7) 0 1 ( 5.9) 0 5 ( 29.4) 0 4 ( 22.2) 0 1 ( 2.9) 0 16 ( 22.9) 0 Paraesthesia 1 ( 5.9) 0 2 ( 11.8) 0 0 0 2 ( 11.8) 0 5 ( 29.4) 0 6 ( 33.3) 0 3 ( 8.8) 0 13 ( 18.6) 0 Lymphocyte count decreased 3 ( 17.6) 0 2 ( 11.8) 0 4 ( 22.2) 0 2 ( 11.8) 0 1 ( 5.9) 0 3 ( 16.7) 2 ( 11.1) 5 ( 14.7) 0 10 ( 14.3) 2 ( 2.9) Cough 4 ( 23.5) 0 4 ( 23.5) 0 2 ( 11.1) 0 1 ( 5.9) 0 0 0 3 ( 16.7) 0 5 ( 14.7) 0 9 ( 12.9) 0 Pyrexia 2 ( 11.8) 0 3 ( 17.6) 1 ( 5.9) 3 ( 16.7) 1 ( 5.6) 2 ( 11.8) 0 3 ( 17.6) 0 1 ( 5.6) 0 4 ( 11.8) 0 10 ( 14.3) 2 ( 2.9) Blood alkaline phosphatase increased 3 ( 17.6) 0 1 ( 5.9) 0 1 ( 5.6) 0 4 ( 23.5) 0 0 0 3 ( 16.7) 0 7 ( 20.6) 0 5 ( 7.1) 0 Dyspepsia 1 ( 5.9) 0 4 ( 23.5) 0 2 ( 11.1) 0 1 ( 5.9) 0 1 ( 5.9) 0 3 ( 16.7) 0 2 ( 5.9) 0 10 ( 14.3) 0 Proteinuria 2 ( 11.8) 0 3 ( 17.6) 0 2 ( 11.1) 0 0 0 3 ( 17.6) 0 2 ( 11.1) 0 2 ( 5.9) 0 10 ( 14.3) 0