Exhibit 99.1

Dyne Therapeutics Announces Positive Topline Results from Phase 1/2 DELIVER Trial of Z-Rostudirsen in Duchenne Muscular Dystrophy (DMD)
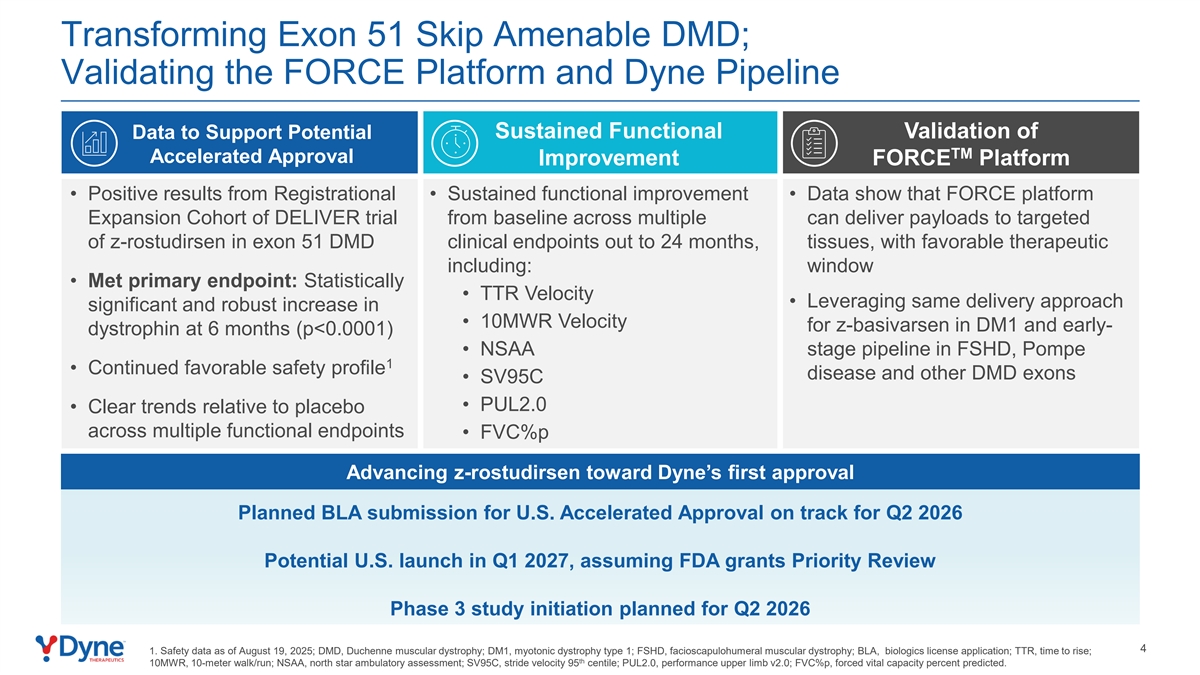
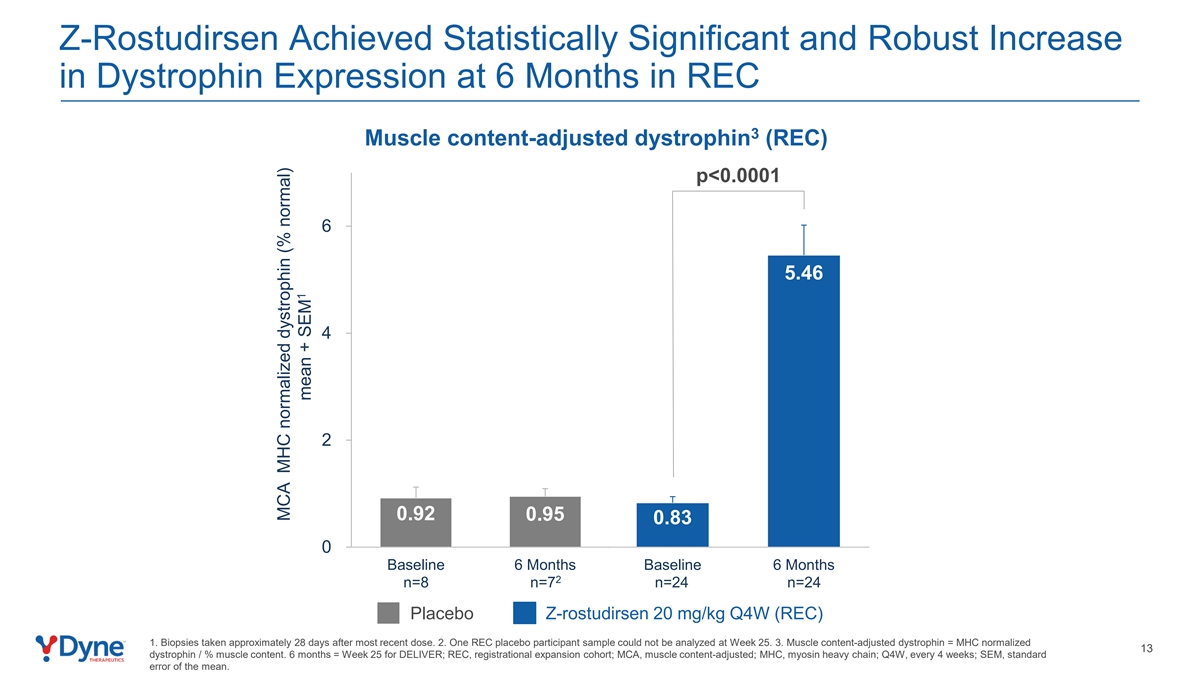
- Registrational Expansion Cohort (REC) met primary endpoint, demonstrating statistically significant increase in dystrophin to 5.46% at 6 months (muscle content-adjusted; p<0.0001), replicating the same 7-fold change from baseline previously observed at the registrational dose -
- Functional improvement was observed across multiple clinical endpoints at 6 months in REC; lung function was preserved at 6 months -
- New positive long-term results from DELIVER trial showed sustained functional improvement across all assessed endpoints through 24 months -
- Continued favorable safety and tolerability profile -
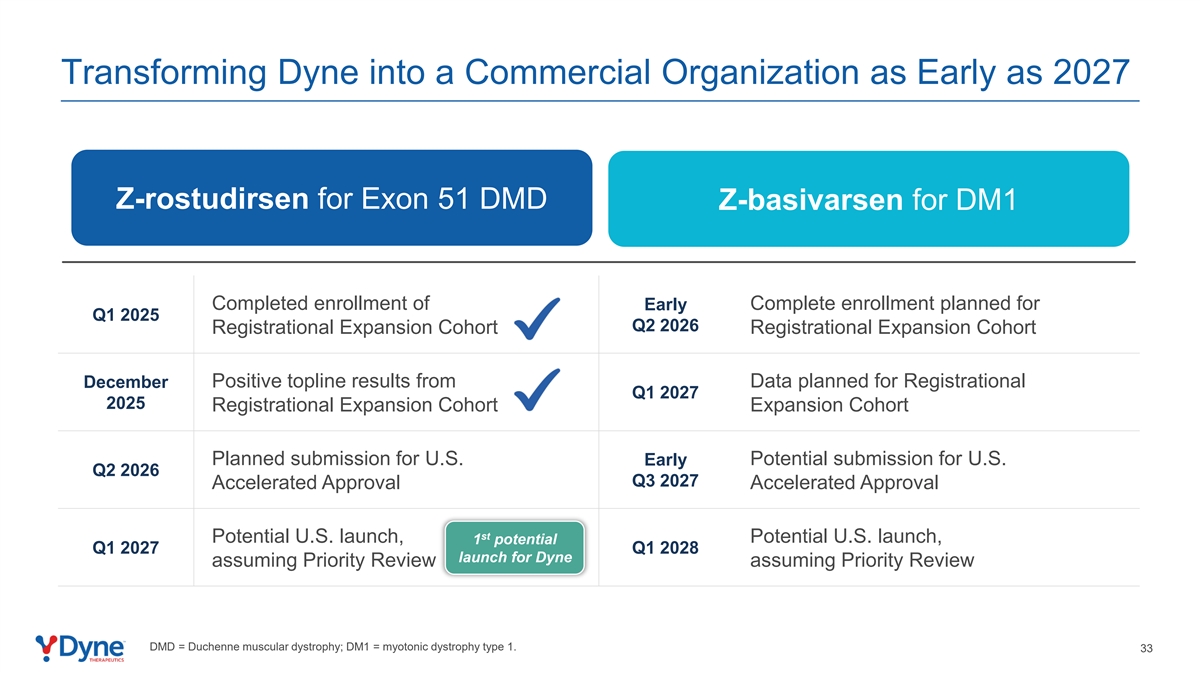
- Submission for U.S. Accelerated Approval on track for Q2 2026 -
- Investor event today, December 8th at 8:00 a.m. ET -
WALTHAM, Mass., December 8, 2025 – Dyne Therapeutics, Inc. (Nasdaq: DYN), a clinical-stage company focused on delivering functional improvement for people living with genetically driven neuromuscular diseases, today announced positive topline results from the Registrational Expansion Cohort (REC) of its Phase 1/2 DELIVER trial evaluating zeleciment rostudirsen (z-rostudirsen, also known as DYNE-251) in individuals with Duchenne muscular dystrophy (DMD) amenable to exon 51 skipping. Additionally, Dyne announced new positive long-term clinical data from the ongoing open-label extension (OLE) and long-term extension (LTE) portions of DELIVER.
The REC met its primary endpoint, demonstrating a statistically significant increase in muscle content-adjusted dystrophin expression to 5.46% of normal relative to baseline at six months (p<0.0001).
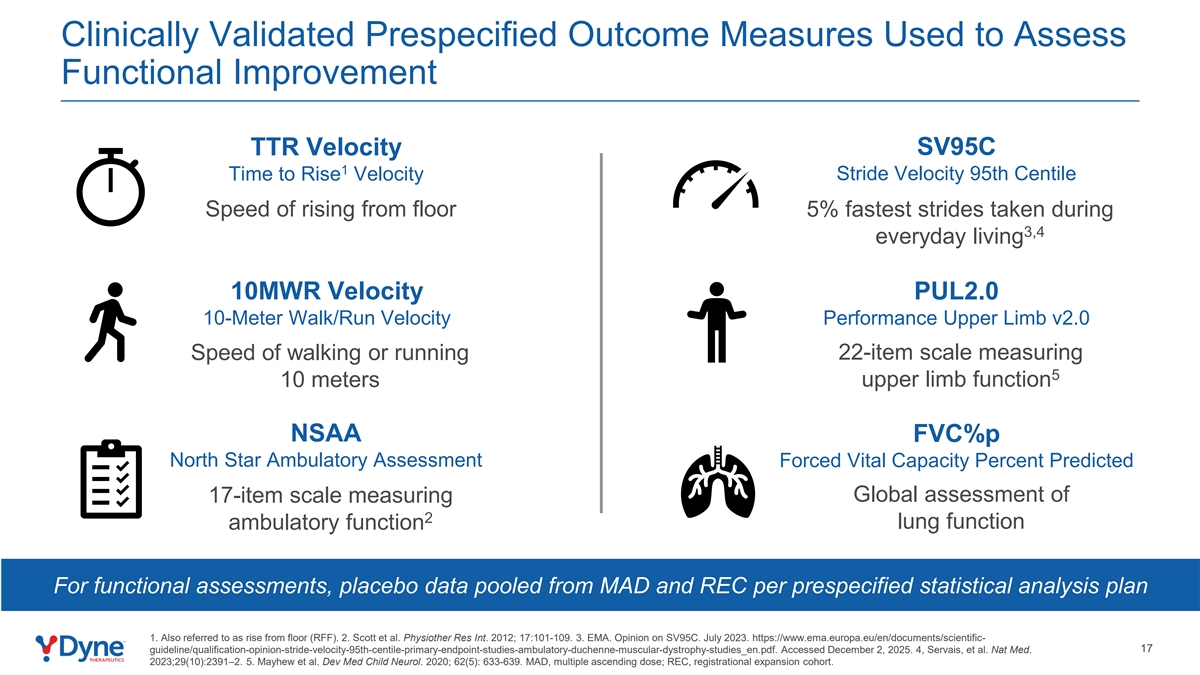
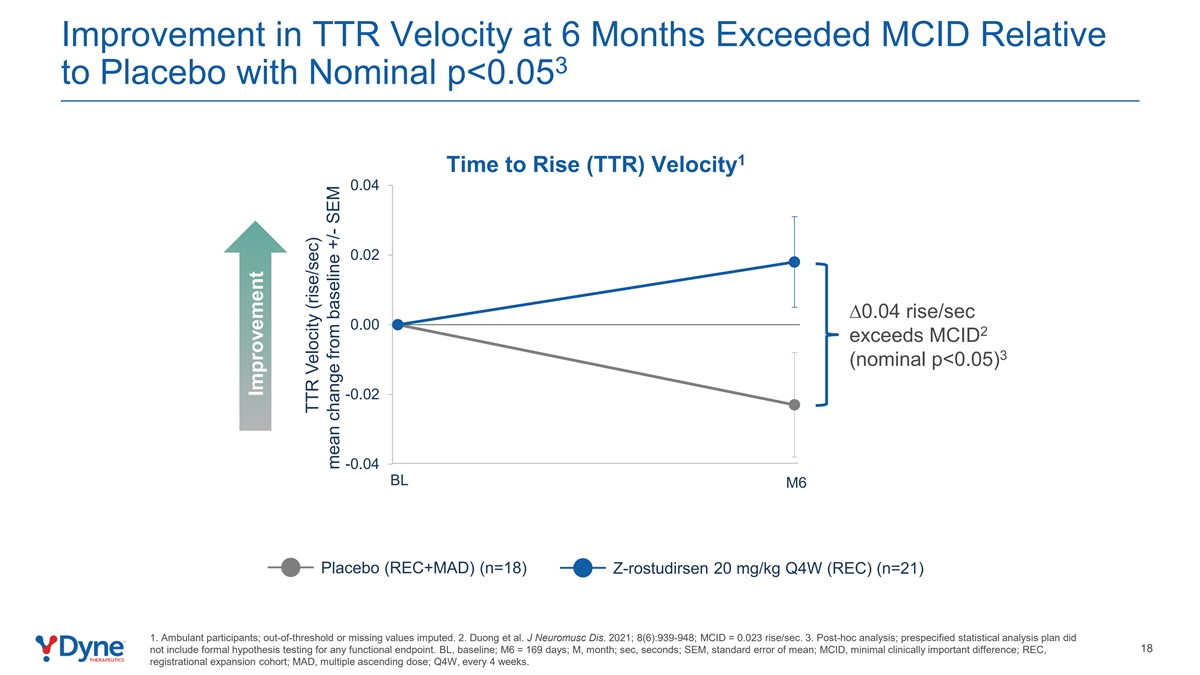
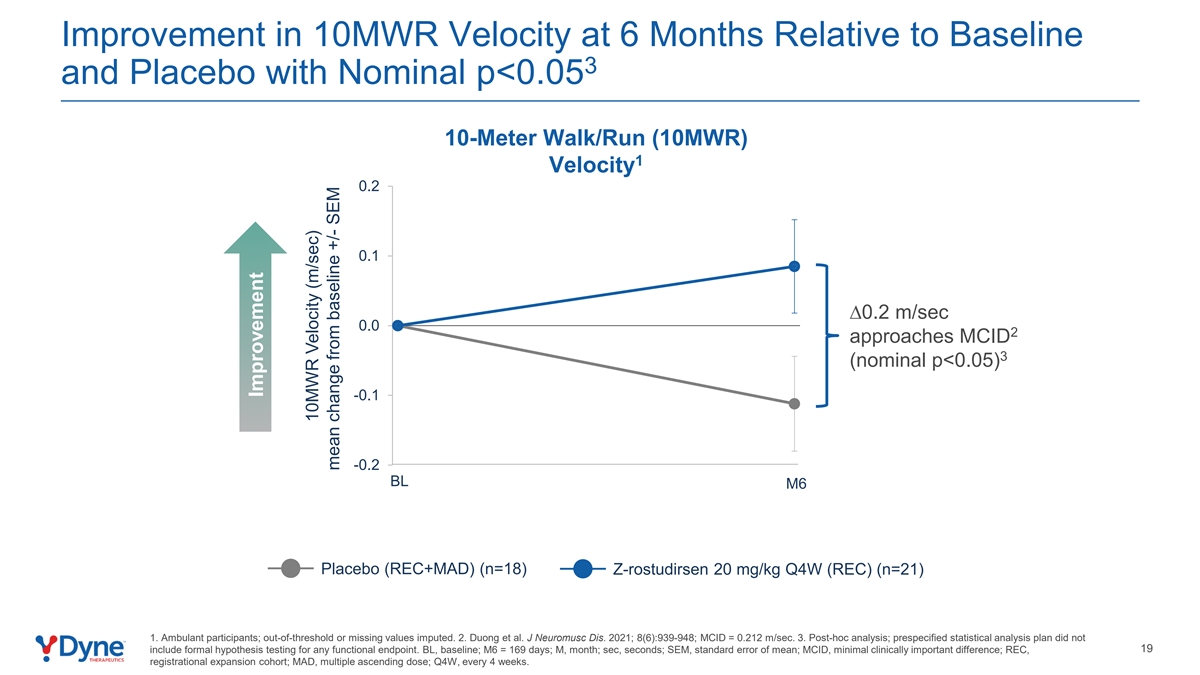
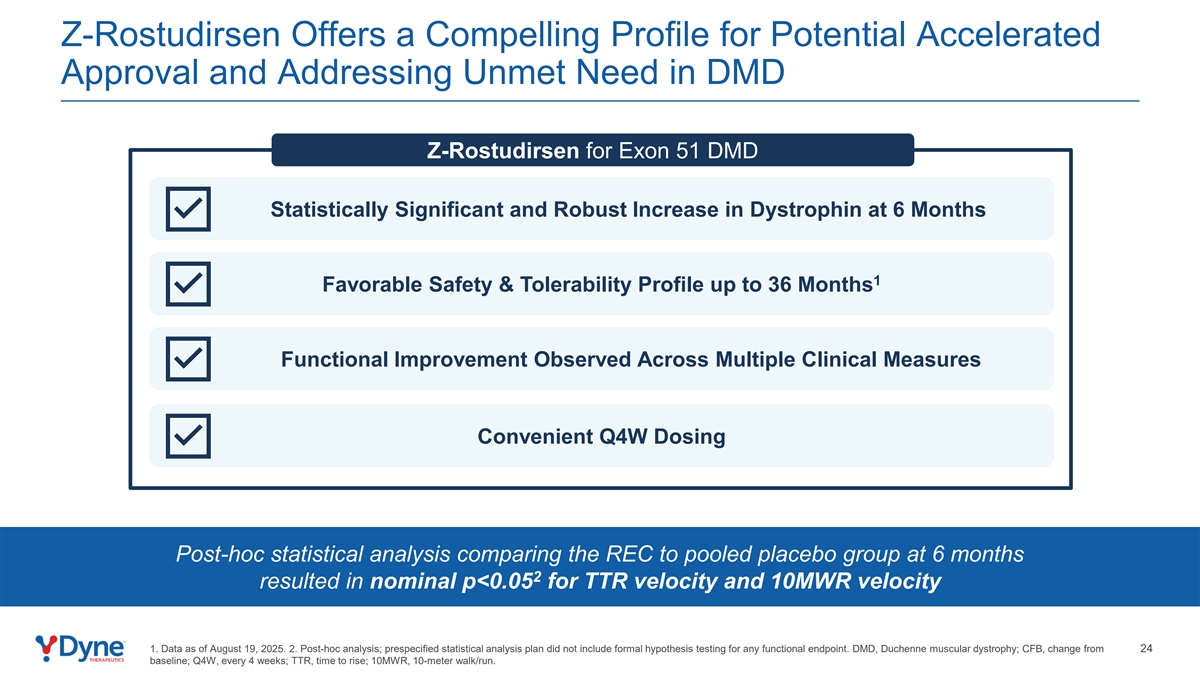
In addition, improvement relative to placebo was observed across all six prespecified functional endpoints from the topline readout of the REC. Two of these measures, Time to Rise (TTR) Velocity and 10-Meter Walk/Run (10MWR) Velocity, both improved relative to placebo at six months with a nominal p<0.05, even though the study was not powered to demonstrate statistical significance in any of the functional measures1. Importantly, lung function, the loss of which is a leading cause of mortality in DMD, as measured by Forced Vital Capacity Percent Predicted (FVC%p), was preserved at 6 months compared to a decline in placebo.
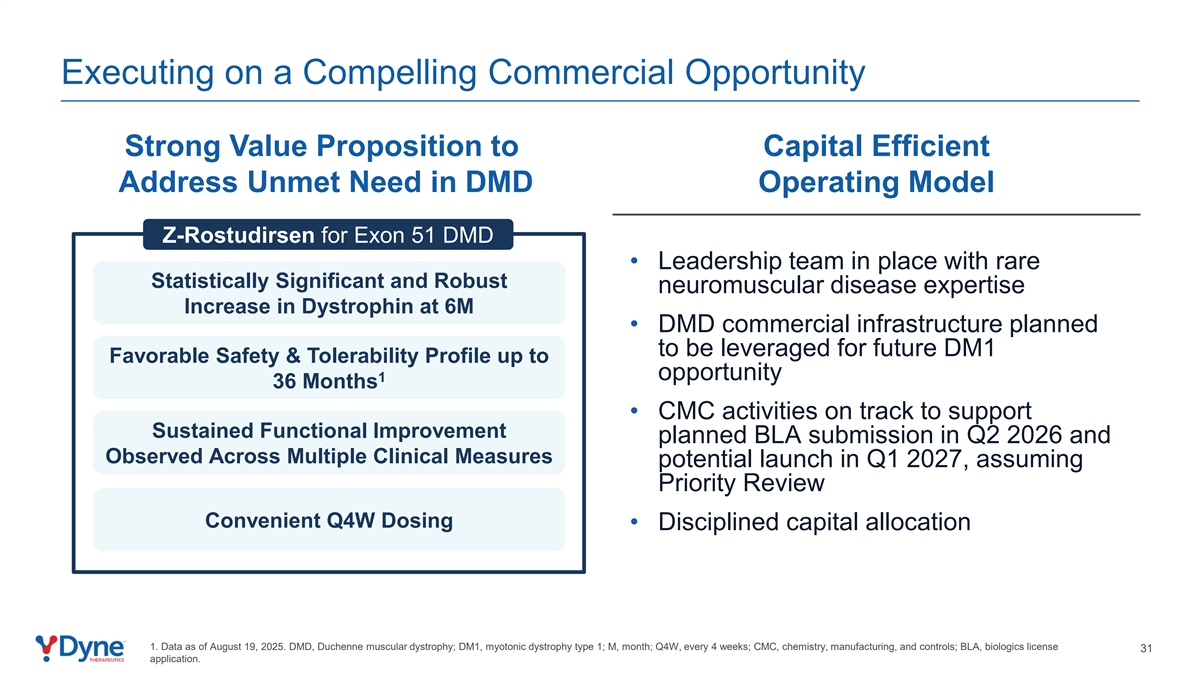
“With its high level of dystrophin expression, favorable safety profile, convenient monthly dosing regimen, and functional improvement as assessed by six prespecified clinical measures, z-rostudirsen has the potential to transform the care of those living with DMD amenable to exon 51 skipping,” said John Cox, president and chief executive officer of Dyne. “With these unprecedented clinical data in hand, we are on track to submit for U.S. Accelerated Approval in Q2 2026, positioning us for a potential
1
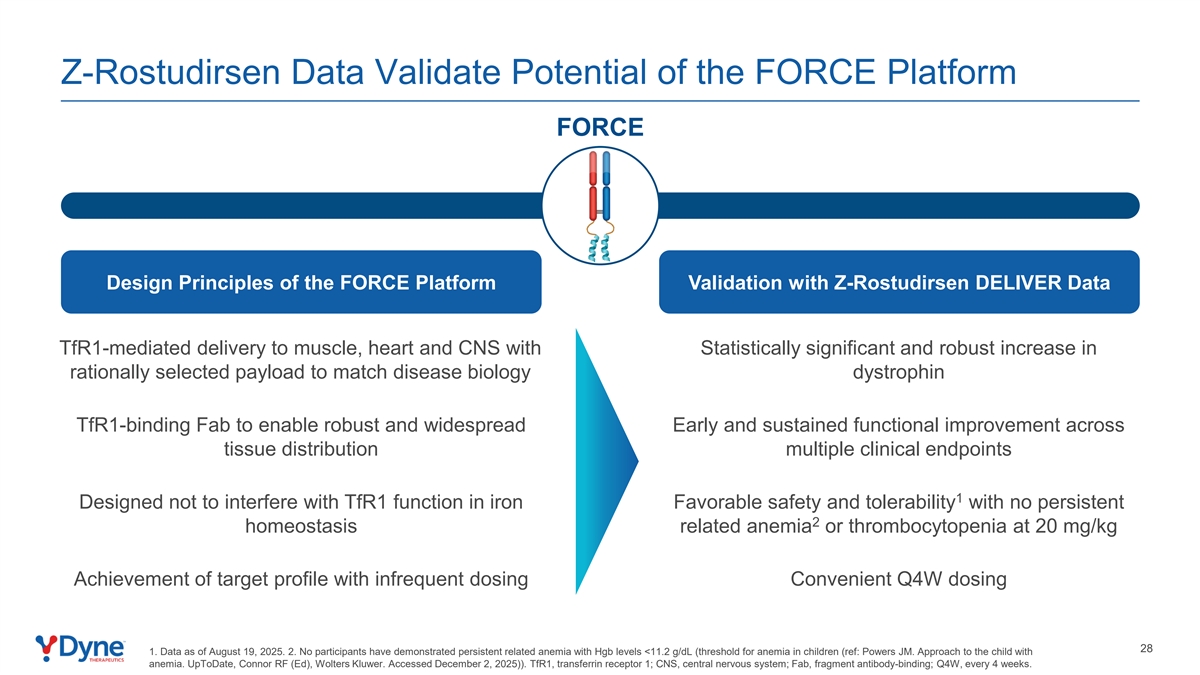
Q1 2027 launch, assuming Priority Review, into an established market of approximately 1,600 people with significant unmet need. In anticipation of approval, we have built a management team of medical, commercial and CMC experts to enable a capital efficient and successful launch. With this clinical validation, we are now in a position to leverage these capabilities and relationships in DMD to advance a broader portfolio of potential exon-skipping therapies with a total population of more than 4,000 individuals. Beyond the opportunity in DMD, we believe the compelling clinical results from our DELIVER study validate the power of our FORCE platform and its ability to deliver multiple potential products that could offer meaningful and sustained benefits for those living with other challenging neuromuscular diseases.”
“The Duchenne community has long awaited therapies that deliver meaningful and sustained functional improvement,” said Perry Shieh, M.D, Ph.D., professor of neurology and pediatrics at the David Geffen School of Medicine at UCLA, a neurologist at the Ronald Reagan UCLA Medical Center in Los Angeles, and a principal investigator for the DELIVER trial. “Our scientific understanding of the disease has led to a strong belief that restoring a sufficient level of near-full-length dystrophin expression in individuals with DMD could have the potential to significantly alter the trajectory of this disease. I am highly encouraged by these new results from the placebo-controlled Registrational Expansion Cohort and the longer-term portions of DELIVER, and I look forward to being able to offer z-rostudirsen to eligible DMD patients, if approved.”
“The data from all 86 participants of the DELIVER trial will form the basis for our planned U.S. Accelerated Approval submission,” said Doug Kerr, M.D., Ph.D., chief medical officer of Dyne. “We are deeply grateful to the clinical trial participants, their families, and physicians for their trust and commitment as we continue to advance this promising therapy. I believe that the clinical results from DELIVER, taken together, are unprecedented in terms of the breadth, magnitude and duration of effect, and this was only possible with the participation of and partnership with the Duchenne community.”
Positive Topline Efficacy Data from DELIVER Registrational Expansion Cohort (REC)
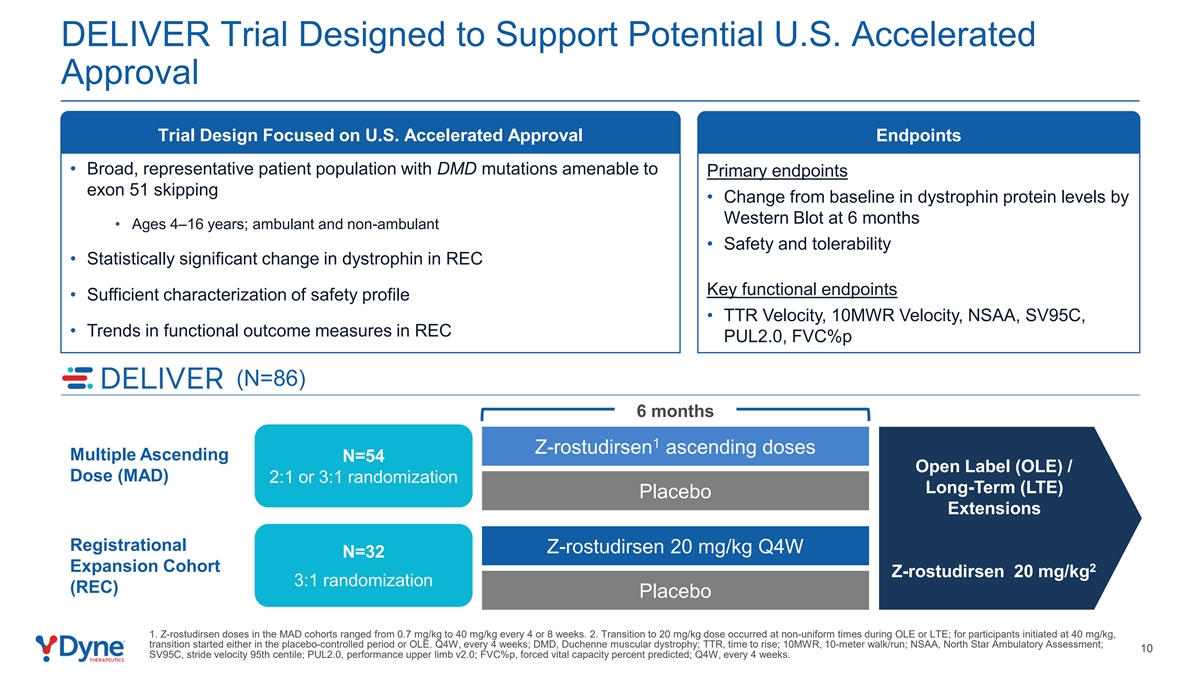
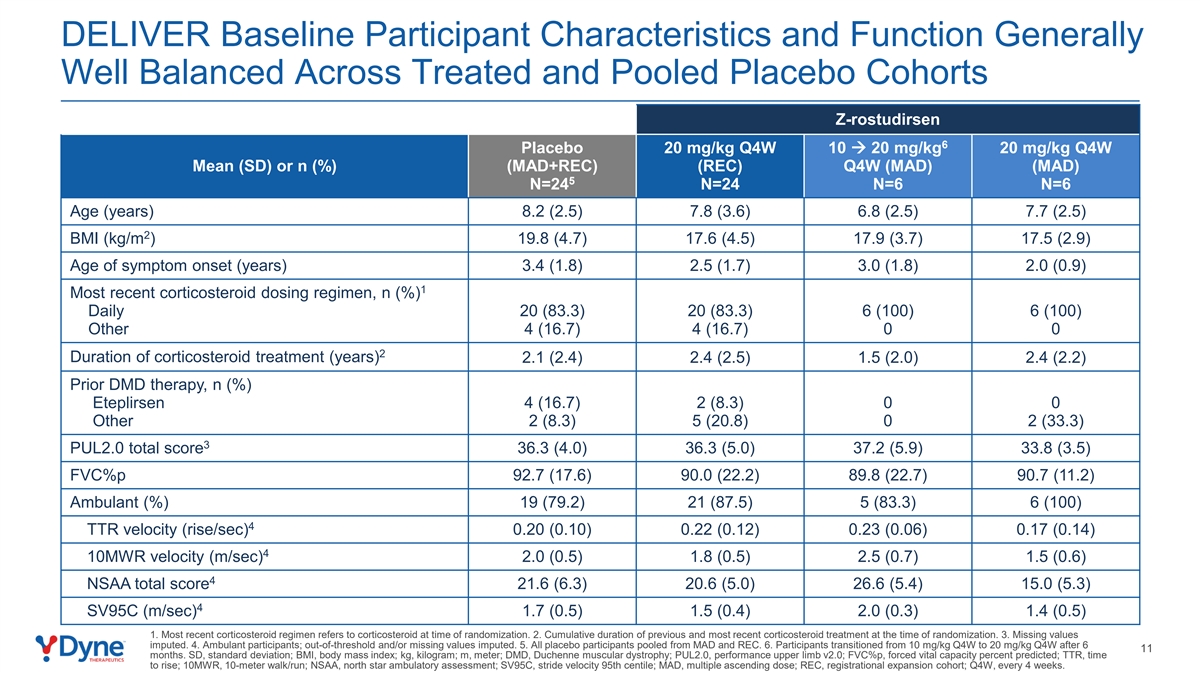
The REC of the DELIVER trial enrolled 32 ambulant and non-ambulant males with DMD who were ages 4 to 16 at baseline and have mutations amenable to exon 51 skipping. Of these, 24 participants were randomized to receive 20 mg/kg z-rostudirsen every four weeks (Q4W), and 8 were randomized to placebo. Key findings after six months include:
| • | Dystrophin: The REC met its primary endpoint, demonstrating a statistically significant change from baseline in muscle-content adjusted dystrophin expression (p < 0.0001), as measured by Western blot. Patients treated with 20 mg/kg z-rostudirsen Q4W reached a mean absolute dystrophin expression of 5.46% of normal (adjusted for muscle content). |
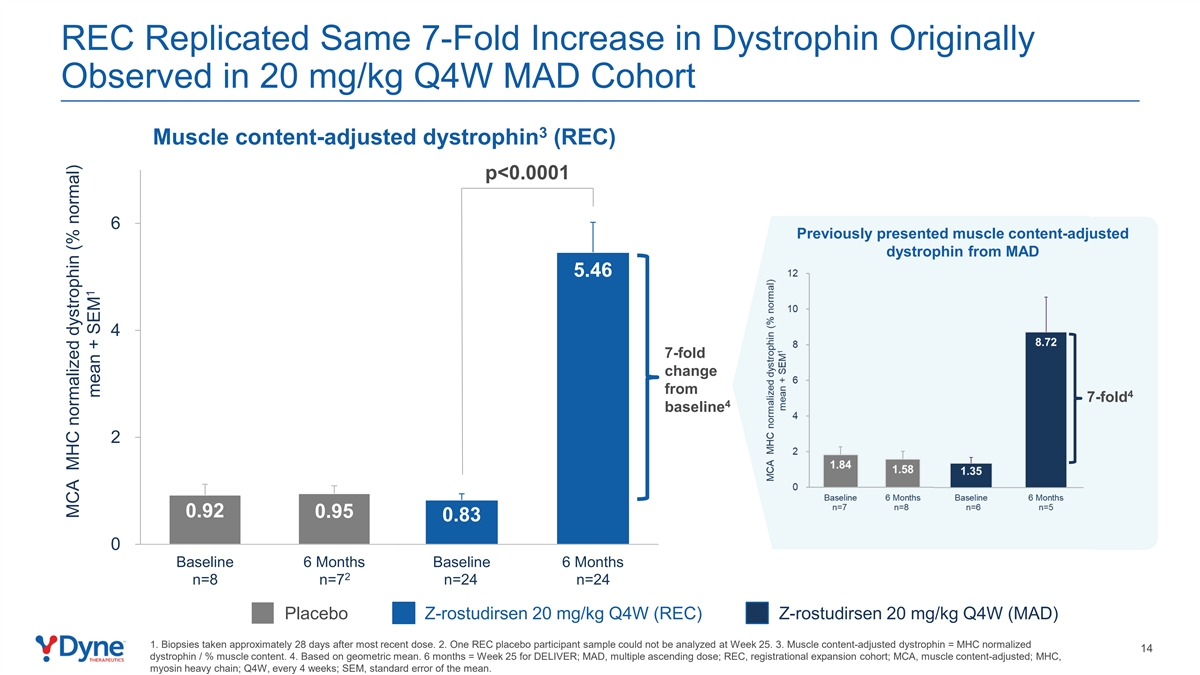
These results replicate the 7-fold increase in muscle-content adjusted dystrophin expression at six months reported previously from participants receiving 20 mg/kg z-rostudirsen Q4W in the multiple-ascending dose (MAD) portion of the DELIVER trial.
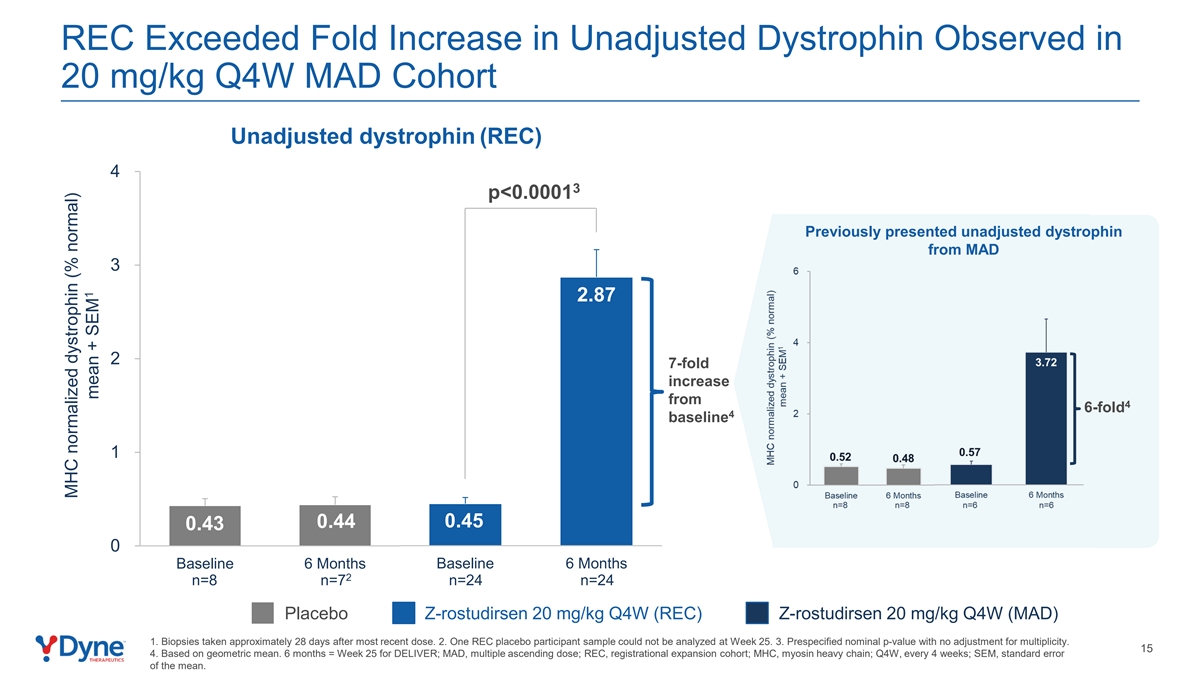
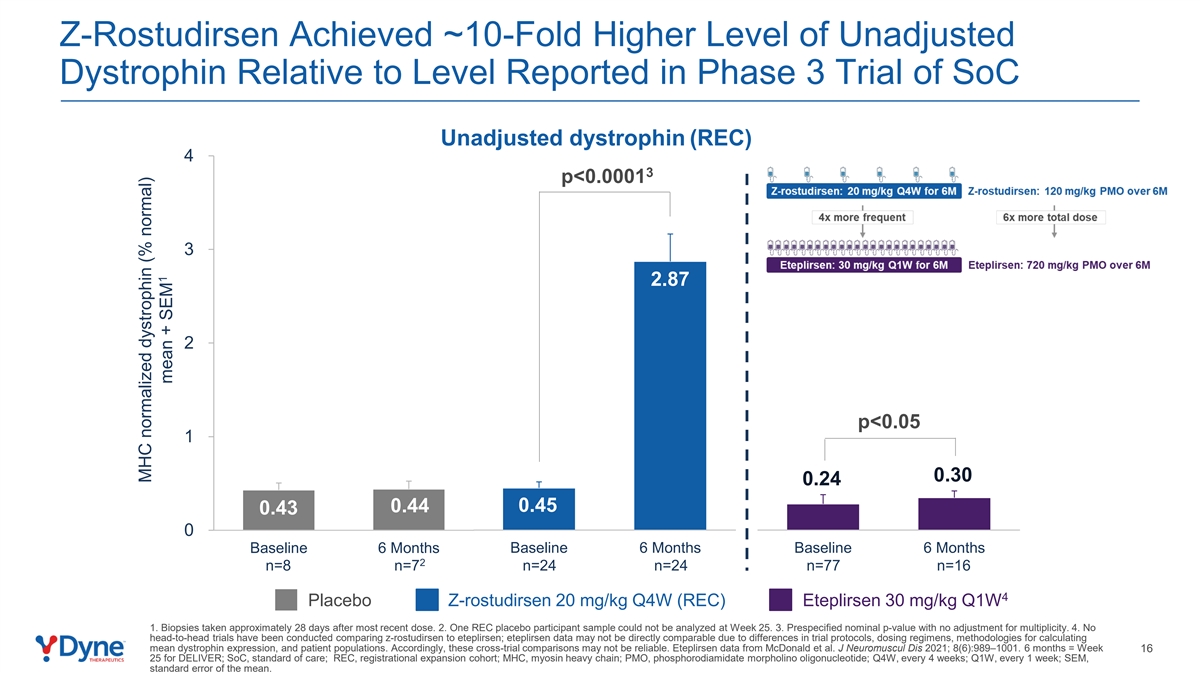
When unadjusted for muscle content, the mean absolute dystrophin expression among patients treated with 20 mg/kg z-rostudirsen Q4W was 2.87% of normal (p < 0.0001)2, approximately 10-fold higher than the 0.3% of normal reported in a clinical trial of the weekly standard of care for DMD exon 51 in the United States, eteplirsen3.
2
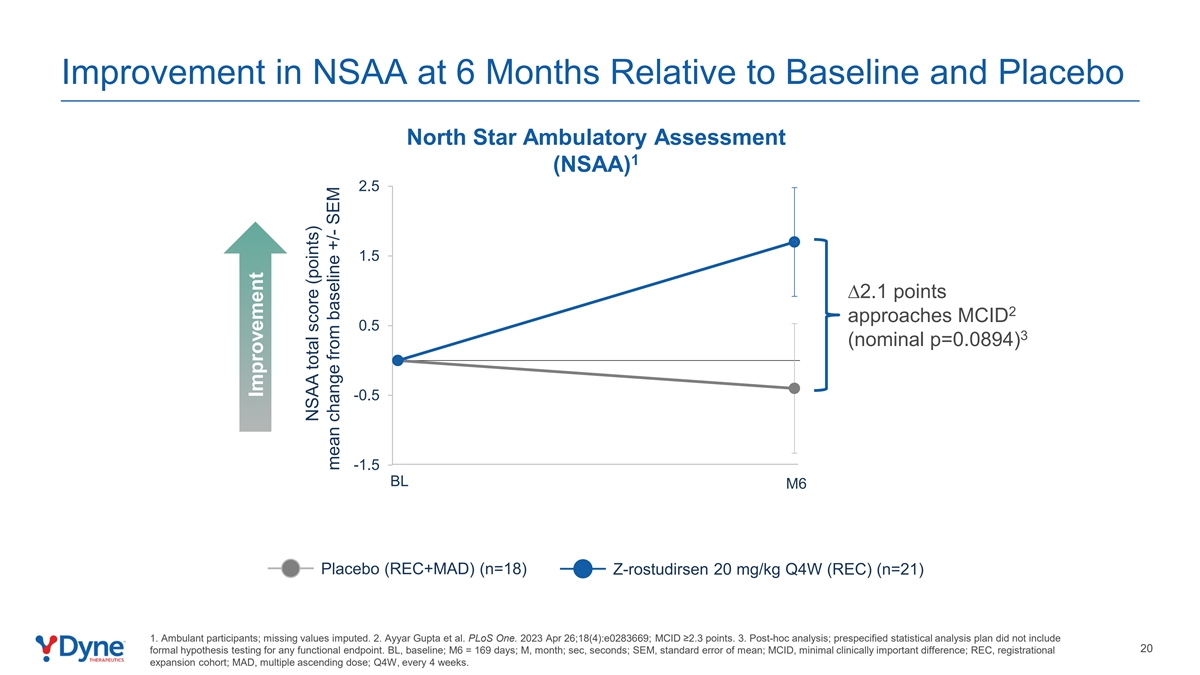
| • | Function: At six months, functional improvement was observed across multiple clinical endpoints relative to baseline and declines in the pooled placebo group (from the entire DELIVER trial per the statistical analysis plan), as assessed by the following ambulatory measures: |
| • | TTR Velocity (placebo n=18; z-rostudirsen n=21) |
| • | 10MWR Velocity (placebo n=18; z-rostudirsen n=21) |
| • | North Star Ambulatory Assessment (NSAA) (placebo n=18; z-rostudirsen n=21) |
Despite not being powered for formal comparisons, a post-hoc statistical analysis comparing the REC to the pooled placebo group at six months generated nominal p<0.05 for TTR Velocity and 10MWR Velocity1.
Functional improvement was also seen in:
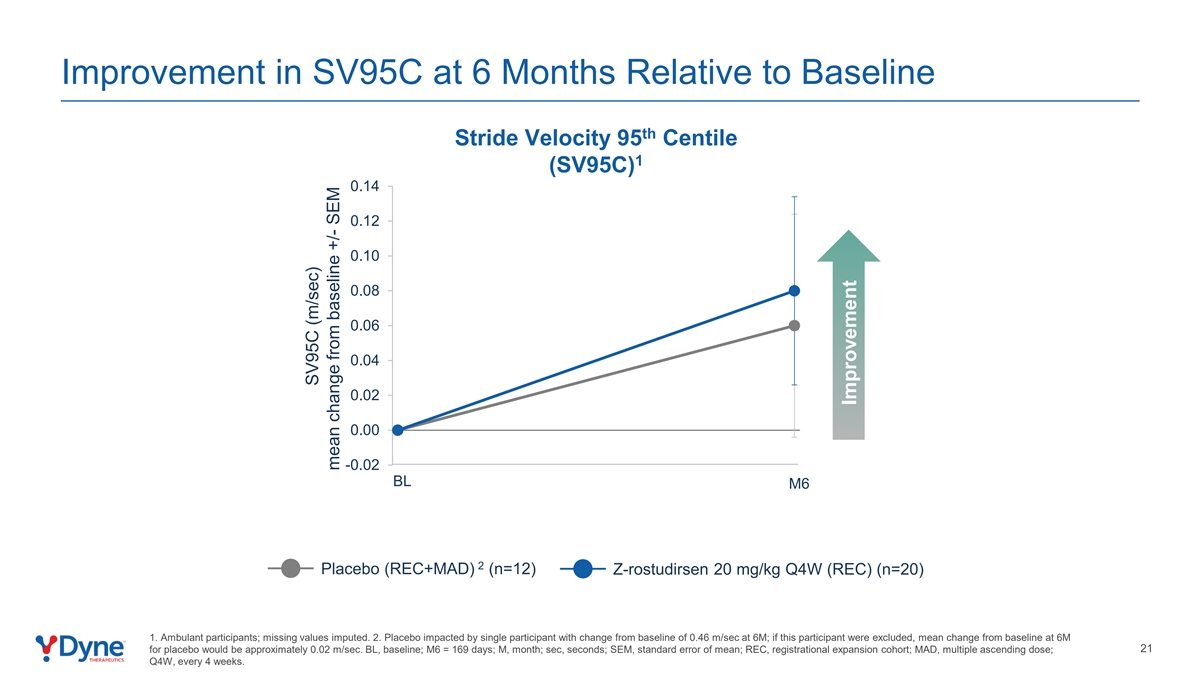
| • | Stride Velocity 95th Centile (SV95C), which improved from baseline and relative to placebo (placebo n=12, z-rostudirsen n=20). |
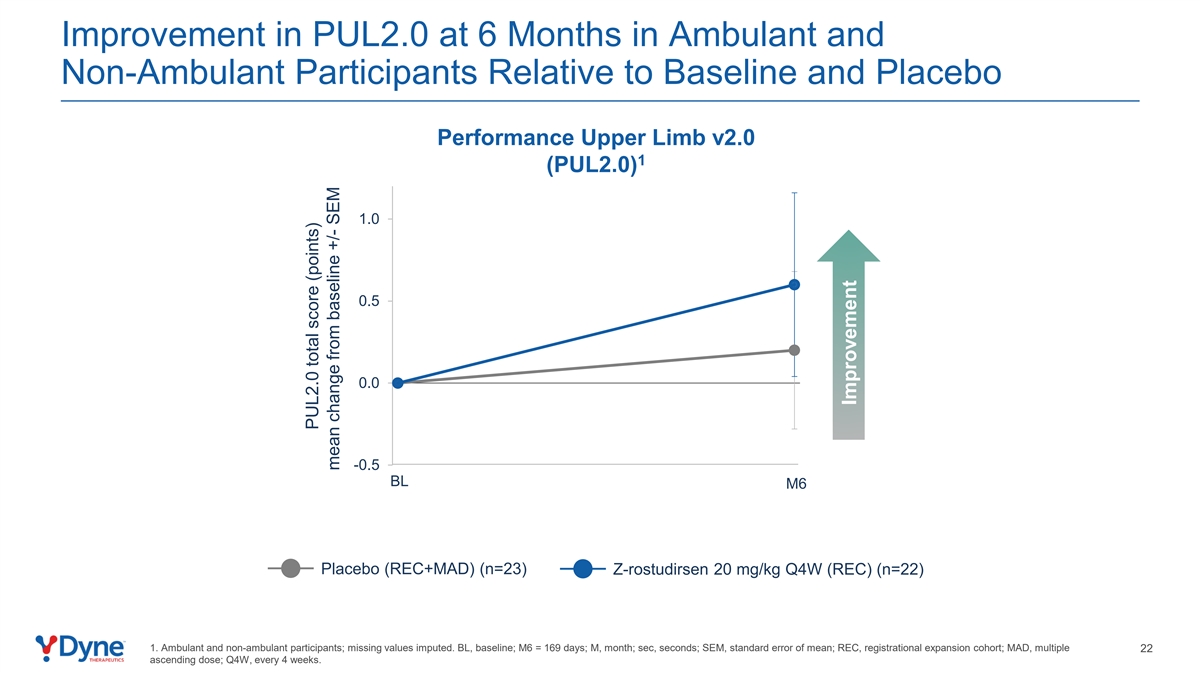
| • | Performance of Upper Limb (PUL2.0), which improved from baseline and relative to placebo (placebo n=23; z-rostudirsen n=22). |
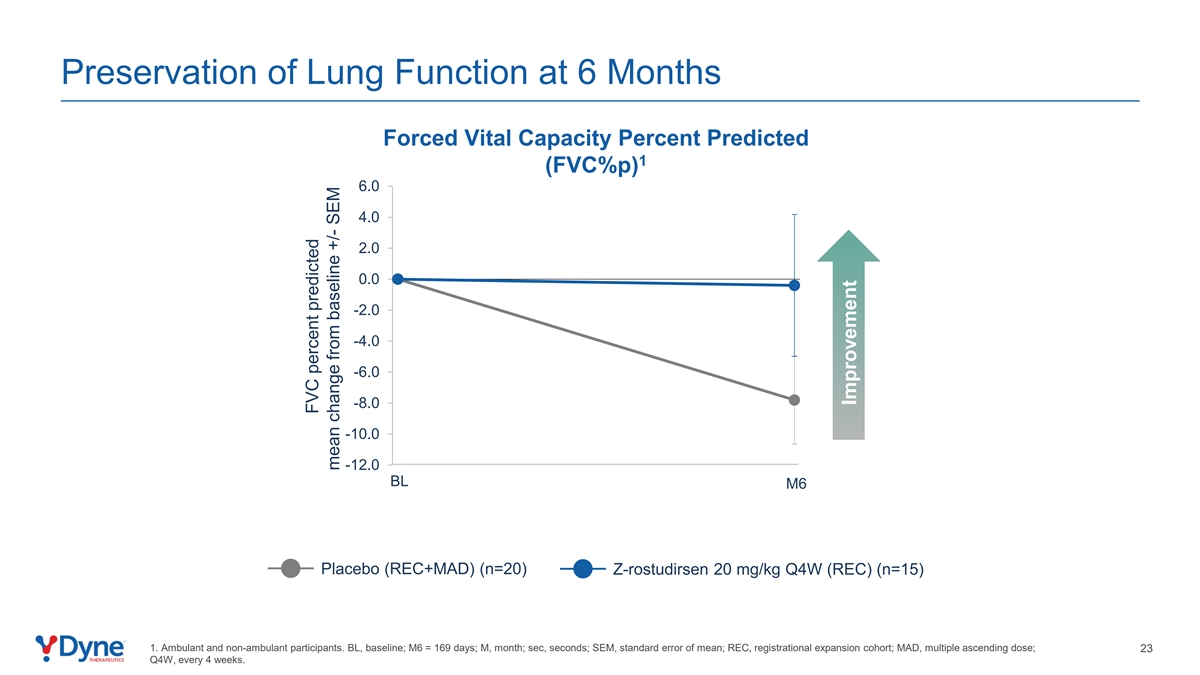
Preservation of lung function:
| • | FVC%p remained stable with clear separation from placebo, which declined (placebo n=20; z-rostudirsen n=15). In DMD, loss of pulmonary function is a leading cause of mortality4. |
Favorable Long-Term Safety & Tolerability Profile
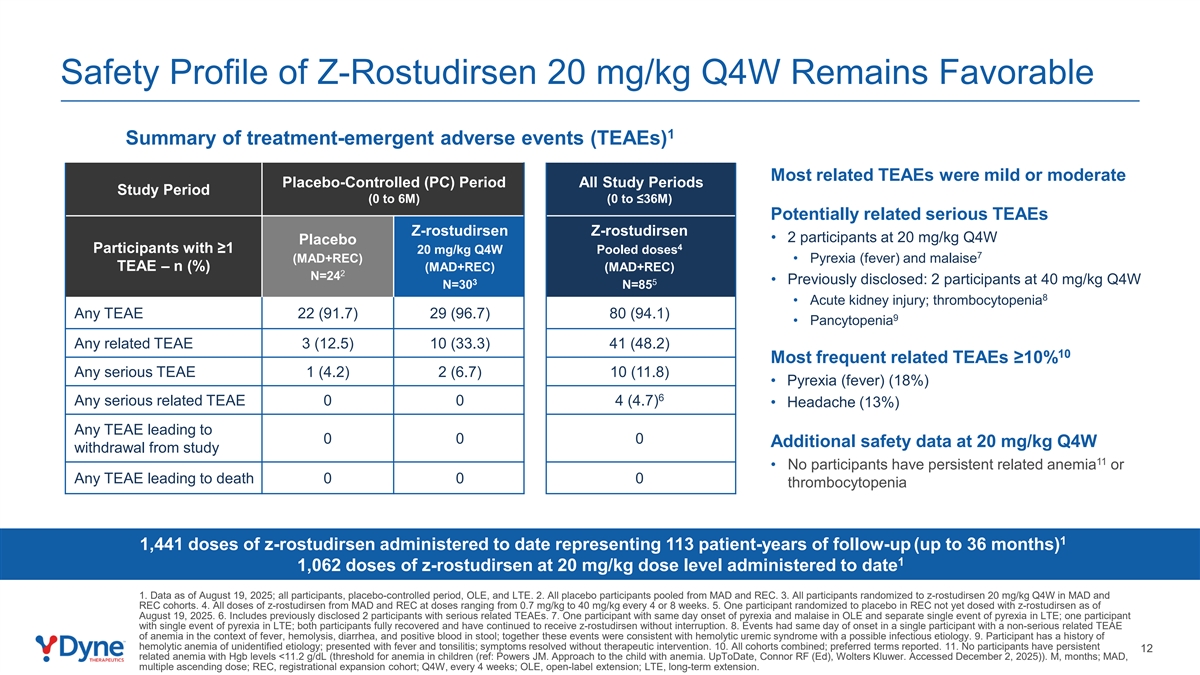
| • | Safety and tolerability data were based on 86 total participants enrolled in the DELIVER trial and followed for up to 36 months, including participants initially enrolled in the MAD cohorts (n=54) and REC (n=32) of the trial and who have transitioned to the OLE and LTE portions. Z-rostudirsen continued to demonstrate a favorable safety profile5, and most related treatment emergent adverse events (TEAEs) were mild or moderate. The most commonly reported related TEAEs were pyrexia (fever) and headache. No related serious TEAEs were observed in the REC. Since the last safety update, two participants in the OLE/LTE portion of the trial experienced malaise and/or pyrexia (fever) which were reported as related serious TEAEs. Both of these participants fully recovered and have continued to receive z-rostudirsen without interruption. |
| • | Approximately 1,441 doses of z-rostudirsen, including 1,062 at the 20 mg/kg Q4W dose, have been administered to date in the DELIVER trial, representing 113 patient-years of follow-up5. |
3
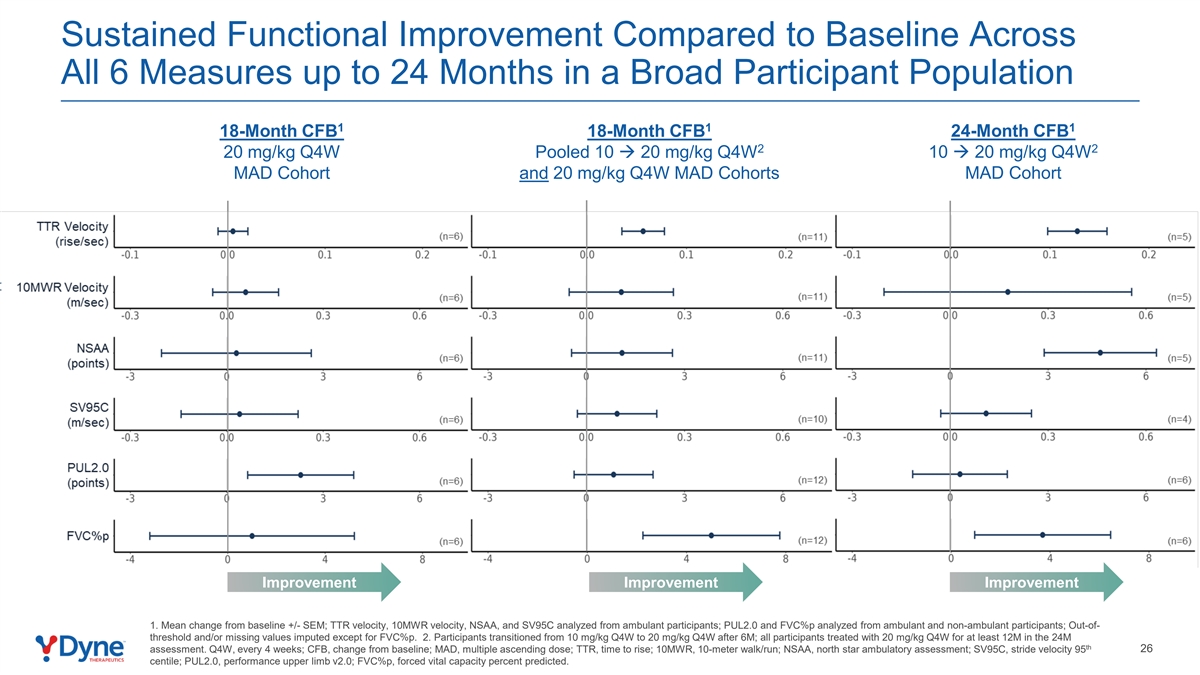
New Positive Long-term Results from DELIVER Trial Showed Sustained Functional Improvement Across All Assessed Endpoints Out to 24 Months
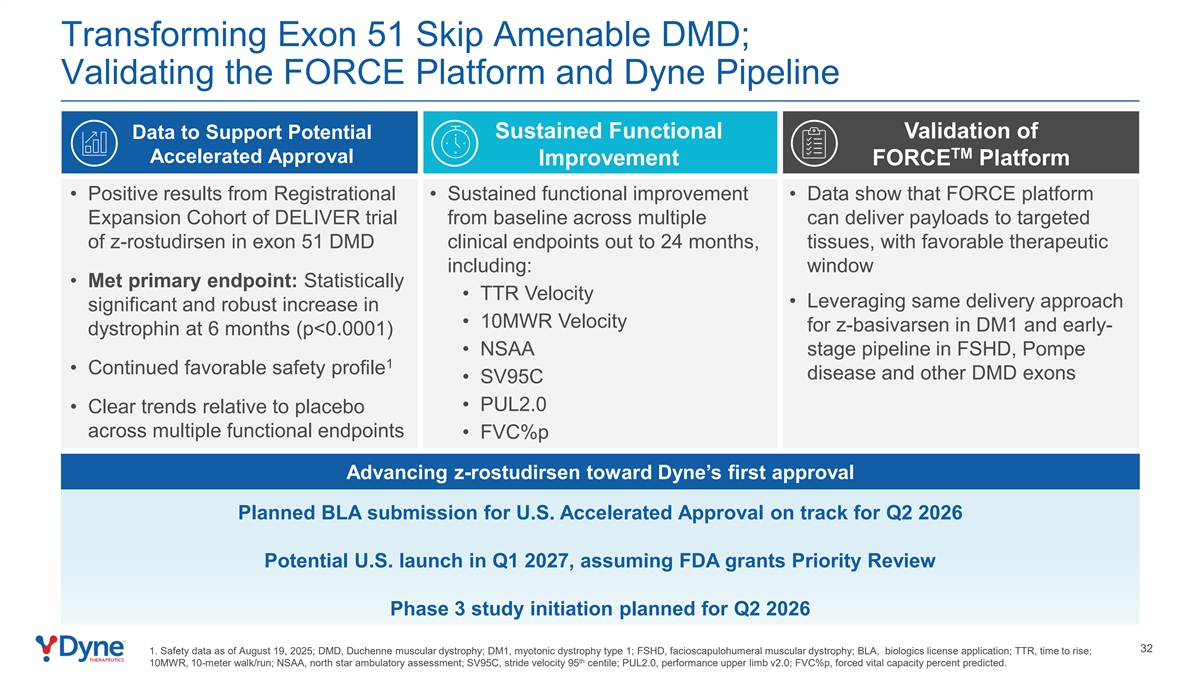
Sustained functional improvement in TTR Velocity, 10MWR Velocity, NSAA, SV95C, PUL2.0, and FVC%p from baseline were observed in the following groups from the OLE and LTE portions of the DELIVER trial:
| • | 24-month functional data from the 6 participants treated with z-rostudirsen in the 10 mg/kg Q4W cohort of the MAD who were dose escalated to 20 mg/kg Q4W in the OLE period. |
| • | 18-month functional data from the 6 participants treated with z-rostudirsen in the 20 mg/kg Q4W MAD cohort. |
| • | Pooled 18-month functional data from both cohorts. |
Key Milestones for Z-Rostudirsen
| • | Dyne plans to submit a BLA (Biologics License Application) for U.S. Accelerated Approval in Q2 2026. |
| • | Dyne plans to initiate a global Phase 3 clinical trial of z-rostudirsen in Q2 2026 to support global approvals. |
| • | Dyne continues to expect a potential U.S. launch of z-rostudirsen in Q1 2027, assuming FDA grants Priority Review. |
| • | Dyne also continues to pursue approval pathways outside of the U.S. for z-rostudirsen in patients with DMD who are amenable to exon 51 skipping. |
Investor Webcast
Dyne will host a conference call and webcast to discuss these updates today, December 8, 2025, at 8:00 a.m. ET and a replay will be accessible for 90 days following the presentation. An accompanying slide presentation for the event and an updated corporate presentation will also be available. To access these presentations and register for the webcast and replay, please visit the Investors & Media section of Dyne’s website at https://investors.dyne-tx.com/news-and-events/events-and-presentations .
About the DELIVER Trial
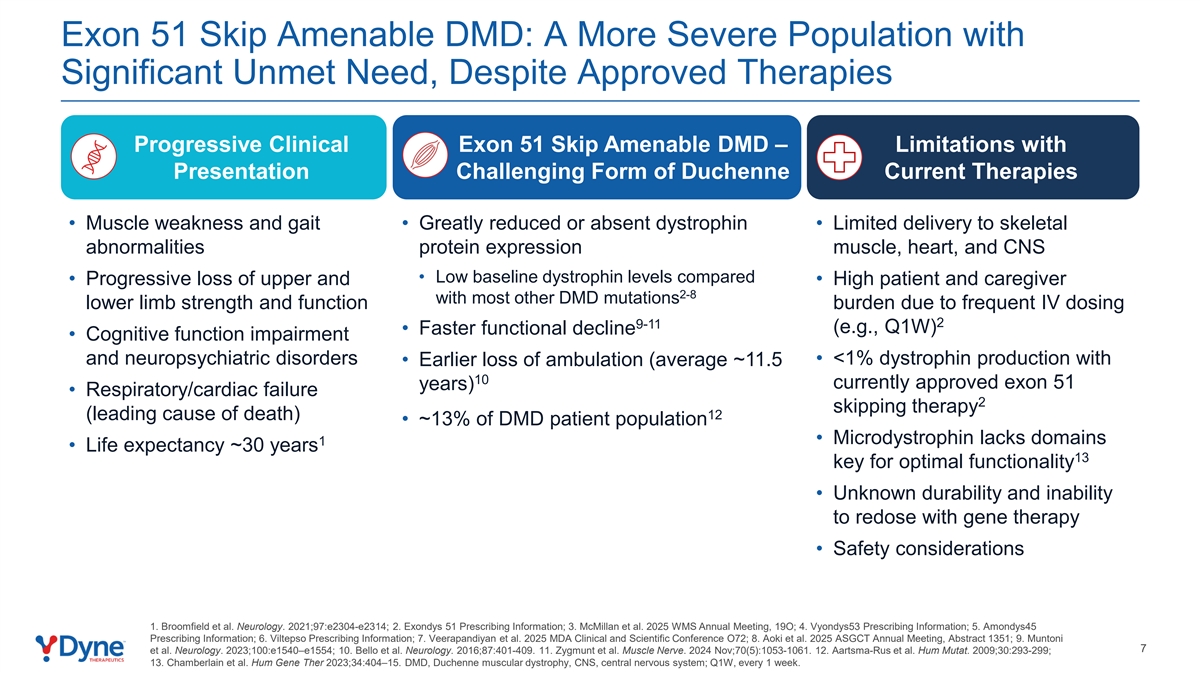
DELIVER is a global, randomized, placebo-controlled, double-blind, Phase 1/2 clinical trial that evaluated the safety, tolerability and efficacy (as measured by both biomarker and functional improvement) of zeleciment rostudirsen (z-rostudirsen, also known as DYNE-251) in individuals with Duchenne muscular dystrophy (DMD) who have mutations in the DMD gene that are amenable to exon 51 skipping. Individuals with DMD amenable to exon 51 skipping typically show lower baseline dystrophin levels compared to those with DMD amenable to the skipping of certain other exons6-15. The multiple ascending dose (MAD) portion of the study resulted in the selection of a registrational dose and regimen of 20 mg/kg of z-rostudirsen administered every four weeks. The placebo-controlled portion of the registrational expansion cohort (REC) to support a potential regulatory submission for U.S. Accelerated Approval has been completed. The primary endpoint for this cohort was the change from baseline in dystrophin protein levels as measured by Western blot at 6 months. Participants from the MAD and REC portions had the option to enroll in the open-label extension and long-term extension portions of the study. For more information on the DELIVER trial, visit clinicaltrials.gov and euclinicaltrials.eu.
4
About zeleciment rostudirsen (z-rostudirsen, also known as DYNE-251)
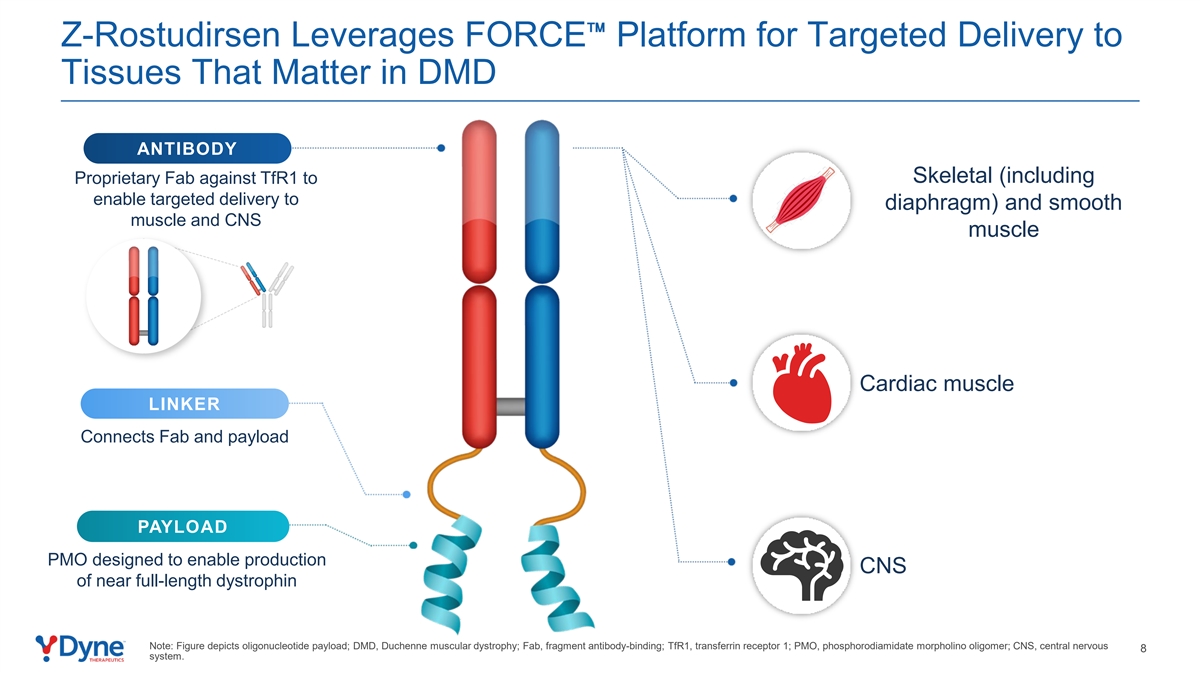
Z-rostudirsen is an investigational therapeutic being evaluated in the Phase 1/2 global DELIVER clinical trial for individuals with DMD who have mutations in the DMD gene that are amenable to exon 51 skipping. Z-rostudirsen consists of a phosphorodiamidate morpholino oligomer (PMO) conjugated to an antigen-binding fragment (Fab) that binds to the transferrin receptor 1 (TfR1). It is designed to enable the production of near full-length dystrophin in muscle and the central nervous system (CNS) to provide functional improvement. Z-rostudirsen has received Breakthrough Therapy, Fast Track and Rare Pediatric Disease designations from the U.S. Food and Drug Administration (FDA), as well as Orphan Drug designation from the FDA and European Medicines Agency (EMA) and the Ministry of Health, Labour and Welfare (MHLW) in Japan for the treatment of individuals with DMD amenable to exon 51 skipping.
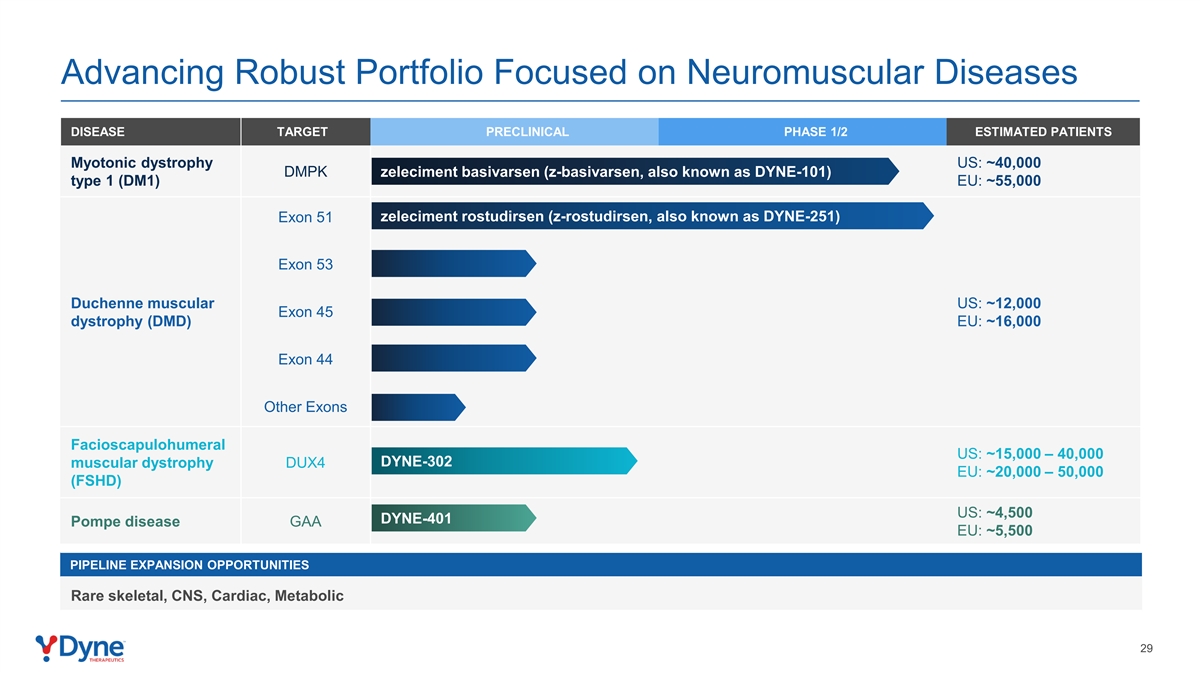
In addition to z-rostudirsen, Dyne is building a DMD franchise and has preclinical programs targeting other exons, including 53, 45 and 44.
About Duchenne Muscular Dystrophy (DMD)
Duchenne muscular dystrophy (DMD) is a rare X-linked progressive neuromuscular disorder caused by mutations in the DMD gene. These mutations result in a complete or near-complete absence of dystrophin, a protein critical for maintaining muscle structure and function. DMD is the most common form of childhood-onset muscular dystrophy, affecting approximately 12,000 individuals in the U.S. and 16,000 in the EU. Symptoms typically emerge between ages 3 and 5, beginning with muscle weakness in the upper arms, thighs and pelvic region, and progressively impacting the lower limbs, forearms, neck and trunk. In addition to physical decline, individuals may experience cognitive impairment and neuropsychiatric challenges such as intellectual disabilities, learning difficulties and behavioral disorders. Despite existing therapies, there remains a significant unmet need for new treatment options that deliver functional improvement.
About Dyne Therapeutics
Dyne Therapeutics is focused on delivering functional improvement for people living with genetically driven neuromuscular diseases. We are developing therapeutics that target muscle and the central nervous system (CNS) to address the root cause of disease. The company is advancing clinical programs for myotonic dystrophy type 1 (DM1) and Duchenne muscular dystrophy (DMD), and preclinical programs for facioscapulohumeral muscular dystrophy (FSHD) and Pompe disease. At Dyne, we are on a mission to deliver functional improvement for individuals, families and communities. Learn more at https://www.dyne-tx.com/ and follow us on X, LinkedIn and Facebook.
5
Forward-Looking Statements
This press release contains forward-looking statements that involve substantial risks and uncertainties. All statements, other than statements of historical facts, contained in this press release, including statements regarding Dyne’s strategy, future operations, prospects and plans, objectives of management, the potential of the FORCETM platform, expectations regarding the timing and outcome of interactions with and submissions to global regulatory authorities and anticipated timelines for submission for regulatory approval and launch of z-rostudirsen, constitute forward-looking statements within the meaning of The Private Securities Litigation Reform Act of 1995. The words “anticipate,” “believe,” “continue,” “could,” “estimate,” “expect,” “intend,” “may,” “might,” “objective,” “ongoing,” “plan,” “predict,” “project,” “potential,” “should,” “will,” or “would,” or the negative of these terms, or other comparable terminology are intended to identify forward-looking statements, although not all forward-looking statements contain these identifying words. Dyne may not actually achieve the plans, intentions or expectations disclosed in these forward-looking statements, and you should not place undue reliance on these forward-looking statements. Actual results or events could differ materially from the plans, intentions and expectations disclosed in these forward-looking statements as a result of various important factors, including: uncertainties inherent in the identification and development of product candidates, including the initiation and completion of preclinical studies and clinical trials; uncertainties as to the availability and timing of results from preclinical studies and clinical trials; the timing of and Dyne’s ability to enroll patients in clinical trials; whether results from preclinical studies and initial data from early clinical trials will be predictive of the final results of the clinical trials or future trials; uncertainties as to the FDA’s and other regulatory authorities’ interpretation of the data from Dyne’s clinical trials and acceptance of Dyne’s clinical programs and the regulatory approval process, including the availability of accelerated approval pathways; whether Dyne’s cash resources will be sufficient to fund its foreseeable and unforeseeable operating expenses and capital expenditure requirements; as well as the risks and uncertainties identified in Dyne’s filings with the Securities and Exchange Commission (SEC), including the Company’s most recent Form 10-Q and in subsequent filings Dyne may make with the SEC. In addition, the forward-looking statements included in this press release represent Dyne’s views as of the date of this press release. Dyne anticipates that subsequent events and developments will cause its views to change. However, while Dyne may elect to update these forward-looking statements at some point in the future, it specifically disclaims any obligation to do so. These forward-looking statements should not be relied upon as representing Dyne’s views as of any date subsequent to the date of this press release.
| 1. | Post-hoc analysis; prespecified statistical analysis plan did not include formal hypothesis testing for any functional endpoint. |
| 2. | Prespecified nominal p-value with no adjustment for multiplicity. |
| 3. | No head-to-head trials have been conducted comparing z-rostudirsen to eteplirsen. Eteplirsen data may not be directly comparable due to differences in trial protocols, dosing regimens, methodologies for calculating mean dystrophin expression, and patient populations. Accordingly, these cross-trial comparisons may not be reliable. Eteplirsen data from McDonald et al. J Neuromuscul Dis. 2021; 8(6): 989–1001. |
| 4. | Cheeran D., Khan S., et al. (2017). Predictors of Death in Adults With Duchenne Muscular Dystrophy-Associated Cardiomyopathy. J Am Heart Assoc 6(10): e006340. |
| 5. | Z-rostudirsen safety data as of August 19, 2025. |
| 6. | Exondys51 Prescribing Information. |
| 7. | McMillan H, et al. 2025 WMS Annual Meeting, 19O. |
| 8. | Vyondys53 Prescribing Information. |
| 9. | Amondys45 Prescribing Information. |
6
| 10. | Viltepso Prescribing Information. |
| 11. | Veerapandiyan A, et al. 2025 MDA Clinical and Scientific Conference O72. |
| 12. | Aoki Y, et al. 2025 ASGCT Annual Meeting, Abstract 1351. |
| 13. | Muntoni F, et al. Neurology. 2023;100:e1540–e1554. |
| 14. | BelloL, et al. Neurology. 2016;87:401-409. |
| 15. | Zygmunt et al. Muscle Nerve. 2024 Nov;70(5):1053-1061. 12. Aartsma-Rus A, et al. Hum Mutat. 2009;30:293-299. |
Contacts:
Investors
Mia Tobias
781-317-0353
Media
Stacy Nartker
781-317-1938
7