Exhibit 99.1

Nasdaq: LGVN October 2021 Cell Therapy for Aging - Related Disease & Life - Threatening Conditions
Forward Looking Statements 2 Certain statements in this presentation that are not historical facts are forward - looking statements that reflect management's current expectations, assumptions, and estimates of future performance and economic conditions, and involve risks and uncertainties that could cause actual results to differ materially from those anticipated by the statements made herein . Forward - looking statements are generally identifiable by the use of forward - looking terminology such as "believe," "expects," "may," "looks to," "will," "should," "plan," "intend," "on condition," "target," "see," "potential," "estimates," "preliminary," or "anticipates" or the negative thereof or comparable terminology, or by discussion of strategy or goals or other future events, circumstances, or effects . Moreover, forward - looking statements in this release include, but are not limited to, statements about the ability of our clinical trials to demonstrate safety and efficacy of our product candidates, and other potentially positive or negative results ; the timing, focus and potential outcomes of our ongoing and future preclinical studies and clinical trials ; the size of the market opportunity for our product candidates, the beneficial characteristics, safety, efficacy and therapeutic effects of our product candidates ; our ability to obtain and maintain regulatory approval of our product candidates, our plans and ability to obtain or protect intellectual property rights, including extensions of existing patent terms where available and our ability to avoid infringing the intellectual property rights of others . Further information relating to factors that may impact the Company's results and forward - looking statements are disclosed in the Company's filings with the Securities and Exchange Commission (SEC), including our Annual Report on Form 10 - K filed with the SEC on March 30 , 2021 . The forward - looking statements contained in this presentation are made as of the date of this presentation, and the Company disclaims any intention or obligation, other than imposed by law, to update or revise any forward - looking statements, whether as a result of new information, future events, or otherwise .
Longeveron At - a - Glance (NASDAQ: LGVN) 3 Biotechnology Regenerative Medicine / Cell Therapy 2014 February 12, 2021 $21.4 million (June 30, 2021) Industry Sect o r Found ed IP O Cash Lo cat ion Miami, Florida (Corporate headquarters, manufacturing, research and development)
Longeveron: Developing Cell Therapy For Aging - Related Disease & Life - Threatening Conditions • Lead investigational therapeutic: Lomecel - B Œ (Allogeneic (donor - derived) medicinal signaling cells (MSCs)) – MSCs isolated from the bone marrow of young healthy adult donors • Lomecel - B produced in Longeveron’s state - of - the - art cGMP facility (Miami, FL) • Research Programs in U.S., Japan and the Bahamas • Clinical trial data evaluating Lomecel - B in three indications/conditions: • Alzheimer’s disease (Ph. 1): Well - tolerated; no evidence of ARIA; exploratory cognitive function & biomarker data • Aging Frailty (Ph. 2b): Well - tolerated; significant, dose - dependent increase in walking distance • Hypoplastic Left Heart Syndrome (Ph. 1): W ell - tolerated; no Major Adverse Cardiac Events (MACE) • Programs awarded ~$15 million in non - dilutive grant funds to date (NIA, NHLBI, Alz. Association & MSCRF) • Anticipated* near - term events/milestones: » Q4: Additional biomarker data from Phase 2b Aging Frailty US Trial » Q4 ‘21/Q1 ‘22: Top line data from Aging Frailty Influenza Vaccine Phase 1/2 “HERA” Trial » Q4 ‘21/Q1 ‘22: Initiate Alzheimer’s Disease Phase 2 Trial » Q4 ‘21/Q1 ‘22: Initiate Japan Phase 2 Aging Frailty Trial 4 *Anticipated event timeline, subject to adjustment and change. ARIA=amyloid related imaging abnormalities; NIA=National Institute on Aging; NHLBI=National Heart, Lung and Blood Institute; MSCRF - Maryland Stem Cell Research Fund
Lomecel - B Medicinal Signaling Cells (MSC) Cell Therapy 5
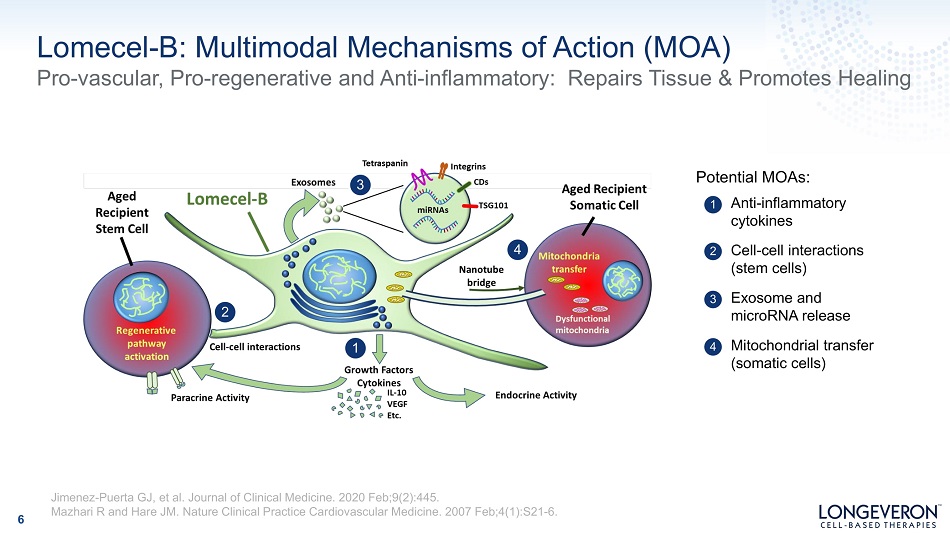
Lomecel - B: Multimodal Mechanisms of Action (MOA) Pro - vascular, Pro - regenerative and Anti - inflammatory: Repairs Tissue & Promotes Healing 6 1 A nt i - i nf l ammator y cytokines 2 3 Exosome and m ic ro RNA re l ease 4 Mitochondrial transfer (somatic cells) Cell - cell interactions (stem cells) 1 2 3 4 Potential MOAs: Jimenez - Puerta GJ, et al. Journal of Clinical Medicine. 2020 Feb;9(2):445. Mazhari R and Hare JM. Nature Clinical Practice Cardiovascular Medicine. 2007 Feb;4(1):S21 - 6.
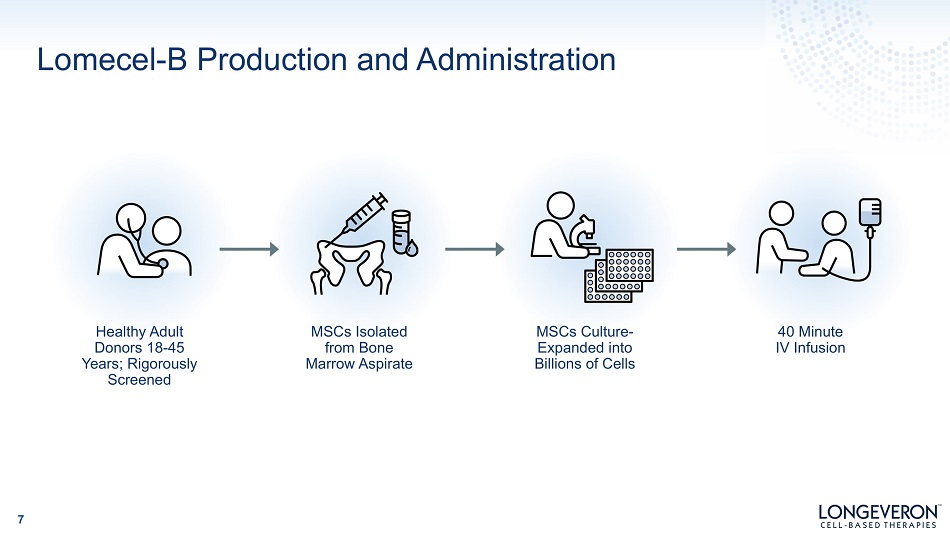
Lomecel - B Production and Administration 7 Healthy Adult Donors 18 - 45 Years; Rigorously Screened MSCs Isolated from Bone Marro w Aspi rat e MSCs Culture - Expanded into Billions of Cells 40 Minute IV Infusion
Lomecel - B: Proprietary, Scalable, “Off - the - Shelf” Cellular Therapy 8 • Robust quality assurance processes ensure batch - to - batch consistency • Cryogenically stored long - term, easy to prepare and administer • Delivered systemically or locally • In response to inflammatory mediators, MSCs home to sites of tissue damage 1 • Not perceived by the host as foreign (Immuno - evasive) 2 K e y A dvantages of Lomecel - B 1 Rustad KC, and Gurtner GC. Advances in wound care. 2012 Aug 1;1(4):147 - 52. 2 Ankrum JA, Ong JF, Karp JM. Mesenchymal stem cells: immune evasive, not immune privileged. Nature biotechnology. 2014 Mar;32(3):252 - 60.
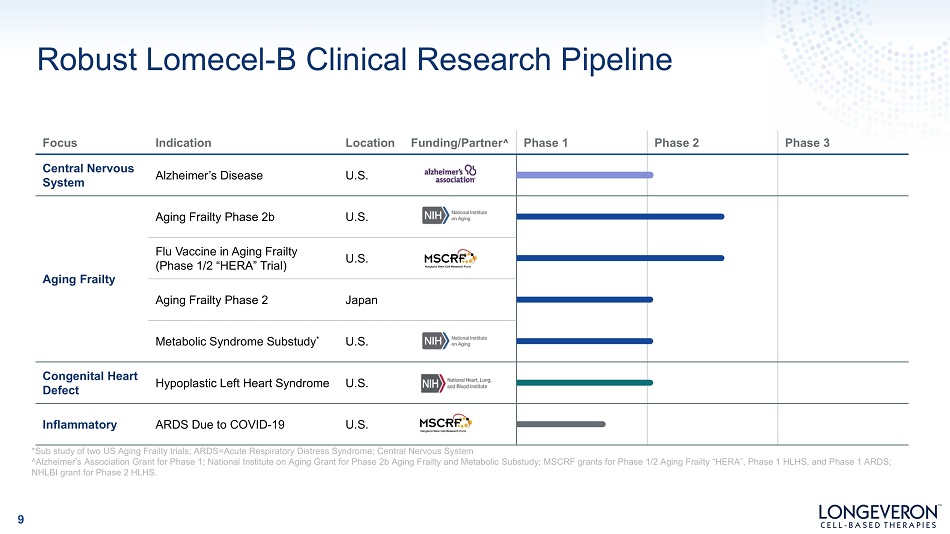
Robust Lomecel - B Clinical Research Pipeline Focus Indication Location Funding/Partner ^ Phase 1 Phase 2 Phase 3 Central Nervous System Alzheimer’s Disease U.S. Aging Frailty Aging Frailty Phase 2b U.S. Flu Vaccine in Aging Frailty (Phase 1/2 “HERA” Trial) U.S. Aging Frailty Phase 2 Japan Metabolic Syndrome Substudy * U.S. Congenital Heart Defect Hypoplastic Left Heart Syndrome U.S. Inflammatory ARDS Due to COVID - 19 U.S. *Sub study of two US Aging Frailty trials; ARDS=Acute Respiratory Distress Syndrome; Central Nervous System ^Alzheimer’s Association Grant for Phase 1; National Institute on Aging Grant for Phase 2b Aging Frailty and Metabolic Substudy; MSCRF grants for Phase 1/2 Aging Frailty “HERA”, Phase 1 HLHS, and Phase 1 ARDS; NHLBI grant for Phase 2 HLHS. 9

Lomecel - B Clinical Research Alzheimer’s Disease 10
Alzheimer’s Disease: Targeting Neuroinflammation 11 • Chronic neuroinflammation a hallmark of dysregulated microglia, cause of nerve cell death • Systemic inflammation likely contributes to disease progression • MSCs in animal models of Alzheimer’s: – Cross the blood brain barrier (BBB) – ↓ pro - inflammatory; ↑ anti - inflammatory biomarkers – Improve immune functioning – Promote neurogenesis – Improve endothelial function Pro - inflammatory state appears requisite for disease, neurodegeneration and neuronal death: Lue et al Inflammation, A beta deposition, and neurofibrillary tangle formation as correlates of Alzheimer's disease neurodegeneration. J Neuropathol Exp Neurol. 1996;55(10):1083 - 8. Epub 1996/10/01 Pimplikar. Neuroinflammation in Alzheimer's disease: from pathogenesis to a therapeutic target. J Clin Immunol. 2014;34 Suppl 1:S64 - 9. Epub 2014/04/09. doi: 10.1007/s10875 - 014 - 0032 - 5. Heneka et al. Neuroinflammation in Alzheimer's disease. Lancet Neurol. 2015;14(4):388 - 405. Epub 2015/03/21. doi: 10.1016/S1474 - 4422(15)70016 - 5. Neves et al. Intravenous administration of mesenchymal stem cells reduces Tau phosphorylation and inflammation in the 3xTg - AD mouse model of Alzheimer's disease. Experimental neurology. Kim et al. The preventive and therapeutic effects of intravenous human adipose - derived stem cells in Alzheimer's disease mice. PloS one. 2012;7(9):e45757. Shin et al. Mesenchymal stem cells enhance autophagy and increase beta - amyloid clearance in Alzheimer disease models. Autophagy. 2014;10(1):32 - 44. Lee JK. Soluble CCL5 derived from bone marrow - derived mesenchymal stem cells and activated by amyloid beta ameliorates Alzheimer's disease in mice by recruiting bone marrow - induced microglia immune responses. Stem Cells. 2012;30(7):1544 - 55. Bae et al. Bone marrow - derived mesenchymal stem cells contribute to the reduction of amyloid - beta deposits and the improvement of synaptic transmission in a mouse model of pre - dementia Alzheimer's disease. Curr Alzheimer Res. 2013;10(5):524 - 31.
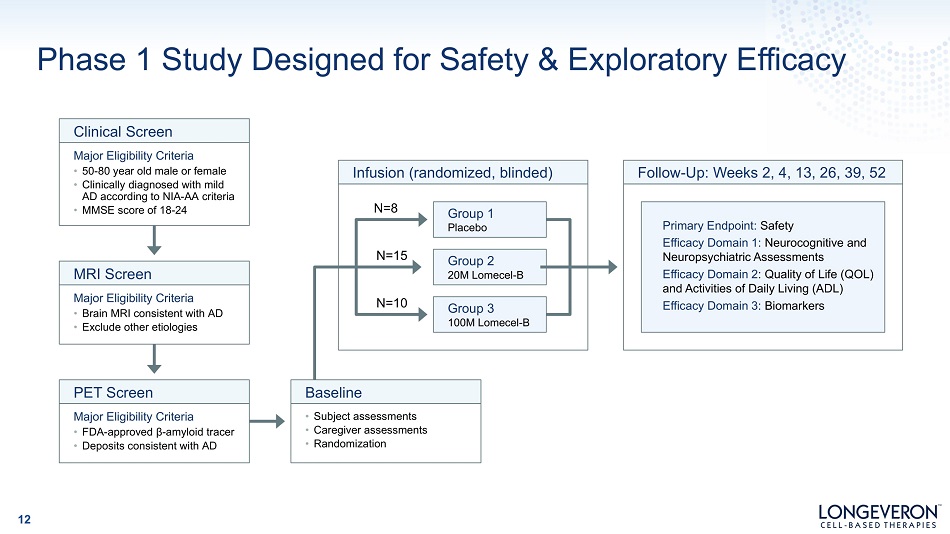
Phase 1 Study Designed for Safety & Exploratory Efficacy 12 Group 1 Placebo Group 2 20M Lomecel - B Group 3 100M Lomecel - B Infusion (randomized, blinded) Clinical Screen Major Eligibility Criteria • 50 - 80 year old male or female • Clinically diagnosed with mild AD according to NIA - AA criteria • MMSE score of 18 - 24 MRI Screen Major Eligibility Criteria • Brain MRI consistent with AD • Exclude other etiologies Major Eligibility Criteria • FDA - approved β - amyloid tracer • Deposits consistent with AD PET Screen • Subject assessments • Caregiver assessments • Randomization Baseline Primary Endpoint: Safety Efficacy Domain 1: Neurocognitive and Neu r ops yc h i a tr i c A ss es sm en ts Efficacy Domain 2 : Quality of Life (QOL) and Activities of Daily Living (ADL) Efficacy Domain 3: Biomarkers Follow - Up: Weeks 2, 4, 13, 26, 39, 52 N=8 N=15 N=10
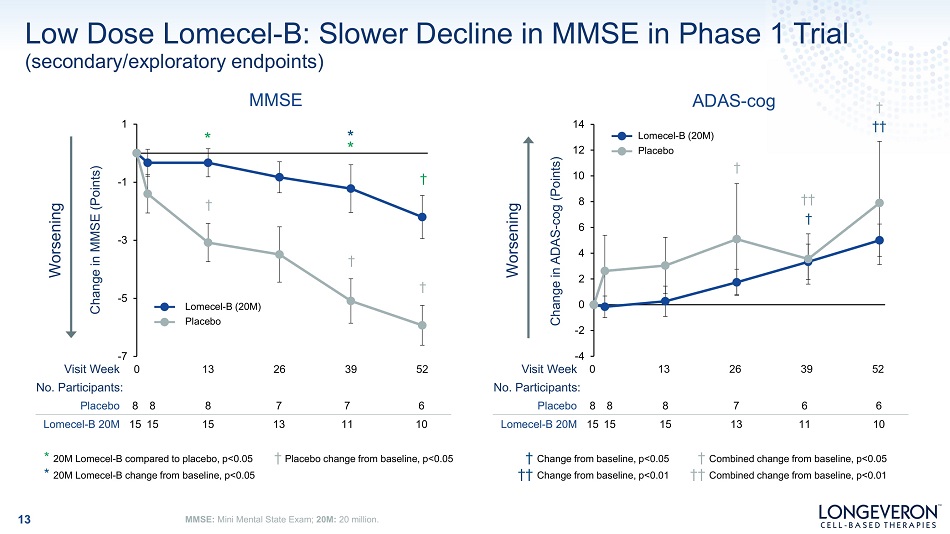
Low Dose Lomecel - B: Slower Decline in MMSE in Phase 1 Trial 13 MMSE: Mini Mental State Exam; 20M: 20 million. † Pl ac eb o ch ang e f rom ba s e li ne , p<0 . 05 * 20M Lomecel - B compared to placebo, p<0.05 * 20M Lomecel - B change from baseline, p<0.05 † Change from baseline, p<0.05 †† Change from baseline, p<0.01 - 4 - 2 0 2 4 6 8 10 12 14 13 26 39 52 Change in ADAS - cog (Points) ADAS - cog † †† † † †† Worsening Lo m e c e l - B (20 M ) Placebo V isi t W ee k 0 No. Participants: Placebo 8 8 8 7 6 6 Lomecel - B 20M 15 15 15 13 11 10 Worsening Placebo 8 8 8 7 7 6 Lomecel - B 20M 15 15 15 13 11 10 † Combined change from baseline, p<0.05 †† Combined change from baseline, p<0.01 - 5 - 3 - 1 1 - 7 V isi t W ee k 0 No. Participants: (secondary/exploratory endpoints) MMSE 13 26 39 52 Change in MMSE (Points) * * * † † Lo m e c e l - B (20 M ) Placebo † †
Safety: Primary Endpoint Met Single infusion of two different doses well tolerated: No Amyloid Related Imaging Abnormalities (ARIA) identified Secondary/Exploratory Endpoints Low dose Lomecel - B group’s MMSE score declined more slowly than placebo Low dose Lomecel - B group showed positive change QOL - AD & ADCS - ADL at 6 months Positive changes in provascular biomarkers (VEGF, IL4 and IL6) Positive changes in inflammatory - associated cytokines (sIL - 2Rα, IL - 10, IL - 12) Observations and results from Phase 1 AD Trial 14
Lomecel - B Robust Clinical Program Aging Frailty 15
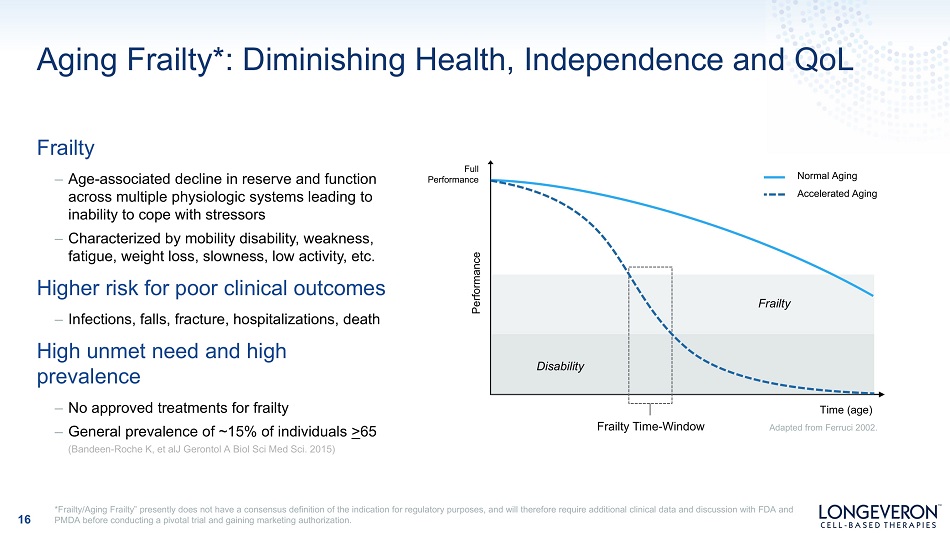
Aging Frailty*: Diminishing Health, Independence and QoL Frailty – Age - associated decline in reserve and function across multiple physiologic systems leading to inability to cope with stressors – Characterized by mobility disability, weakness, fatigue, weight loss, slowness, low activity, etc . Higher risk for poor clinical outcomes – Infections, falls, fracture, hospitalizations, death High unmet need and high prevalence – No approved treatments for frailty – General prevalence of ~15% of individuals > 65 (Bandeen - Roche K, et alJ Gerontol A Biol Sci Med Sci. 2015) Performance Normal Aging A cce l e r ate d A g i ng F r ail ty Disability Time (age) Adapted from Ferruci 2002. Frailty Time - Window *Frailty/Aging Frailty” presently does not have a consensus definition of the indication for regulatory purposes, and will therefore require additional clinical data and discussion with FDA and PMDA before conducting a pivotal trial and gaining marketing authorization. 16 F ul l P e rf o rm an ce
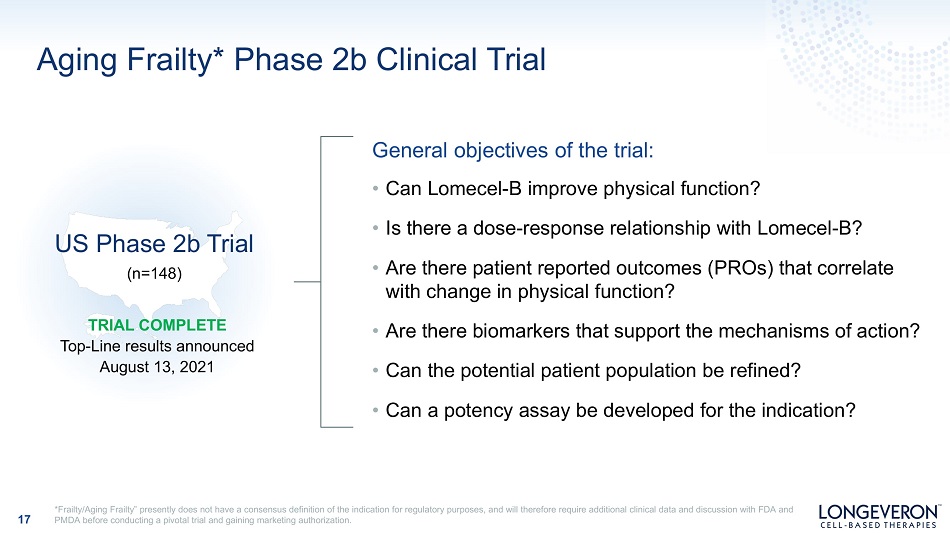
Aging Frailty* Phase 2b Clinical Trial General objectives of the trial: • Can Lomecel - B improve physical function? • Is there a dose - response relationship with Lomecel - B? • Are there patient reported outcomes (PROs) that correlate with change in physical function? • Are there biomarkers that support the mechanisms of action? • Can the potential patient population be refined? • Can a potency assay be developed for the indication? TRIAL COMPLETE Top - Line results announced August 13, 2021 US Phase 2b Trial (n=148) *Frailty/Aging Frailty” presently does not have a consensus definition of the indication for regulatory purposes, and will therefore require additional clinical data and discussion with FDA and PMDA before conducting a pivotal trial and gaining marketing authorization. 17
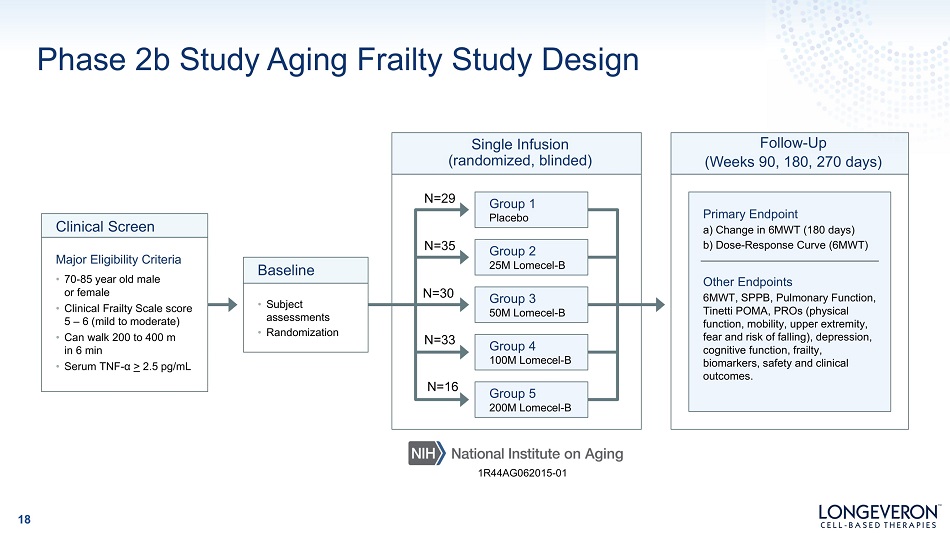
Phase 2b Study Aging Frailty Study Design Group 1 Placebo Group 2 25M Lomecel - B Group 3 50M Lomecel - B Single Infusion (randomized, blinded) Clinical Screen Major Eligibility Criteria • 70 - 85 year old male or female • Clinical Frailty Scale score 5 – 6 (mild to moderate) • Can walk 200 to 400 m in 6 min • Serum TNF - α > 2.5 pg/mL • Subject assess m ents • Randomization Baseline Primary Endpoint a) Change in 6MWT (180 days) b) Dose - Response Curve (6MWT) Other Endpoints 6MWT, SPPB, Pulmonary Function, Tinetti POMA, PROs (physical function, mobility, upper extremity, fear and risk of falling), depression, cognitive function, frailty, biomarkers, safety and clinical outcomes. Follow - Up (Weeks 90, 180, 270 days) N=29 N=35 N=30 Group 4 100M Lomecel - B Group 5 200M Lomecel - B N=33 N=16 1R44AG062015 - 01 18
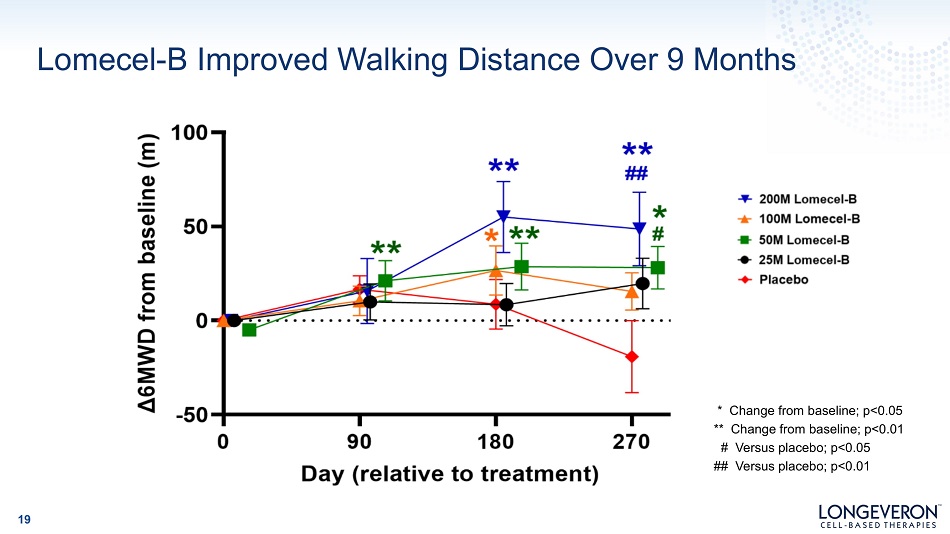
Lomecel - B Improved Walking Distance Over 9 Months * Change from baseline; p<0.05 ** Change from baseline; p<0.01 # Versus placebo; p<0.05 ## Versus placebo; p<0.01 19
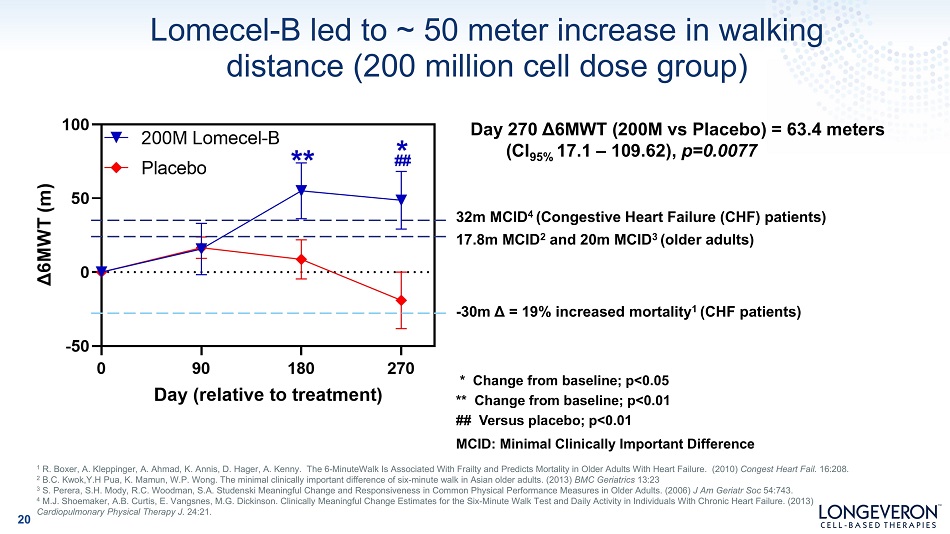
Lomecel - B led to ~ 50 meter increase in walking distance (200 million cell dose group) - 30m Δ = 19% increased mortality 1 (CHF patients) Day 270 Δ6MWT (200M vs Placebo) = 63.4 meters (CI 95% 17.1 – 109.62), p=0.0077 32m MCID 4 (Congestive Heart Failure (CHF) patients) 17.8m MCID 2 and 20m MCID 3 (older adults) * Change from baseline; p<0.05 ** Change from baseline; p<0.01 ## Versus placebo; p<0.01 MCID: Minimal Clinically Important Difference 1 R. Boxer, A. Kleppinger, A. Ahmad, K. Annis, D. Hager, A. Kenny. The 6 - MinuteWalk Is Associated With Frailty and Predicts Mortality in Older Adults With Heart Failure. (2010) Congest Heart Fail. 16:208. 2 B.C. Kwok,Y.H Pua, K. Mamun, W.P. Wong. The minimal clinically important difference of six - minute walk in Asian older adults. (2013) BMC Geriatrics 13:23 3 S. Perera, S.H. Mody, R.C. Woodman, S.A. Studenski Meaningful Change and Responsiveness in Common Physical Performance Measures in Older Adults. (2006) J Am Geriatr Soc 54:743. 4 M.J. Shoemaker, A.B. Curtis, E. Vangsnes, M.G. Dickinson. Clinically Meaningful Change Estimates for the Six - Minute Walk Test and Daily Activity in Individuals With Chronic Heart Failure. (2013) Cardiopulmonary Physical Therapy J. 24:21. 20
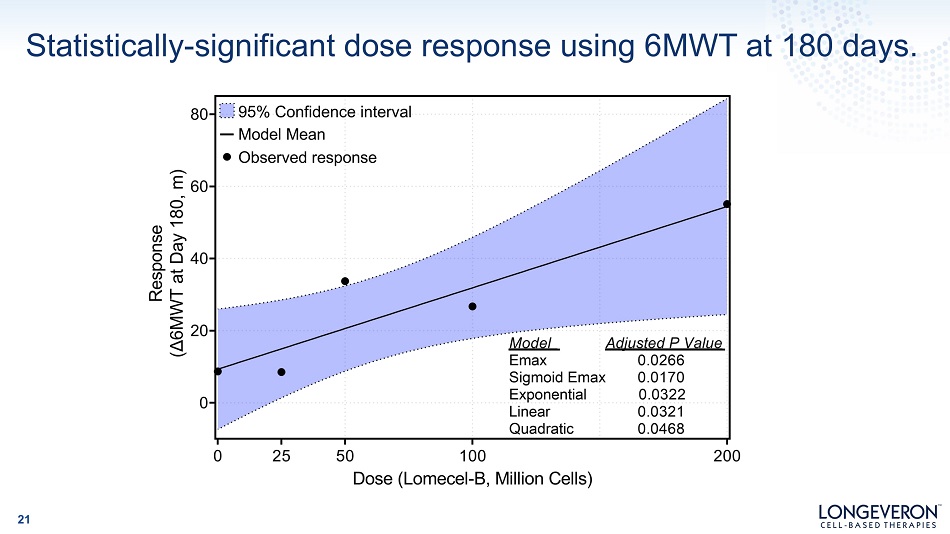
Statistically - significant dose response using 6MWT at 180 days. 21
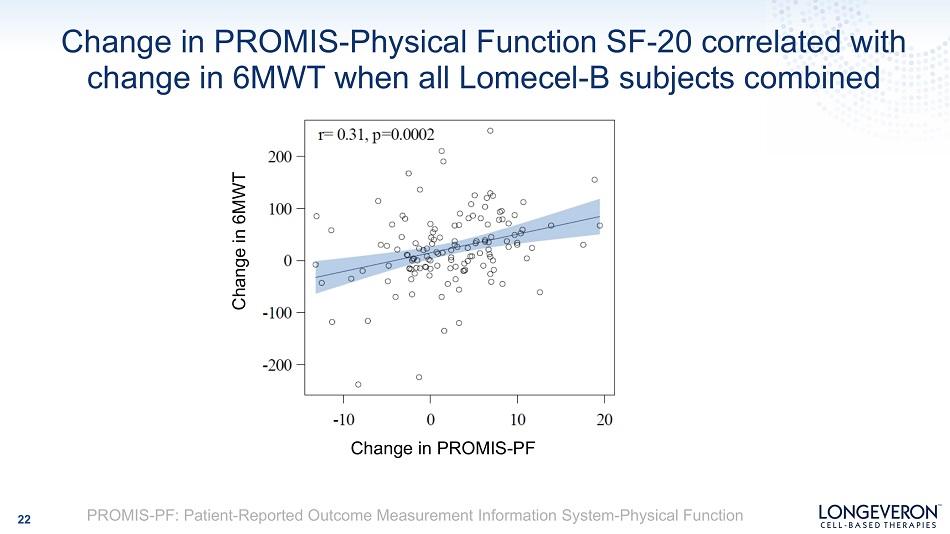
Change in PROMIS - Physical Function SF - 20 correlated with change in 6MWT when all Lomecel - B subjects combined 22 Change in PROMIS - PF Change in 6MWT PROMIS - PF: Patient - Reported Outcome Measurement Information System - Physical Function
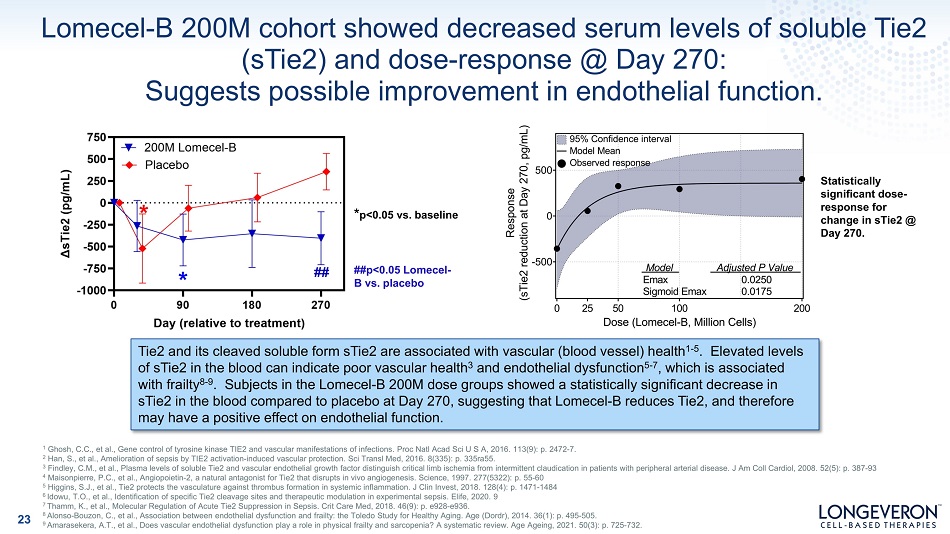
Lomecel - B 200M cohort showed decreased serum levels of soluble Tie2 (sTie2) and dose - response @ Day 270: Suggests possible improvement in endothelial function. ##p<0.05 Lomecel - B vs. placebo * p<0.05 vs. baseline Statistically significant dose - response for change in sTie2 @ Day 270. Tie2 and its cleaved soluble form sTie2 are associated with vascular (blood vessel) health 1 - 5 . Elevated levels of sTie2 in the blood can indicate poor vascular health 3 and endothelial dysfunction 5 - 7 , which is associated with frailty 8 - 9 . Subjects in the Lomecel - B 200M dose groups showed a statistically significant decrease in sTie2 in the blood compared to placebo at Day 270, suggesting that Lomecel - B reduces Tie2, and therefore may have a positive effect on endothelial function. 23 1 Ghosh, C.C., et al., Gene control of tyrosine kinase TIE2 and vascular manifestations of infections. Proc Natl Acad Sci U S A, 2016. 113(9): p. 2472 - 7. 2 Han, S., et al., Amelioration of sepsis by TIE2 activation - induced vascular protection. Sci Transl Med, 2016. 8(335): p. 335ra55. 3 Findley, C.M., et al., Plasma levels of soluble Tie2 and vascular endothelial growth factor distinguish critical limb ischemia from intermittent claudication in patients with peripheral arterial disease. J Am Coll Cardiol, 2008. 52(5): p. 387 - 93 4 Maisonpierre, P.C., et al., Angiopoietin - 2, a natural antagonist for Tie2 that disrupts in vivo angiogenesis. Science, 1997. 277(5322): p. 55 - 60 5 Higgins, S.J., et al., Tie2 protects the vasculature against thrombus formation in systemic inflammation. J Clin Invest, 2018. 128(4): p. 1471 - 1484 6 Idowu, T.O., et al., Identification of specific Tie2 cleavage sites and therapeutic modulation in experimental sepsis. Elife, 2020. 9 7 Thamm, K., et al., Molecular Regulation of Acute Tie2 Suppression in Sepsis. Crit Care Med, 2018. 46(9): p. e928 - e936. 8 Alonso - Bouzon, C., et al., Association between endothelial dysfunction and frailty: the Toledo Study for Healthy Aging. Age (Dordr), 2014. 36(1): p. 495 - 505. 9 Amarasekera, A.T., et al., Does vascular endothelial dysfunction play a role in physical frailty and sarcopenia? A systematic review. Age Ageing, 2021. 50(3): p. 725 - 732.
Anticipated Next Steps 24 • Continued deeper review of clinical data, subgroup analysis, biomarker analysis; • Work with Longeveron’s Frailty Steering Committee & potentially regulators to determine next steps in clinical development plan; • Publish results in peer - reviewed journal
“HERA” Trial: Immune Response to Influenza Vaccine in Aging Frailty* 25 *As noted previously, Frailty/Aging Frailty” is currently not a recognized indication by US FDA or Japan PMDA HAI=Hemagglutination Inhibition Objectives • Safety • Can Lomecel - B improve adaptive immunity against influenza virus in subjects with Aging Frailty? Exploratory Endpoints (not full list) • Change from baseline in HAI assay at 4 weeks • Virus - specific antibody production • Incidence of flu/flu - like symptoms • Changes in frailty (e.g. physical function & mobility) US Phase 1/2 Influenza Vaccine Trial (n=61) TRIAL COMPLETE Top - line results anticipated in 2021 or early 2022
Aging Frailty* Clinical Trial in Japan 26 Objectives • Safety • Can Lomecel - B improve exercise tolerance and mobility? Efficacy Endpoints • Change in 6MWT; grip strength, walking speed, patient - reported outcomes biomarkers, fear and risk of falling, depression, sexual function, clinical outcomes, others Japanese National Center for Geriatrics and Gerontology - sponsored trial • NCGG (Nagoya) and Juntendo University (Tokyo) selected as clinical sites Clinical Trial Notification (CTN) accepted by PMDA TRIAL PLANNING ONGOING Anticipated to start in 2021 or early 2022 Japan Phase 2 Trial (n=45) *Frailty/Aging Frailty” presently does not have a consensus definition of the indication for regulatory purposes, and will therefore require additional clinical data and discussion with FDA and PMDA before conducting a pivotal trial and gaining marketing authorization.
Lomecel - B Robust Clinical Program Congenital Heart Defect 27
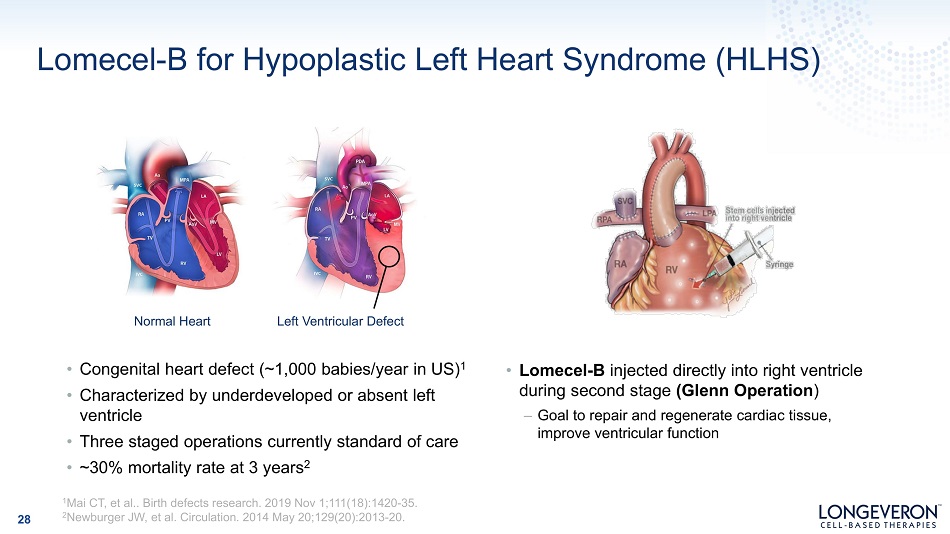
Lomecel - B for Hypoplastic Left Heart Syndrome (HLHS) Normal Heart Left Ventricular Defect • Congenital heart defect (~1,000 babies/year in US) 1 • Characterized by underdeveloped or absent left ventricle • Three staged operations currently standard of care • ~30% mortality rate at 3 years 2 • Lomecel - B injected directly into right ventricle during second stage (Glenn Operation ) – Goal to repair and regenerate cardiac tissue, improve ventricular function 28 1 Mai CT, et al.. Birth defects research. 2019 Nov 1;111(18):1420 - 35. 2 Newburger JW, et al. Circulation. 2014 May 20;129(20):2013 - 20.
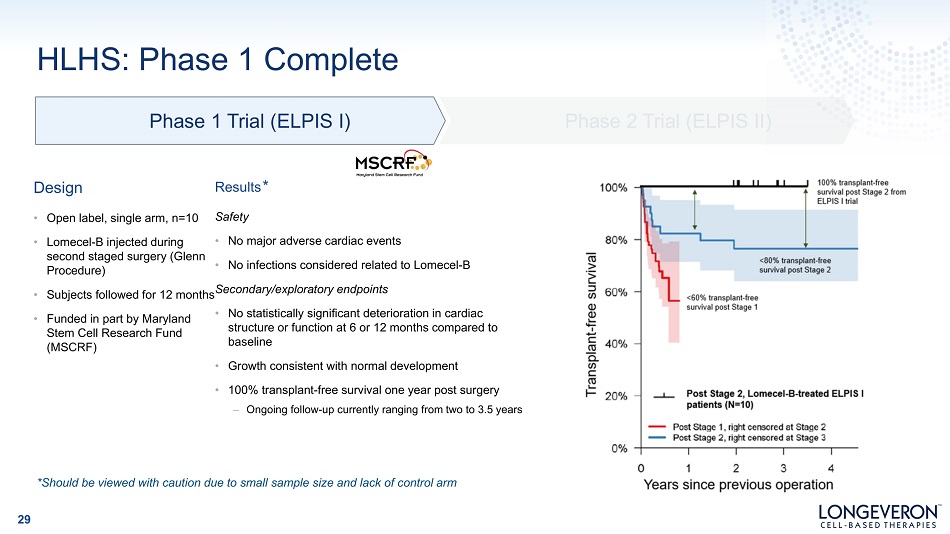
Phase 1 Trial (ELPIS I) HLHS: Phase 1 Complete D e s ign • Open label, single arm, n=10 • Lomecel - B injected during second staged surgery (Glenn Procedure) • • Funded in part by Maryland Stem Cell Research Fund (MSCRF) Subjects followed for 12 months Secondary/exploratory endpoints Results * Safety • No major adverse cardiac events • No infections considered related to Lomecel - B • No statistically significant deterioration in cardiac structure or function at 6 or 12 months compared to baseline • Growth consistent with normal development • 100% transplant - free survival one year post surgery – Ongoing follow - up currently ranging from two to 3.5 years Phase 2 Trial (ELPIS II) *Should be viewed with caution due to small sample size and lack of control arm 29
HLHS: On to Phase 2 • N=38; randomized, controlled, blinded • First infant treated July 7 2021 during Stage II Glenn surgery • Will be enrolling at up to seven major pediatric cardiac centers • Primary endpoint: Change in Right Ventricular Ejection Fraction (RVEF) at 12 months Phase 1 Trial (ELPIS I) Phase 2 Trial (ELPIS II) 30
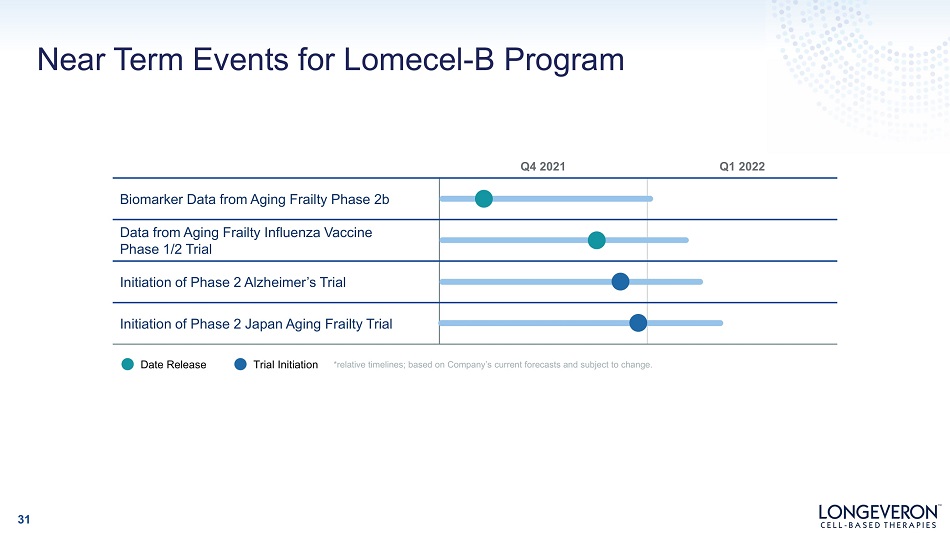
Q4 2021 Q1 2022 Biomarker Data from Aging Frailty Phase 2b Data from Aging Frailty Influenza Vaccine Phase 1/2 Trial Initiation of Phase 2 Alzheimer’s Trial Initiation of Phase 2 Japan Aging Frailty Trial Near Term Events for Lomecel - B Program *relative timelines; based on Company’s current forecasts and subject to change. Date Release Trial Initiation 31

Corporate Overview 32
Intellectual Property & Barriers to Competition 33 Company - Owned Patent Applications • Allogeneic MSCs for use as a vaccine adjuvant • Allogeneic MSCs for improving humoral immunity • Allogeneic MSCs to treat sexual dysfunction • MSC protein expression from stimuli (potency assay) • MSCs to treat Alzheimer’s disease • Other applications currently confidential Licensed Patents & Applications • Monitoring cardiomyopathy therapy • CD271+ MSCs for cardiac repair – License is for use of CD271+ cells for aging - related disorders Proprietary Manufacturing Process • Exclusively licensed from University of Miami • Improved and optimized by Longeveron • In - house manufacturing to maintain proprietary trade secrets Trademarks and Trademark Applications • Applications pending in multiple jurisdictions for LONGEVERON and LOMECEL - B

Experienced and Successful Leadership Geoff Green, MBA CEO 25+ years in life sciences, with a variety leadership roles throughout his time in the industry, including operations, business development, clinical affairs. Previously President and Acting CEO of DOR BioPharma, (now Soligenix (NAS: SNGX)), VP of Business Dev. & Clinical Affairs at Accu - Break Pharmaceuticals, VP of Operations at Partikula. Earned a B.A. in biology from Kenyon College, and an M.B.A. from Barry University’s Andreas School of Business. Joshua M. Hare, MD Co - Founder & CSO Co - founded Longeveron in 2014 from the University of Miami, where he is also the Founding Director of the university’s Interdisciplinary Stem Cell Institute (ISCI). Graduate of the University of Pennsylvania & Johns Hopkins University School of Medicine. Served as a research fellow at Harvard University and is Board Certified in cardiovascular medicine. James Clavijo CFO 25+ years of experience as a CFO for pharmaceutical, healthcare and manufacturing companies. Served as Chief Financial Officer for Aeterna Zentaris (NASDAQ:AEZS) & Tri - source Pharma & as Chief Accounting Officer at Soligenix (NASDAQ: SNGX) Dan Gincel, PhD Senior VP, Strategic Collaborations & Scientific Affairs 20+ years leadership experience overseeing development and commercialization of regenerative medicines, including cell therapies, as well as establishing public - private collaborations and corporate partnerships. VP of University Partnerships and a member of the Executive Leadership team at the Maryland Technology Development Corporation (TEDCO). Lisa McClain - Moss Vice President, Manufacturing With leadership with Cognate BioServices and St. Jude’s Children Research Hospital, Ms. McClain - Moss leads Longeveron’s cell therapy manufacturing and product development activity. Paul Lehr, JD General Counsel, International Executive Director 25+ years with legal & executive positions in corporate and research settings. Former President of the Pritikin Longevity Institute and CEO of National YoungArts Foundation.. BA from Brown University, and JD from University of Florida. Anthony Oliva, PhD Senior Scientist 20+ years of basic and clinical research experience, with accumulated experience in regulatory and clinical affairs. Integral in leading Longeveron’s grant application and grant funding process. B.A. in Biological Sciences from the University of Chicago; Ph.D. in Neuroscience from Baylor College of Medicine; Post - doctoral research at Oregon Health & Science University. 34
S um m ary Well - characterized allogeneic MSC product in development Robust clinical pipeline with advanced trials in Alzheimer’s disease, aging related frailty, HLHS and other indications State - of - the - art GMP facility for stringent manufacturing Lomecel - B well - tolerated to date; supportive early clinical data in 3 indications Significant catalysts expected in 2021 - 2022 Proven management, scientific, and manufacturing teams 35

Thank You 36 www.longeveron.com Nasdaq: LGVN
