false
0001094038
0001094038
2025-08-26
2025-08-26
iso4217:USD
xbrli:shares
iso4217:USD
xbrli:shares
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d) of the Securities
Exchange Act of 1934
August 26, 2025
Date of Report (Date of earliest event reported)
MARKER THERAPEUTICS, INC.
(Exact name of registrant as specified in its charter)
| Delaware |
001-37939 |
45-4497941 |
(State or other jurisdiction of
incorporation) |
(Commission File Number) |
(IRS Employer Identification No.) |
|
2450 Holcombe Blvd, TMC Partners Office 1.311
Houston,
Texas |
|
77021 |
| (Address of principal executive offices) |
|
(Zip Code) |
(713) 400-6400
Registrant’s telephone number, including
area code
(Former name or former address, if changed since
last report)
Check the appropriate box below if the Form 8-K is intended to simultaneously
satisfy the filing obligation of the registrant under any of the following provisions:
| ¨ |
Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| ¨ |
Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
| ¨ |
Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| ¨ |
Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class |
|
Trading
Symbol(s) |
|
Name of each exchange on which
registered |
| Common Stock, par value $0.001 per share |
|
MRKR |
|
The Nasdaq Stock Market LLC |
Indicate by check mark whether the registrant is an emerging growth
company as defined in Rule 405 of the Securities Act of 1933 (§230.405 of this chapter) or Rule 12b-2 of the Securities
Exchange Act of 1934 (§240.12b-2 of this chapter).
Emerging
growth company ¨
If an emerging
growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any
new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ¨
Item 7.01. Regulation
FD Disclosure.
On August 26, 2025, Marker Therapeutics, Inc. (the
“Company”) issued a press release announcing the progress and clinical observations from the Company’s Phase
1 APOLLO study. A copy of the press release is attached hereto as Exhibit 99.1 to this Current Report on Form 8-K and is incorporated
herein by reference.
In addition, on August 26, 2025, the Company updated
its corporate presentation, which is available through the Company’s website and a copy of which is attached hereto as Exhibit 99.2
to this Current Report on Form 8-K. The Company will also host a webcast discussing the results from the Company’s APOLLO study.
The webcast presentation is attached hereto as Exhibit 99.3.
The
information in this Item 7.01 of this Current Report on Form 8-K (including Exhibit 99.1, 99.2 and 99.3) is being furnished
and shall not be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended (the “Exchange
Act”), or subject to the liabilities of that section or Sections 11 and 12(a)(2) of the
Securities Act of 1933, as amended. The information shall not be deemed incorporated by reference into any filing under the Securities
Act of 1933, as amended, or the Exchange Act, except as expressly set forth by specific reference in such a filing.
Item 9.01. Financial Statements and Exhibits.
(d) Exhibits.
SIGNATURES
Pursuant to the requirements
of the Securities Exchange Act of 1934, as amended, the Registrant has duly caused this report to be signed on its behalf by the undersigned
hereunto duly authorized.
| |
Marker Therapeutics, Inc. |
| |
|
|
| Dated: August 26, 2025 |
By: |
/s/ Juan Vera |
| |
|
Juan Vera |
| |
|
President and Chief Executive Officer |
Exhibit 99.1

Marker Therapeutics Provides Update on Phase
1 APOLLO Study Highlighting Encouraging Overall Response Rates in Relapsed Lymphoma
Ongoing Phase 1 APOLLO study investigating MT-601
in patients with relapsed B cell lymphoma showed 66% of Non-Hodgkin Lymphoma (NHL) patients achieving objective response rates, with 50%
demonstrating complete response (CR)
Favorable safety profile observed in study participants
with no dose limiting toxicities (DLTs) or immune-effector cell associated neurotoxicity syndrome (ICANS) in the dose escalation cohort
Dose expansion phase of study will investigate
MT-601 at pre-specified maximum dose in patients with Diffuse Large B Cell Lymphoma (DLBCL) who have relapsed after or are ineligible
for chimeric antigen receptor (CAR)-T cell therapy
Live Webcast to be held today to discuss results
at 8:30 a.m. ET
Houston, TX – August 26, 2025 –
Marker Therapeutics, Inc. (Nasdaq: MRKR), a clinical-stage immuno-oncology company focusing on developing next-generation T cell-based
immunotherapies for the treatment of hematological malignancies and solid tumor indications, today provided an update on the progress
and clinical observations from the Phase 1 APOLLO study.
The Company’s Phase 1 APOLLO study (clinicaltrials.gov
identifier: NCT05798897) is a multicenter, open-label clinical study investigating MT-601, a Multi-Antigen Recognizing (MAR)-T cell product,
in patients with lymphoma who have relapsed after anti-CD19 CAR-T cell therapy or for whom anti-CD19 CAR-T cell therapy is not an option.
Today, Marker is reporting an update on the safety and efficacy data from the dose escalation portion of the study showing a favorable
safety profile across all evaluated doses (dose range 100x106-400x106 cells) and a 66% objective response rate in
patients with NHL, with 50% demonstrating complete response.
A total of 24 B-cell lymphoma patients have been
treated with MT-601 across 7 U.S. clinical sites, including 15 patients with Non-Hodgkin Lymphoma (NHL) and 9 patients with Hodgkin Lymphoma
(HL). At the time of the data cutoff (June 2025), 12 NHL and 9 HL patients have been assessed. Patients with NHL and HL received doses
ranging from 100x106-400x106 cells and showed objective responses and a favorable safety profile.
“We are very excited and encouraged by the
progress of the study,” said Juan Vera, M.D., President and CEO of Marker Therapeutics. “The safety and preliminary efficacy
data from our Phase 1 APOLLO study underscore the potential of MT-601 in heavily pre-treated patients with lymphoma, who have relapsed
after multiple lines of therapy, including CAR-T cells and bispecific antibodies. While CAR-T cells have gained acceptance in the treatment
of lymphoma, with approximately 8,000 patients treated globally in 2024, 40-60% of such patients have disease progression within the first
year of treatment. We believe that MT-601 could address this critical unmet need and offer new hope to patients who have exhausted multiple
lines of treatment, including CAR-T cell therapy.”
Efficacy and Duration of Response
The 12 NHL patients received doses ranging from
100x106-200x106 cells and had undergone multiple lines of therapy (median of 5 prior lines of therapy), including
anti-CD19 CAR-T cells (n=9) and bispecific antibodies (n=4); dual exposed patients (n=4). 8 out of 12 NHL patients had objective responses
(66%), with 6 patients demonstrating complete response (CR) as best response (50%). Durable responses were observed (range 3-24 months)
with 5 patients showing continued response ≥6 months, including 3 patients with ≥12 months durability.
HL patients received doses ranging from 200x106-400x106
cells and had undergone a median of 8 prior lines of therapy. Seven out of 9 HL patients had objective responses (78%), with 1 patient
demonstrating CR (11%) highlighting the versatility of MT-601 across multiple histologies.
Safety Profile
The dose escalation portion of the study tested
doses ranging from 100x106-400x106 cells in patients with B-cell lymphoma. To date, no DLTs have been reported at
the highest dose (400x106 cells). Infusion of MT-601 was well tolerated in all study participants, with no observation of ICANS
and two reported Grade 1 cytokine release syndrome (CRS) events (fever; no treatment was required). Patients were treated with or without
lymphodepleting chemotherapy prior to receiving infusions of MT-601. No change in DLTs or ICANS was observed between patients treated
with and without lymphodepletion. Data collected from the 24 patients treated demonstrated a robust safety profile with no reported serious
adverse events reinforcing the benefit of MT-601.
Study Design and Dose Expansion
The Phase 1 APOLLO study is composed of a dose
escalation phase, followed by a dose expansion phase. The dose escalation cohort evaluated the safety and optimum dose level of MT-601
with doses ranging from 100x106-400x106 cells. On June 17, the Safety Review Committee (SRC) cleared the pre-specified
maximum dose (400x106 cells) for the dose expansion portion of the trial. The dose expansion will enroll patients with DLBCL
who have relapsed after anti-CD19 CAR-T cells or who are ineligible for CAR-T therapy.
“The observed outcomes in NHL demonstrate
that certain patients can achieve clinically meaningful responses with MT-601 even at lower doses of 100x106 or 200x106
cells,” commented Dr. Vera. “We look forward to advancing the study to the dose expansion phase, where we will investigate
MT-601 at the maximum dose of 400x106 cells in patients with relapsed DLBCL to potentially build upon these promising results.”
Dr. Vera continued, “The encouraging efficacy
in patients with NHL was achieved at doses ranging from 100x106-200x106 cells. We believe that investigating MT-601
at the maximum dose of 400x106 cells in the dose expansion cohort could have the potential to further improve the clinical
efficacy and durability we are currently observing in patients with NHL. It is particularly encouraging that even at the highest dose
level no DLTs were reported in the dose escalation phase. We will continue to closely monitor the safety and efficacy of MT-601 in treated
patients and anticipate to provide another data update in the first half of 2026.”
Webcast Details
Marker will host a live, online-only webcast
today at 8:30 am E.D.T. to discuss the clinical results and provide a corporate update. To attend the live event, please use this
link to register. During the event, attendees will have the opportunity to submit written questions via the webcast platform’s
Q&A feature. After the event, a recording will be made available for replay on the Company’s IR website under Events &
Presentations for approximately 30 days.
About MT-601
The Company’s lead product, MT-601, is a
multi-antigen recognizing (MAR) T cell product that utilizes a non-genetically modified approach that specifically targets six different
tumor antigens upregulated in lymphoma cells (Survivin, PRAME, WT-1, NY-ESO-1, SSX-2, MAGEA-4). Marker is currently investigating MT-601
in the Company-sponsored Phase 1 APOLLO trial (clinicaltrials.gov identifier: NCT05798897) for the treatment of patients with lymphoma
who have relapsed after or are not candidates for anti-CD19 CAR-T cell therapies.
About APOLLO
The APOLLO trial (clinicaltrials.gov Identifier:
NCT05798897) is a Phase 1, multicenter, open-label study designed to evaluate the safety and efficacy of MT-601 in participants with relapsed
or refractory lymphoma who have either failed anti-CD19 chimeric antigen receptor (CAR) T cell therapy or are not candidates for anti-CD19
CAR-T cell therapy. The primary objective of this exploratory Phase 1 clinical trial is to evaluate the optimum dose, safety, and preliminary
efficacy of MT-601 in participants with various lymphoma subtypes. The APOLLO study is supported by the National Cancer Institute of the
National Institutes of Health under Award Number R44CA291521.
About MAR-T cells
The multi-antigen recognizing (MAR) T cell platform
(formerly known as multiTAA-specific T cells) is a novel, non-genetically modified cell therapy approach that selectively expands tumor-specific
T cells from a patient's/donor’s blood capable of recognizing a broad range of tumor antigens. Unlike other T cell therapies, MAR-T
cells allow the recognition of hundreds of different epitopes within up to six tumor-specific antigens, thereby reducing the possibility
of tumor escape. Since MAR-T cells are not genetically engineered, Marker believes that its product candidates will be easier and less
expensive to manufacture, with an improved safety profile compared to current engineered T cell approaches and may provide patients with
meaningful clinical benefits.
About Marker Therapeutics, Inc.
Marker Therapeutics, Inc. is a Houston, TX-based
clinical-stage immuno-oncology company specializing in the development of next-generation T cell-based immunotherapies for the treatment
of hematological malignancies and solid tumors. The Company was founded at Baylor College of Medicine, and clinical trials that enrolled
more than 200 patients across various hematological and solid tumor indications showed that the Company’s autologous and allogeneic
MAR-T cell products were well tolerated and demonstrated durable clinical responses. Marker’s goal is to introduce novel T cell
therapies to the market and improve patient outcomes. To achieve these objectives, the Company prioritizes the preservation of financial
resources and focuses on operational excellence. Marker’s unique T cell platform is strengthened by non-dilutive funding from U.S.
state and federal agencies supporting cancer research.
To receive future press releases via email, please
visit: https://www.markertherapeutics.com/email-alerts.
Forward-Looking Statements
This release
contains forward-looking statements for purposes of the safe harbor provisions of the Private Securities Litigation Reform Act of 1995.
Statements in this news release concerning the Company’s expectations, plans, business outlook or future performance, and any other
statements concerning assumptions made or expectations as to any future events, conditions, performance or other matters, are “forward-looking
statements.” Forward-looking statements include statements regarding our intentions, beliefs, projections, outlook, analyses or
current expectations concerning, among other things: our research, development and regulatory activities and expectations relating to
our non-engineered multi-tumor antigen specific T cell therapies; the effectiveness of these programs or the possible range of application
and potential curative effects and safety in the treatment of diseases; and the timing, conduct, interim results announcements and outcomes
of our clinical trials of our product candidates, including MT-601 for the treatment of patients with lymphoma.
Forward-looking statements are by their nature subject to risks, uncertainties and other factors which could cause actual results to
differ materially from those stated in such statements. Such risks, uncertainties and factors include, but are not limited to the risks
set forth in the Company’s most recent Form 10-K, 10-Q and other SEC filings
which are available through EDGAR at WWW.SEC.GOV. The Company assumes no obligation
to update its forward-looking statements whether as a result of new information, future events or otherwise, after the date of this press
release except as may be required by law.
Media and Investor Contact
Marker Therapeutics, Inc.
+1 (713) 400-6400
[email protected]
Exhibit 99.2

MARKER THERAPEUTICS CORPORATE PRESENTATION August 2025 NASDAQ: MRKR
Forward Looking Statements Certain statements contained herein are forward - looking statements within the meaning of Section 21 E of the Securities Exchange Act of 1934 , as amended, and Section 27 A of the Securities Act of 1933 , as amended, that involve risks and uncertainties . All statements other than statements relating to historical matters including statements to the effect that we “believe”, “expect”, “anticipate”, “plan”, “target”, “intend” and similar expressions, including without limitation statements regarding Marker Therapeutics, Inc . ’s (“Marker” or the “Company”) intentions, beliefs, projections, outlook, analyses or current expectations are “forward - looking statements” . Forward - looking statements include statements concerning, among other things : the Company’s research, development and regulatory activities and expectations relating to its non - engineered multi - antigen recognizing (MAR) T cell therapies ; the effectiveness of the Company’s programs or the possible range of application and potential curative effects and safety in the treatment of diseases ; the timing, conduct and success of the Company’s clinical trials of its product candidates, including MT - 401 for the treatment of patients with Acute Myeloid Leukemia (“AML”) or Myelodysplastic Syndrome (“MDS”), MT - 401 Off - the - Shelf (“OTS”) for the treatment of patients with AML, and MT - 601 for the treatment of patients with relapsed lymphoma ; the Company’s long - term stability and cash runway ; the Company’s optimized manufacturing process ; and the future development of MAR - T cell therapies (formerly known as multiTAA - specific T cells) . Forward - looking statements are by their nature subject to risks, uncertainties and other factors which could cause actual results to differ materially from those stated in such statements . Such risks, uncertainties and factors include, but are not limited to the risks set forth in the Company’s most recent Forms 10 - K, 10 - Q and other SEC filings which are available through EDGAR at WWW . SEC . GOV . No representation or warranty (expressed or implied) is made as to, and no reliance should be placed on, the fairness, accuracy or completeness of the information contained herein . Accordingly, none of the Company, or any of its principals, partners, subsidiaries or affiliates, or any of such person’s board members, officers or employees accepts any liability whatsoever arising directly or indirectly from the use of this presentation . Certain information set forth herein includes estimates, projections and targets and involves significant elements of subjective judgement and analysis, which may or may not be correct . No representations are made as to the accuracy of such estimates, projections or targets or that all assumptions relating to such estimates, projections or targets have been considered or stated or that such estimates, projections or targets will be realized . This presentation does not purport to contain all of the information that may be required to evaluate the Company and any recipient hereof should conduct its own independent analysis of the Company and the data and information contained herein . Any forward - looking statements are not guarantees of future performance and actual results may differ materially from estimates in the forward - looking statements . Unless otherwise stated, all information in this presentation is as of the date of the cover page of this presentation, and the Company undertakes no obligation to revise these forward - looking statements to reflect events or circumstances that arise after the date hereof . 2
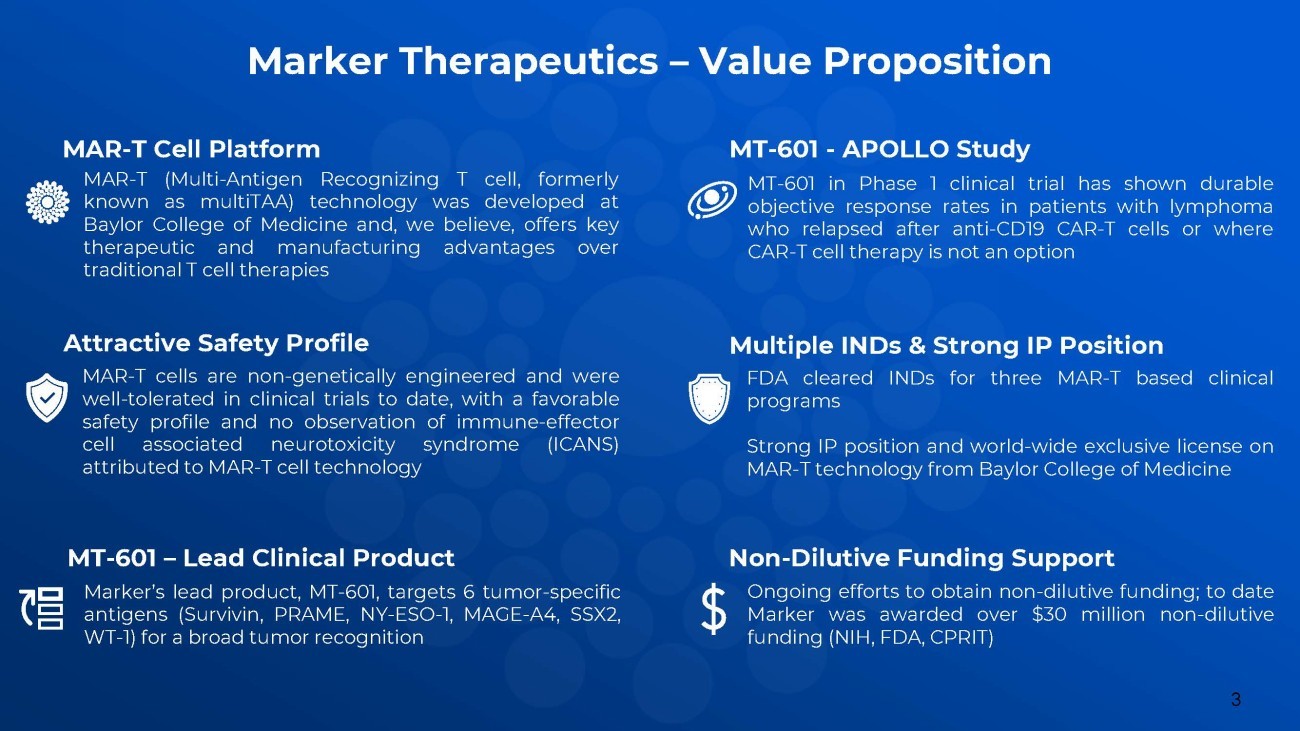
3 MAR - T Cell Platform MAR - T (Multi - Antigen Recognizing T cell, formerly known as multiTAA) technology was developed at Baylor College of Medicine and, we believe, offers key therapeutic and manufacturing advantages over traditional T cell therapies Attractive Safety Profile MAR - T cells are non - genetically engineered and were well - tolerated in clinical trials to date, with a favorable safety profile and no observation of immune - effector cell associated neurotoxicity syndrome (ICANS) attributed to MAR - T cell technology MT - 601 – Lead Clinical Product Marker’s lead product, MT - 601 , targets 6 tumor - specific antigens (Survivin, PRAME, NY - ESO - 1 , MAGE - A 4 , SSX 2 , WT - 1 ) for a broad tumor recognition MT - 601 - APOLLO Study MT - 601 in Phase 1 clinical trial has shown durable objective response rates in patients with lymphoma who relapsed after anti - CD 19 CAR - T cells or where CAR - T cell therapy is not an option Multiple INDs & Strong IP Position FDA cleared INDs for three MAR - T based clinical programs Strong IP position and world - wide exclusive license on MAR - T technology from Baylor College of Medicine Non - Dilutive Funding Support Ongoing efforts to obtain non - dilutive funding ; to date Marker was awarded over $ 30 million non - dilutive funding (NIH, FDA, CPRIT) Marker Therapeutics – Value Proposition

MAR - T Technology 4
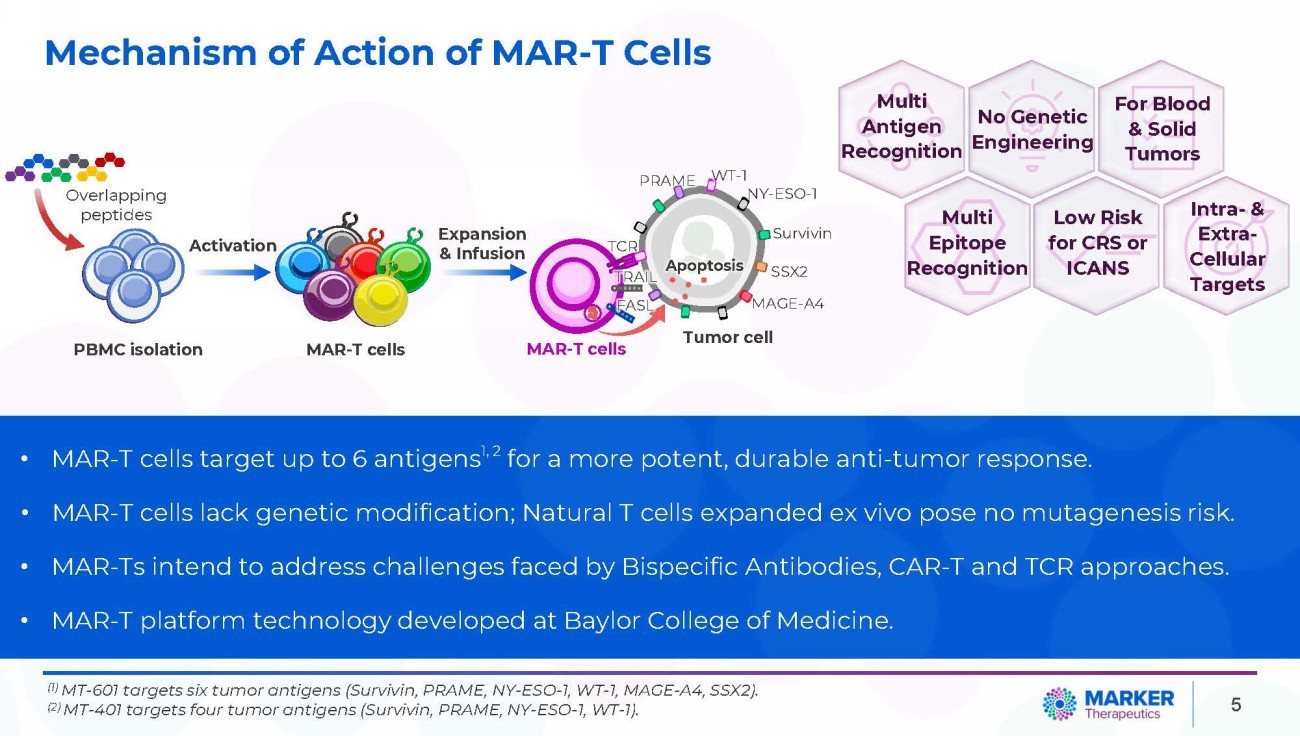
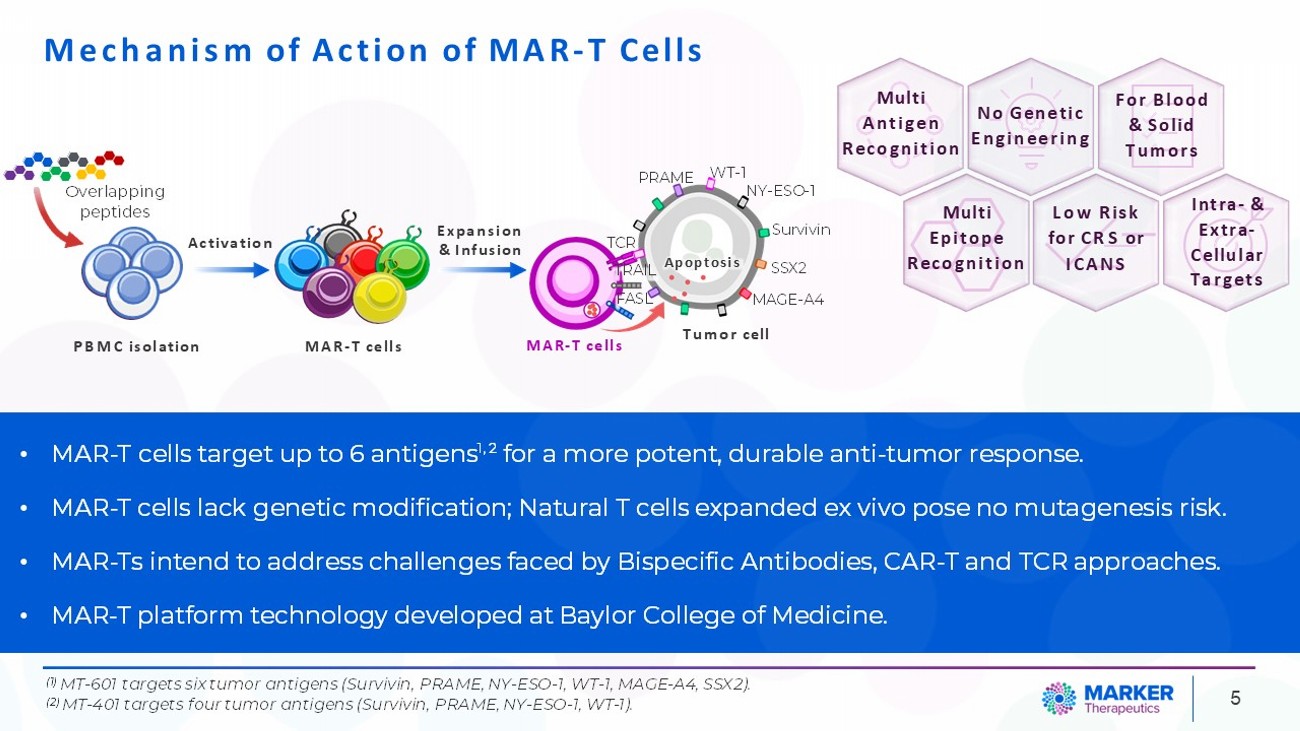
5 • MAR - T cells target up to 6 antigens 1, 2 for a more potent, durable anti - tumor response. • MAR - T cells lack genetic modification; Natural T cells expanded ex vivo pose no mutagenesis risk. • MAR - Ts intend to address challenges faced by Bispecific Antibodies, CAR - T and TCR approaches. • MAR - T platform technology developed at Baylor College of Medicine. Mechanism of Action of MAR - T Cells (1) MT - 601 targets six tumor antigens (Survivin, PRAME, NY - ESO - 1, WT - 1, MAGE - A4, SSX2). (2) MT - 401 targets four tumor antigens (Survivin, PRAME, NY - ESO - 1, WT - 1). Overlapping peptides PBMC isolation MAR - T cells Activation Expansion & Infusion Apoptosis PRAME Survivin WT - 1 NY - ESO - 1 SSX2 MAGE - A4 Tumor cell TCR TRAIL FASL MAR - T cells Multi Antigen Recognition Multi Epitope Recognition Low Risk for CR S o r ICANS For Blood & S ol id Tumors Intra - & Extra - Cellular Targets No Genetic Engineering
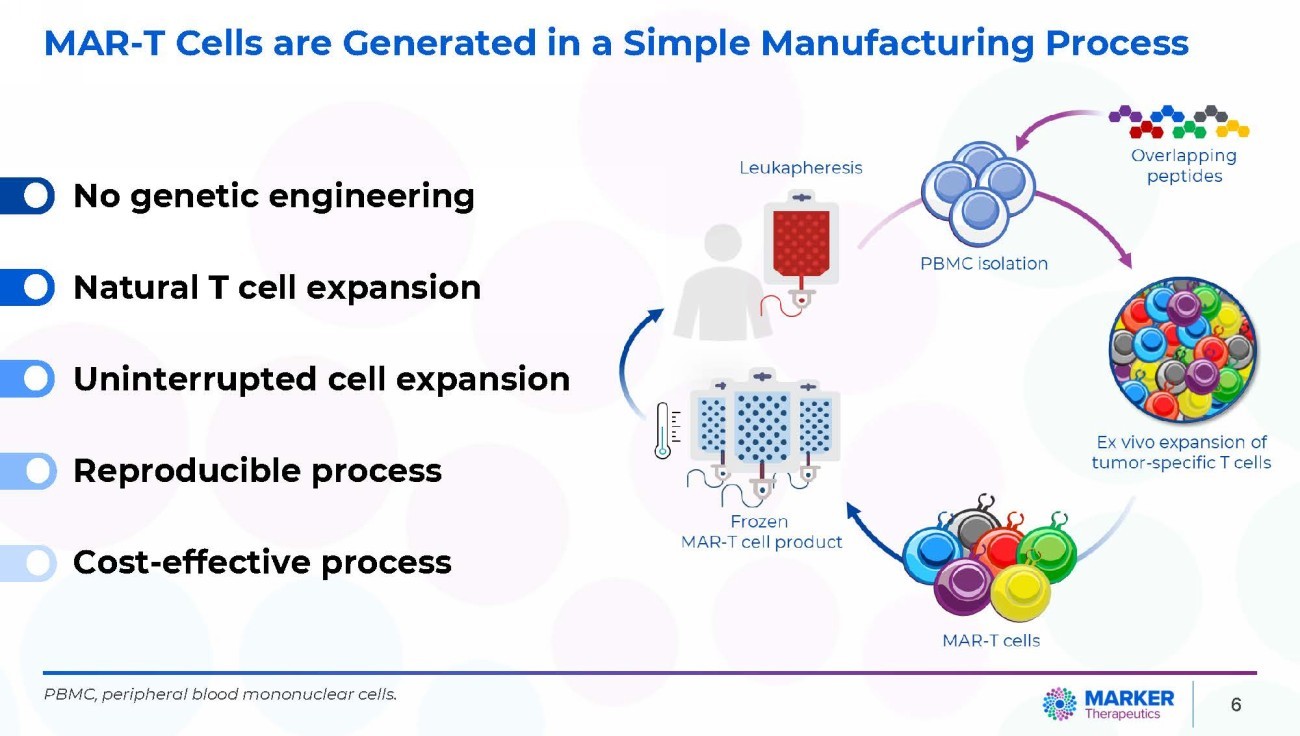
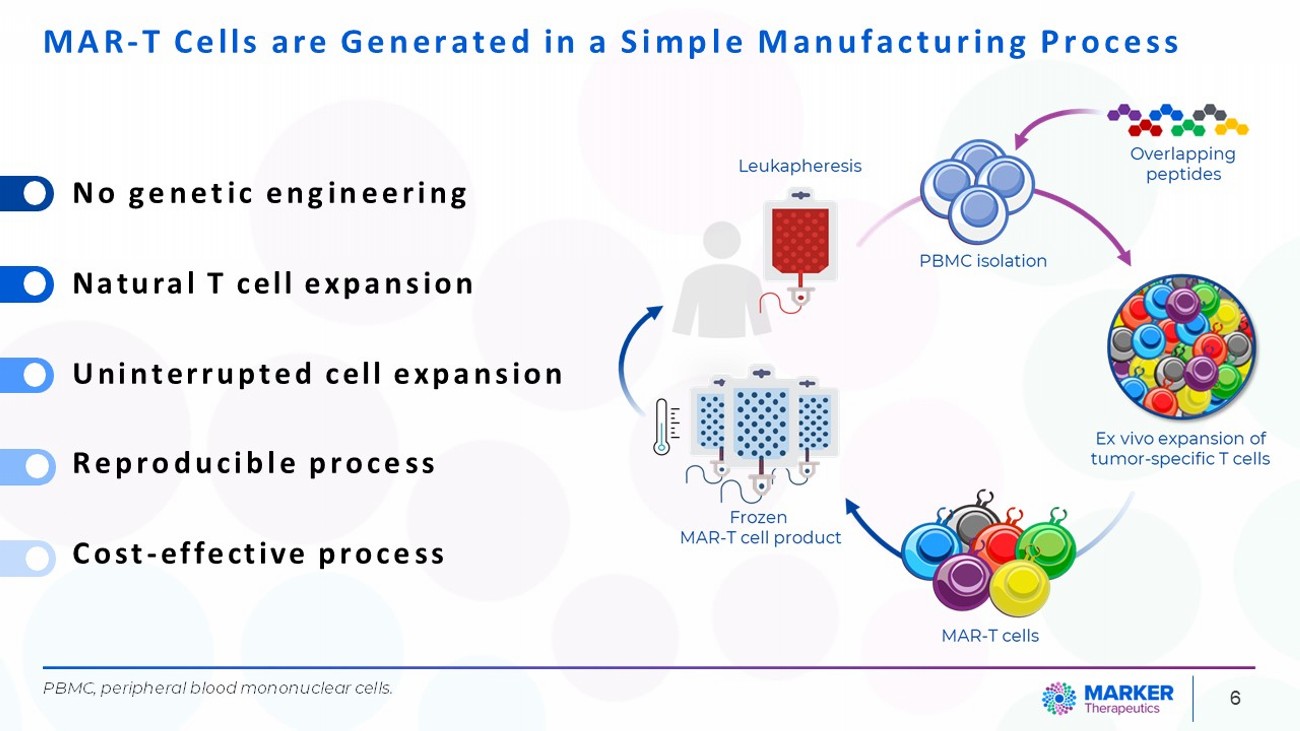
• No genetic engineering • Natural T cell expansion • Uninterrupted cell expansion • Reproducible process • Cost - effective process PBMC, peripheral blood mononuclear cells. 6 MAR - T Cells are Generated in a Simple Manufacturing Process
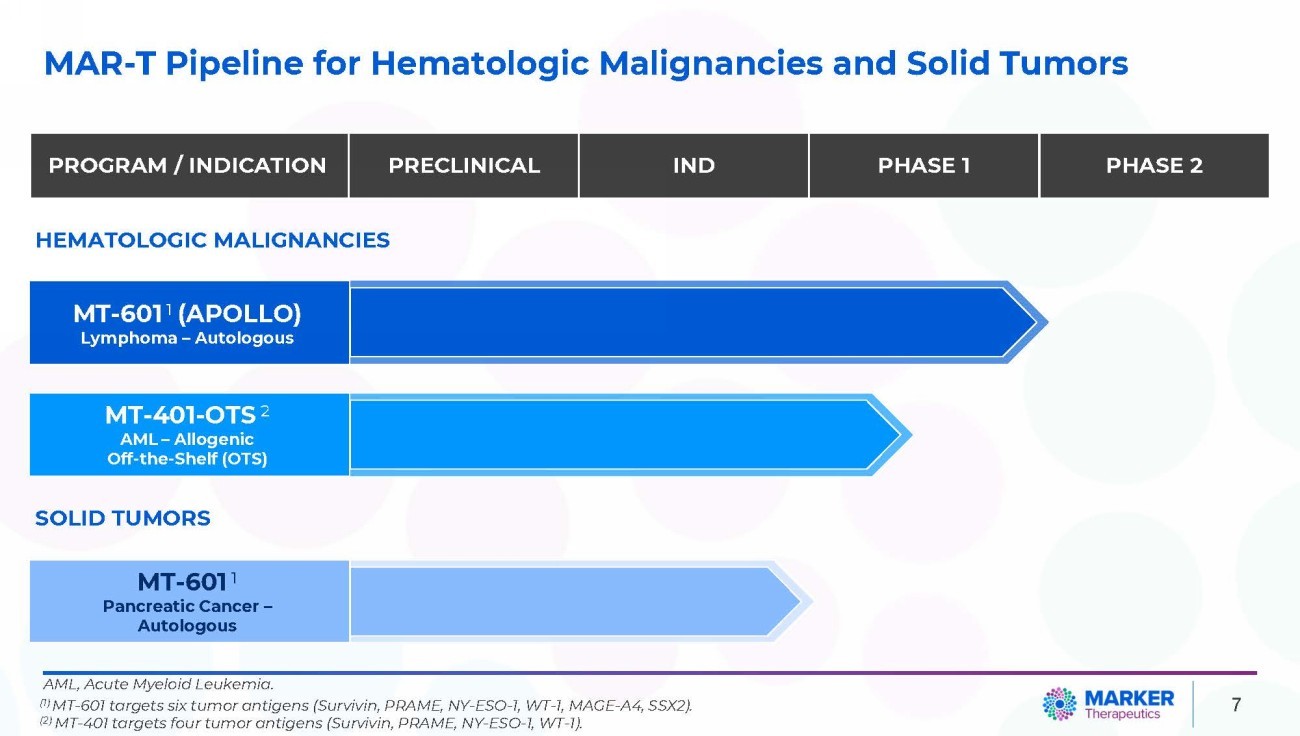
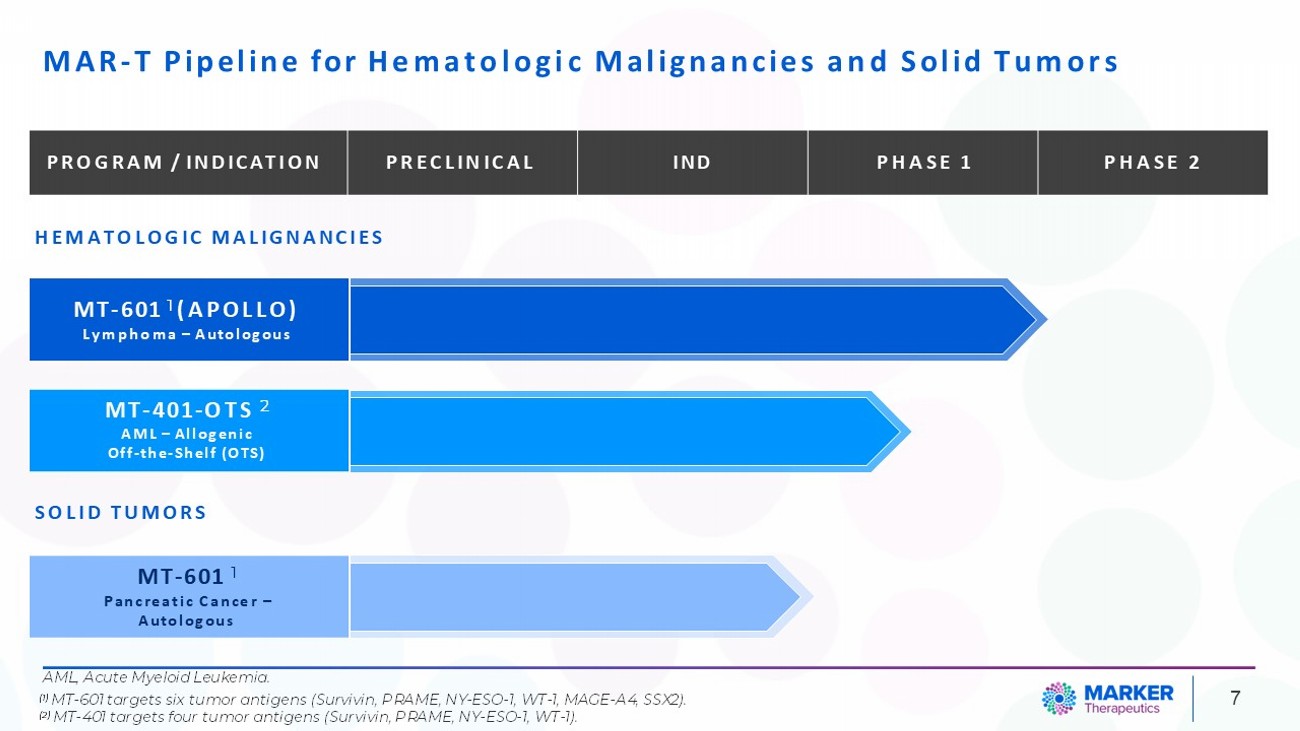
MAR - T Pipeline for Hematologic Malignancies and Solid Tumors 7 PHASE 2 PHASE 1 IND PRECLINICAL PROGRAM / INDICATION HEMATOLOGIC MALIGNANCIES MT - 601 1 (APOLLO) Lymphoma – Autologous MT - 401 - OTS 2 AML – Allogenic Off - the - Shelf (OTS) SOLID TUMORS MT - 601 1 Pancreatic Cancer – Autologous AML, Acute Myeloid Leukemia. (1) MT - 601 targets six tumor antigens (Survivin, PRAME, NY - ESO - 1, WT - 1, MAGE - A4, SSX2). (2) MT - 401 targets four tumor antigens (Survivin, PRAME, NY - ESO - 1, WT - 1).
MT - 601 – APOLLO STUDY MAR - Ts targeting 6 tumor antigens for patients with lymphoma who relapsed after anti - CD 19 CAR - T cells or where CAR - T cell therapy is not an option 8
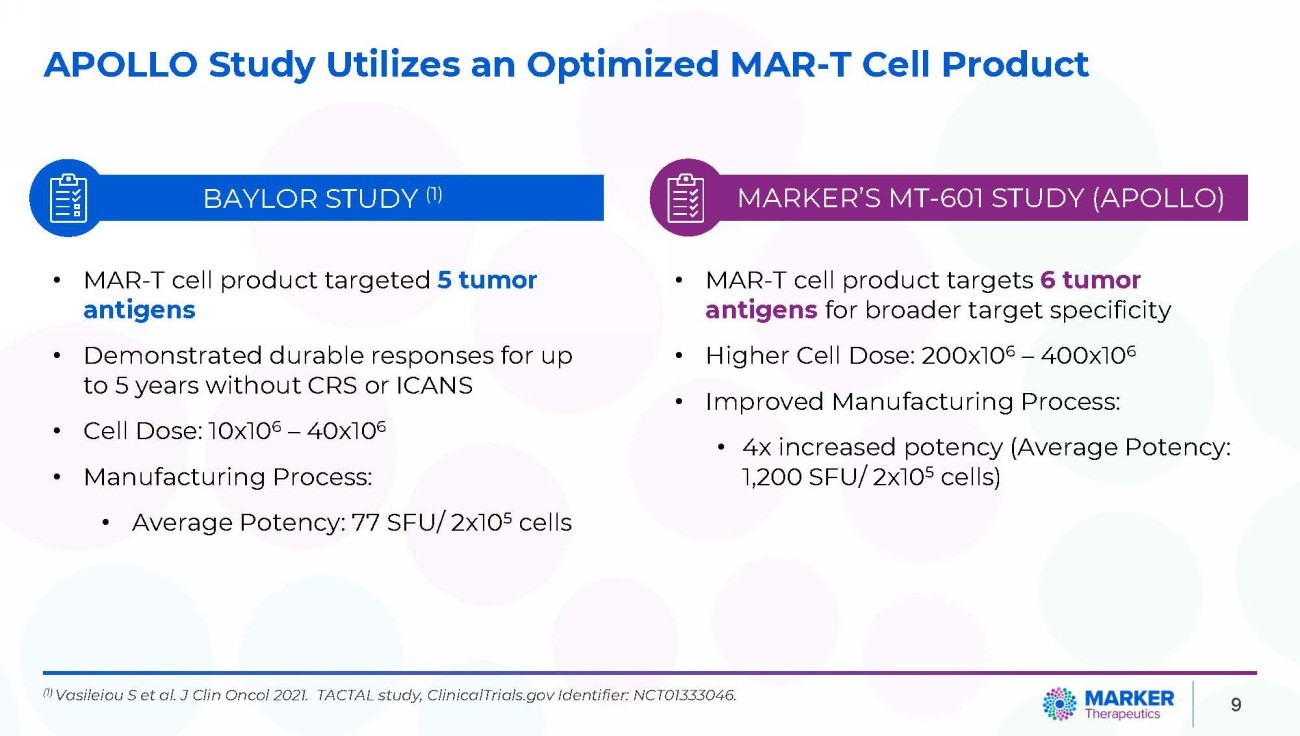
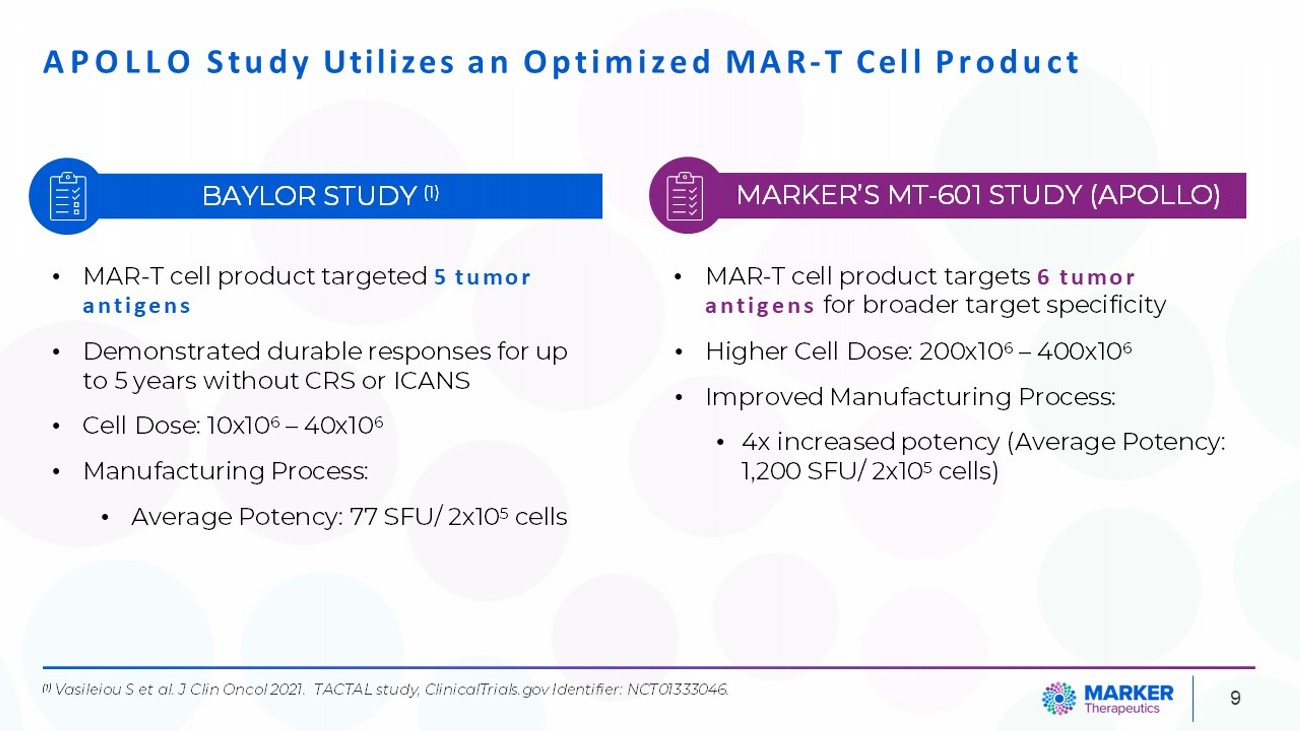
APOLLO Study Utilizes an Optimized MAR - T Cell Product 9 MARKER’S MT - 601 STUDY (APOLLO) BAYLOR STUDY (1) • MAR - T cell product targeted 5 tumor antigens • Demonstrated durable responses for up to 5 years without CRS or ICANS • Cell Dose: 10x10 6 – 40x10 6 • Manufacturing Process: • Average Potency: 77 SFU/ 2x10 5 cells • MAR - T cell product targets 6 tumor antigens for broader target specificity • Higher Cell Dose: 200x10 6 – 400x10 6 • Improved Manufacturing Process: • 4x increased potency (Average Potency: 1,200 SFU/ 2x10 5 cells) (1) Vasileiou S et al. J Clin Oncol 2021. TACTAL study, ClinicalTrials.gov Identifier: NCT01333046.
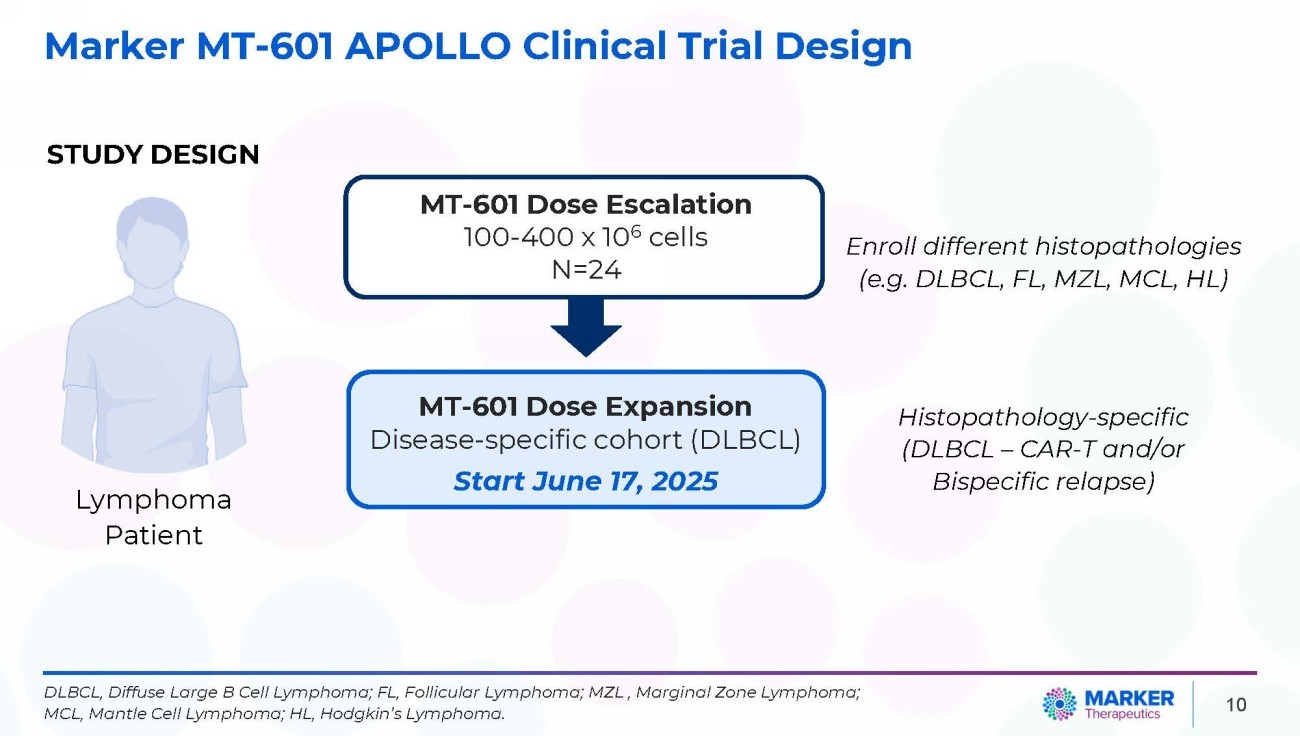
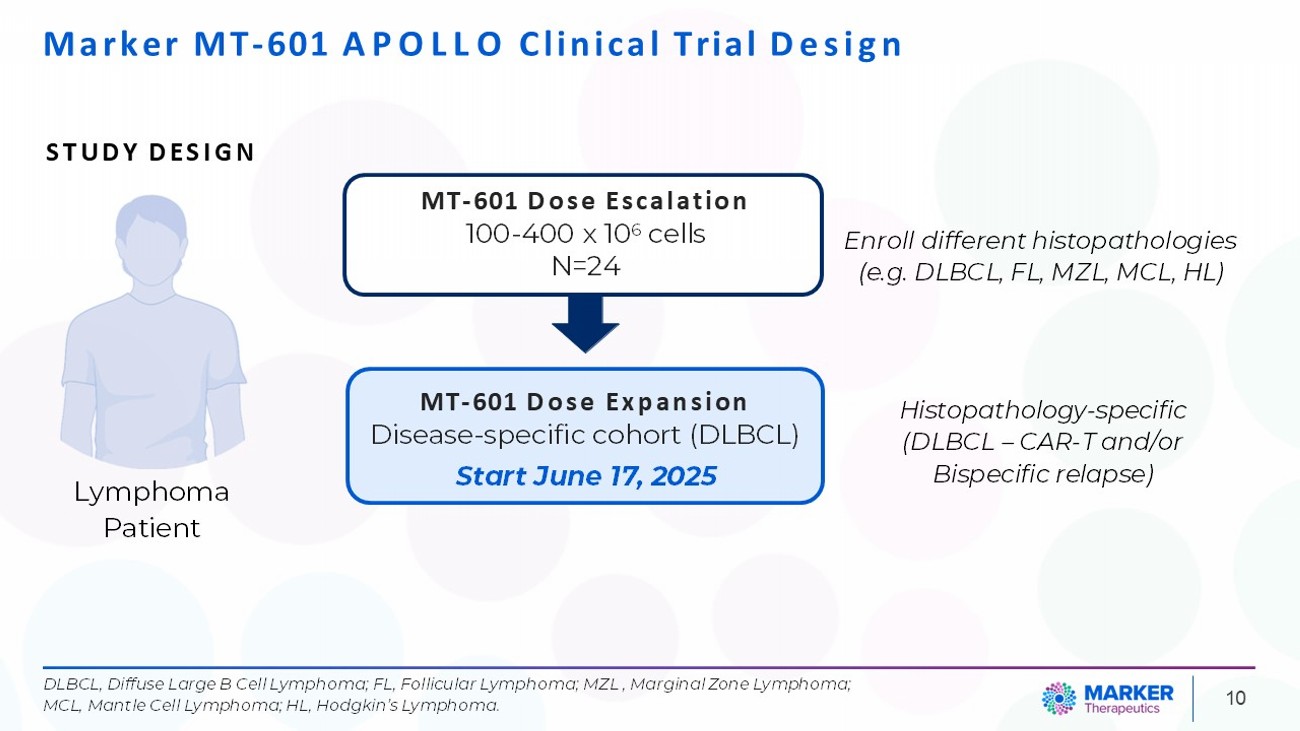
Marker MT - 601 APOLLO Clinical Trial Design Lymphoma Patient 10 MT - 601 Dose Escalation 100 - 400 x 10 6 cells N=24 STUDY DESIGN Enroll different histopathologies (e.g. DLBCL, FL, MZL, MCL, HL) Histopathology - specific (DLBCL – CAR - T and/or Bispecific relapse) DLBCL, Diffuse Large B Cell Lymphoma; FL, Follicular Lymphoma; MZL , Marginal Zone Lymphoma; MCL, Mantle Cell Lymphoma; HL, Hodgkin’s Lymphoma. MT - 601 Dose Expansion Disease - specific cohort (DLBCL) Start June 17, 2025
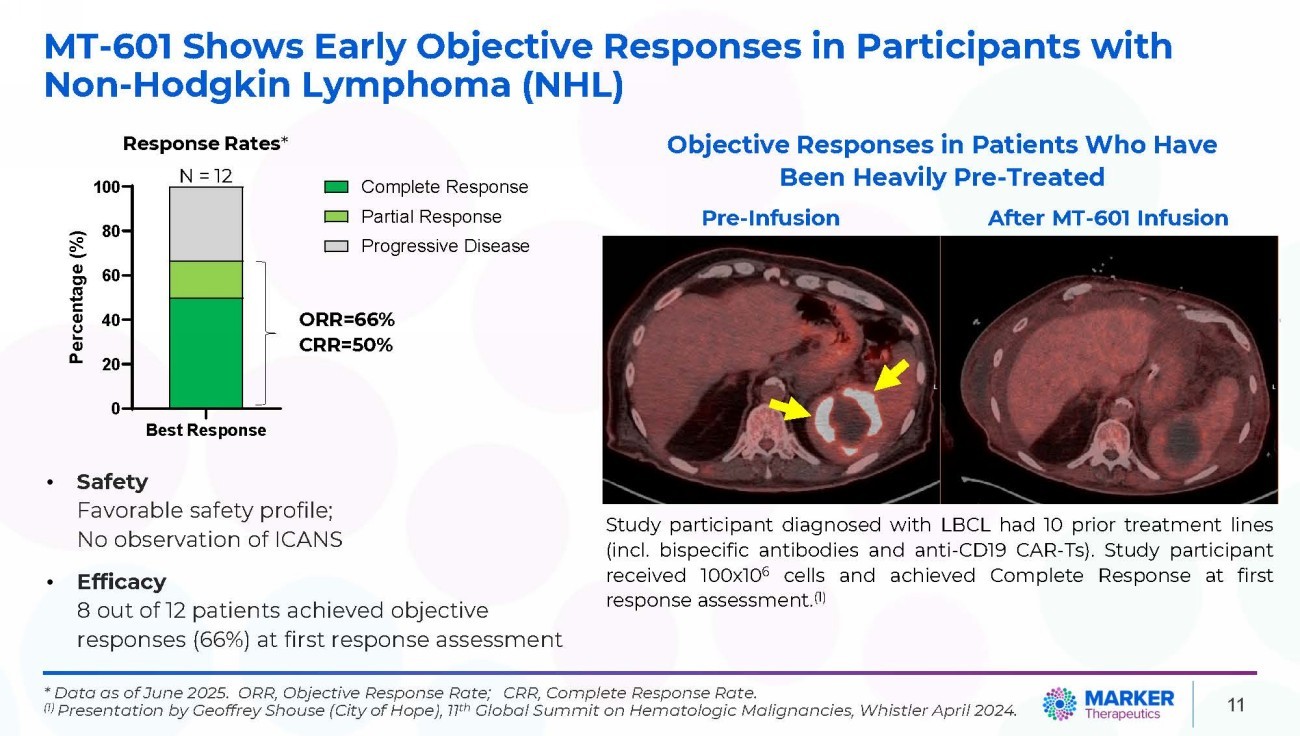
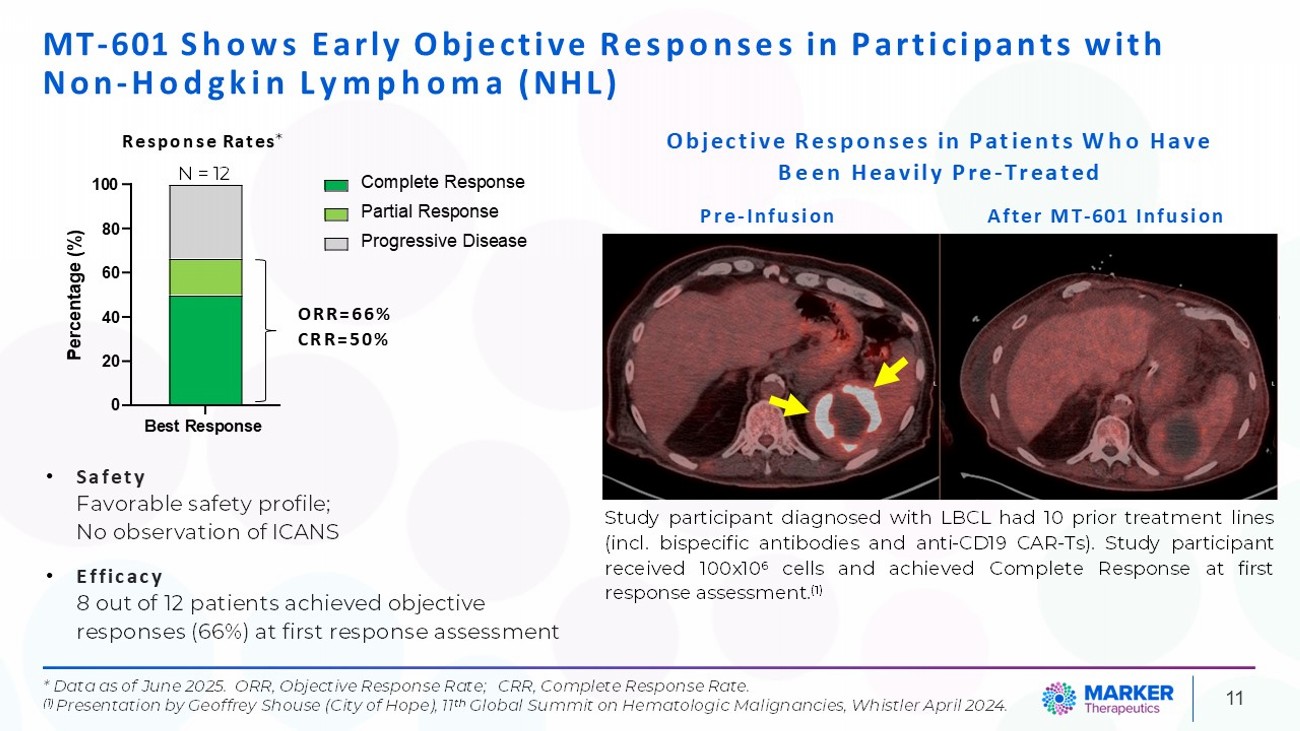
MT - 601 Shows Early Objective Responses in Participants with Non - Hodgkin Lymphoma (NHL) 20 0 Best Response 40 60 80 100 Percentage (%) Complete Response Partial Response Progressive Disease ORR=66% CRR=50% N = 12 Study participant diagnosed with LBCL had 10 prior treatment lines (incl . bispecific antibodies and anti - CD 19 CAR - Ts) . Study participant received 100 x 10 6 cells and achieved Complete Response at first response assessment . ( 1 ) Objective Responses in Patients Who Have Been Heavily Pre - Treated Pre - Infusion After MT - 601 Infusion 11 * Data as of June 2025. ORR, Objective Response Rate; CRR, Complete Response Rate. (1) Presentation by Geoffrey Shouse (City of Hope), 11 th Global Summit on Hematologic Malignancies, Whistler April 2024. • Safety Favorable safety profile; No observation of ICANS • Efficacy 8 out of 12 patients achieved objective responses (66%) at first response assessment Response Rates *
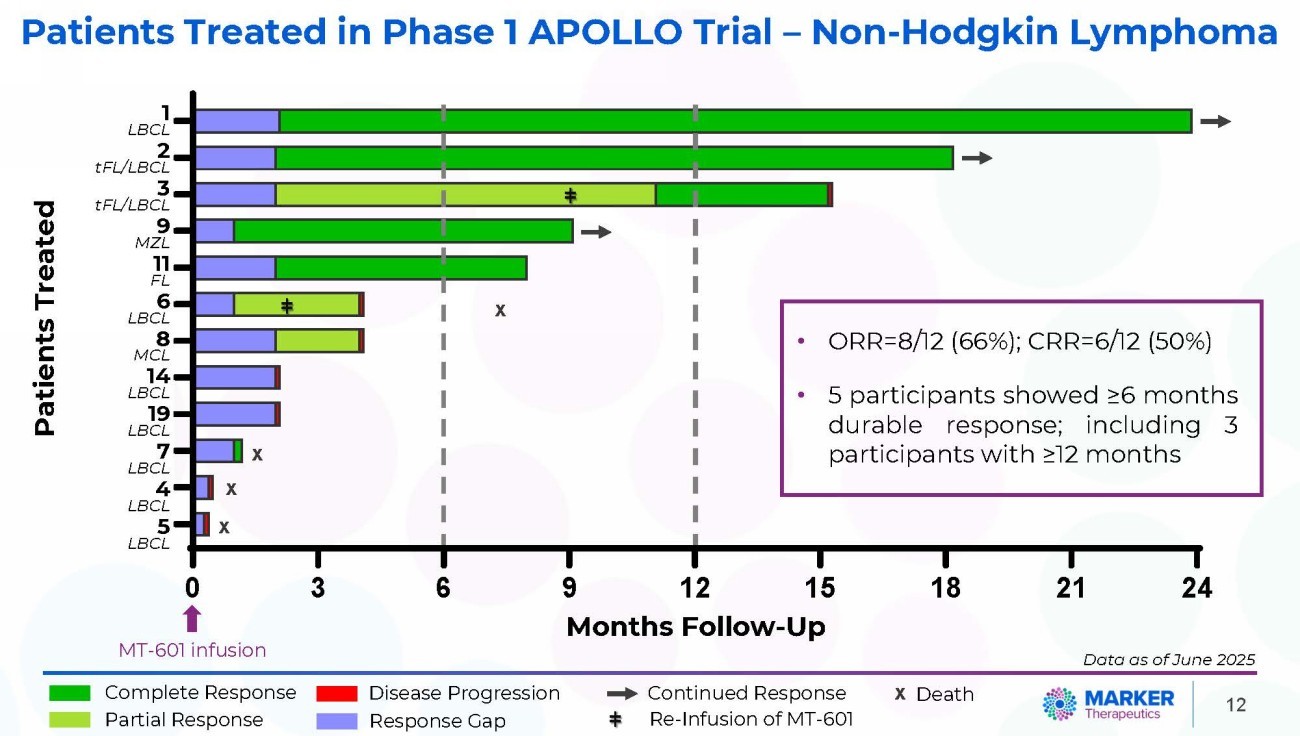
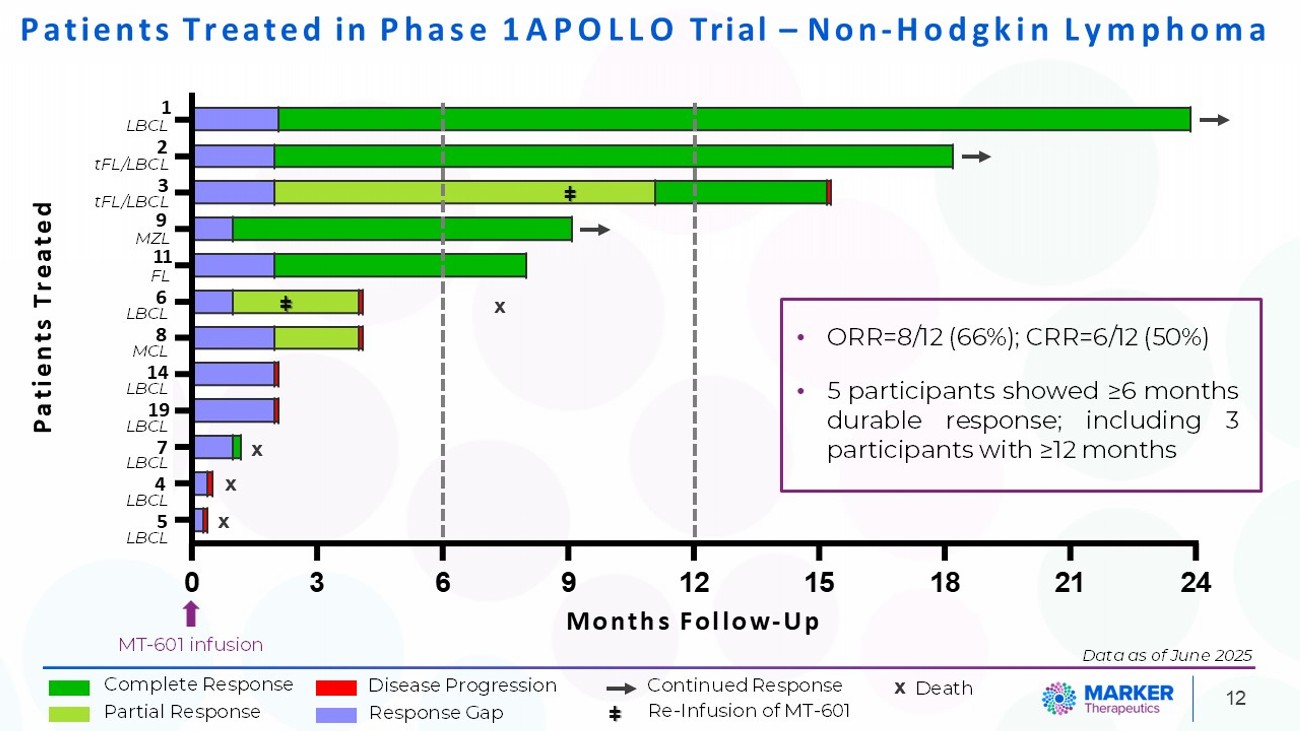
0 3 6 18 007 - 601 007 - 603 007 - 604 009 - 603 008 - 601 009 - 601 010 - 601 010 - 602 004 - 602 007 - 602 001 - 602 005 - 601 Patients Treated 12 Patients Treated in Phase 1 APOLLO Trial – Non - Hodgkin Lymphoma 9 12 15 Months Follow - Up MT - 601 infusion ǂ Complete Response Partial Response ǂ Continued Response Re - Infusion of MT - 601 ǂ x Death x x x x Disease Progression Response Gap • ORR=8/12 (66%); CRR=6/12 (50%) • 5 participants showed ≥ 6 months durable response ; including 3 participants with ≥ 12 months Patients Treated 1 LBCL 2 tFL/LBCL 3 tFL/LBCL 9 MZL 11 FL 6 LBCL 8 MCL 14 LBCL 19 LBCL 7 LBCL 4 LBCL 5 LBCL 21 24 Data as of June 2025
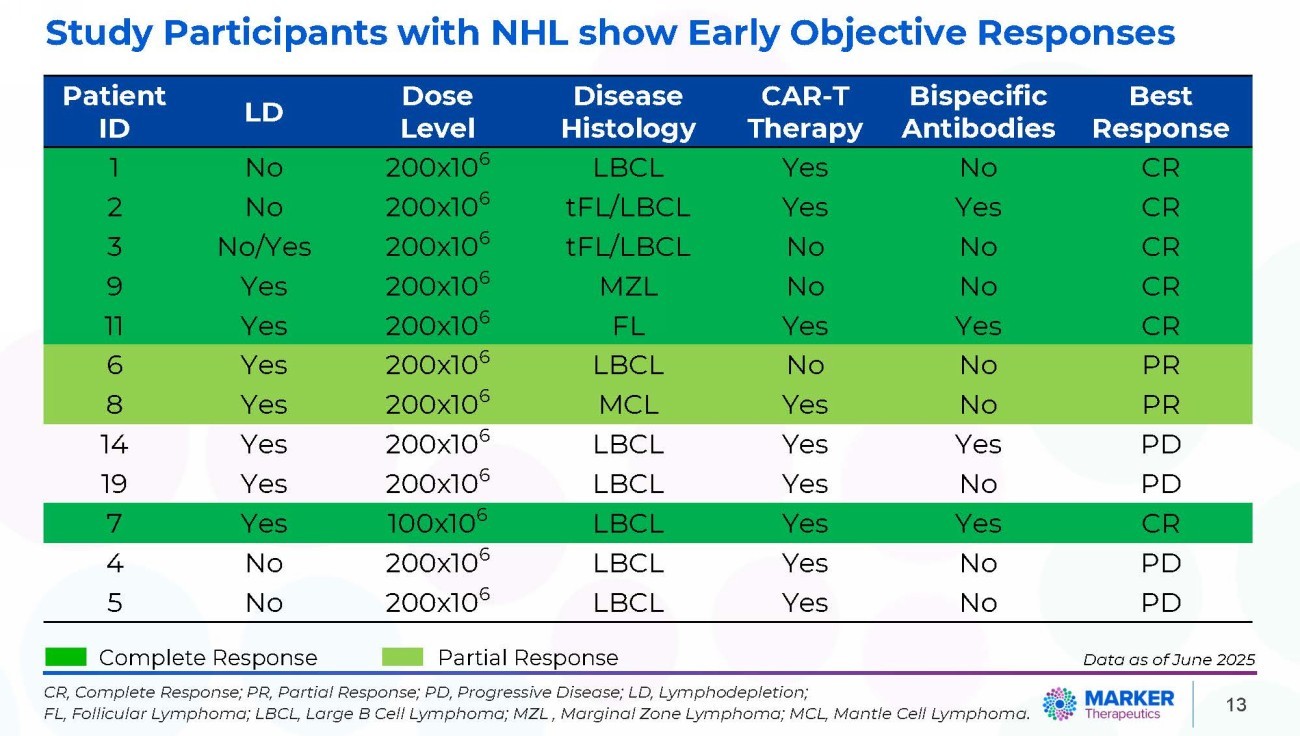
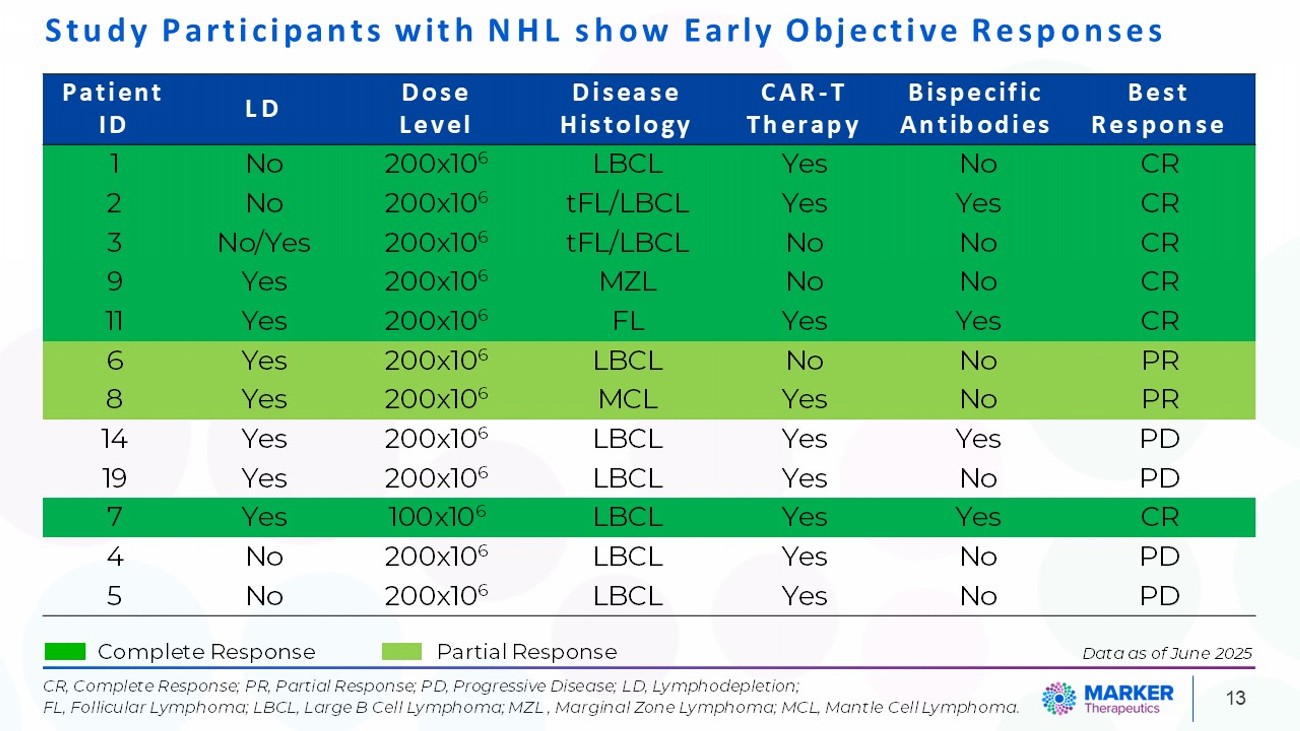
13 Study Participants with NHL show Early Objective Responses Complete Response Partial Response CR, Complete Response; PR, Partial Response; PD, Progressive Disease; LD, Lymphodepletion; FL, Follicular Lymphoma; LBCL, Large B Cell Lymphoma; MZL , Marginal Zone Lymphoma; MCL, Mantle Cell Lymphoma. Best Response Bispecific Antibodies CAR - T Therapy Disease Histology Dose Level LD Patient ID CR No Yes LBCL 200x10 6 No 1 CR Yes Yes tFL/LBCL 200x10 6 No 2 CR No No tFL/LBCL 200x10 6 No/Yes 3 CR No No MZL 200x10 6 Yes 9 CR Yes Yes FL 200x10 6 Yes 11 PR No No LBCL 200x10 6 Yes 6 PR No Yes MCL 200x10 6 Yes 8 PD Yes Yes LBCL 200x10 6 Yes 14 PD No Yes LBCL 200x10 6 Yes 19 CR Yes Yes LBCL 100x10 6 Yes 7 PD No Yes LBCL 200x10 6 No 4 PD No Yes LBCL 200x10 6 No 5 Data as of June 2025
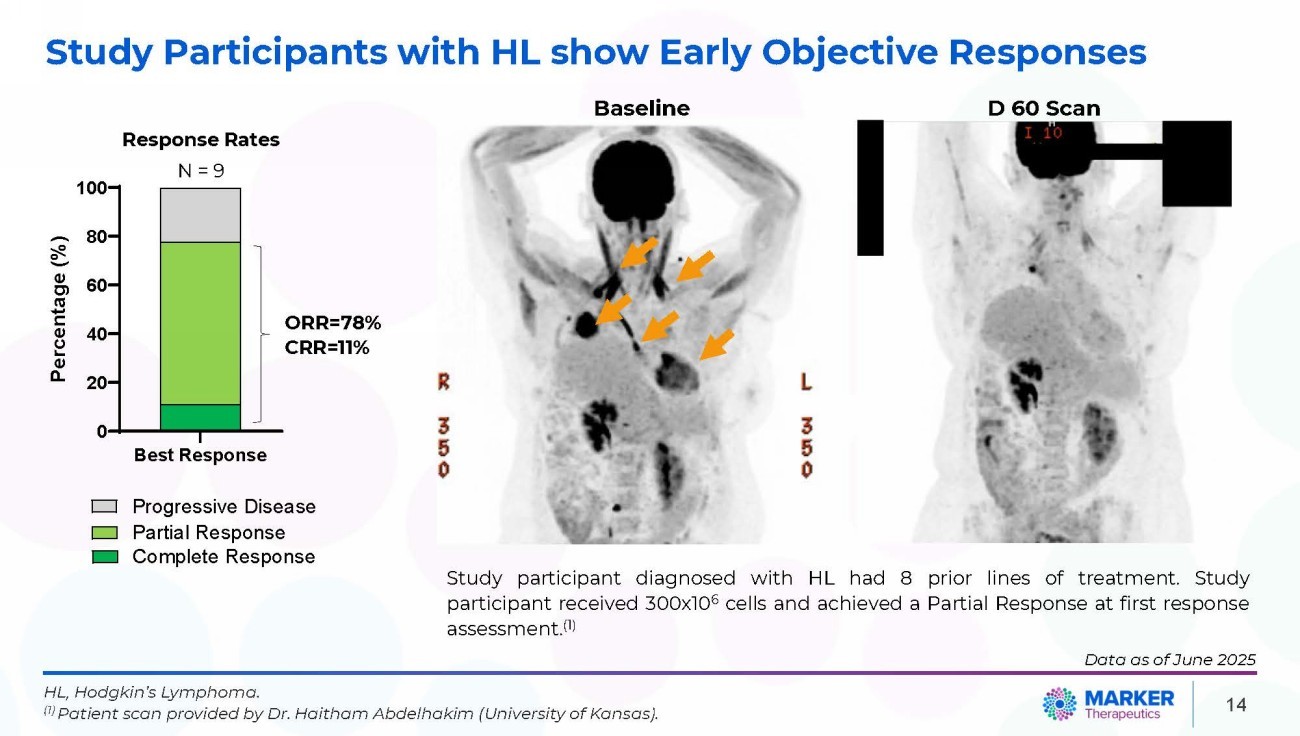
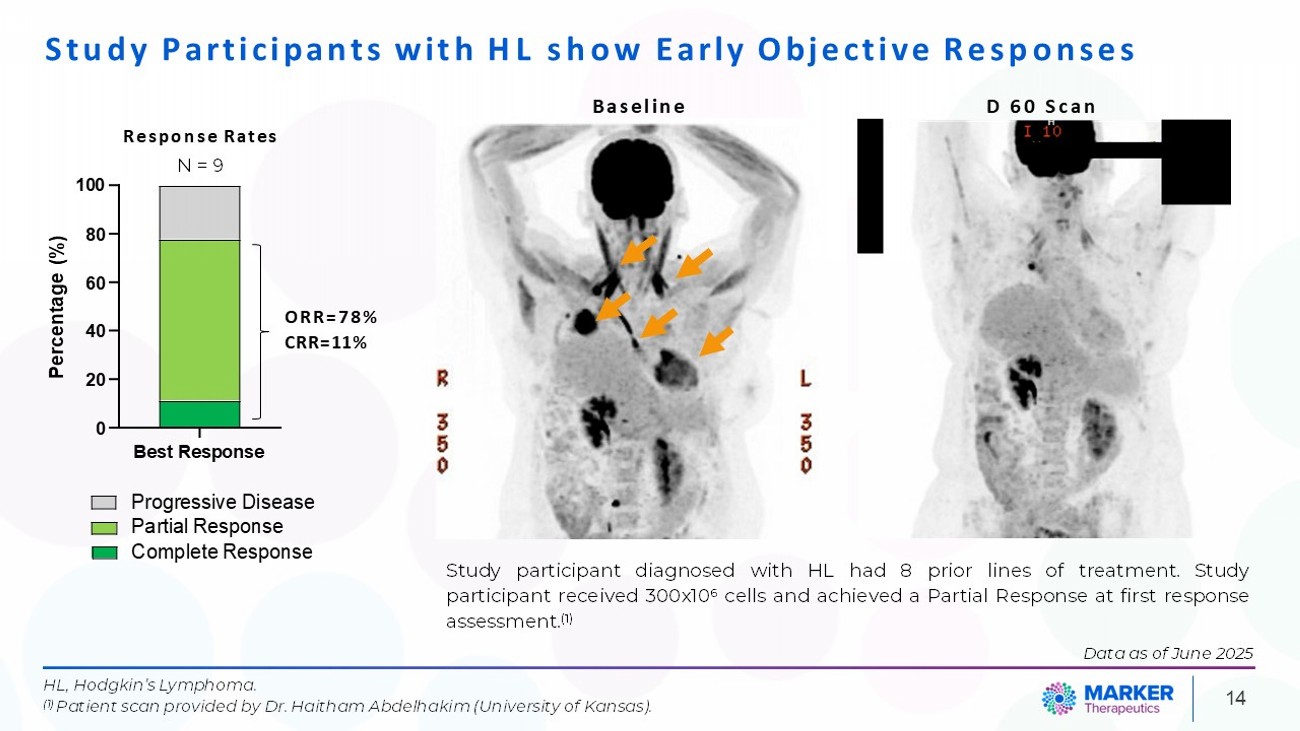
14 Study Participants with HL show Early Objective Responses HL, Hodgkin’s Lymphoma. (1) Patient scan provided by Dr. Haitham Abdelhakim (University of Kansas). 40 Percentage (%) 20 0 Best Response Progressive Disease Partial Response Complete Response Response Rates N = 9 100 80 60 ORR=78% CRR=11% Baseline D 60 Scan Study participant diagnosed with HL had 8 prior lines of treatment . Study participant received 300 x 10 6 cells and achieved a Partial Response at first response assessment . ( 1 ) Data as of June 2025
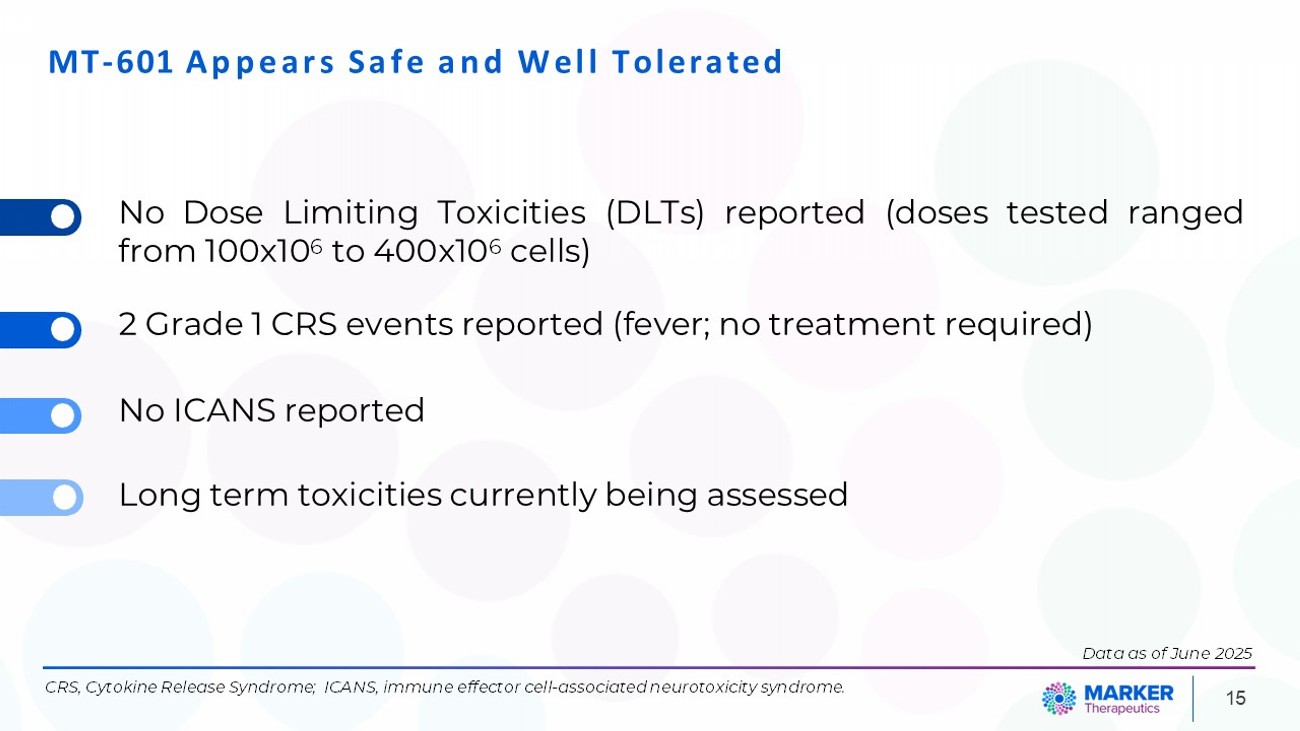
MT - 601 Appears Safe and Well Tolerated No Dose Limiting Toxicities (DLTs) reported (doses tested ranged from 100x10 6 to 400x10 6 cells) 2 Grade 1 CRS events reported (fever; no treatment required) No ICANS reported Long term toxicities currently being assessed CRS, Cytokine Release Syndrome; ICANS, immune effector cell - associated neurotoxicity syndrome. 15 Data as of June 2025
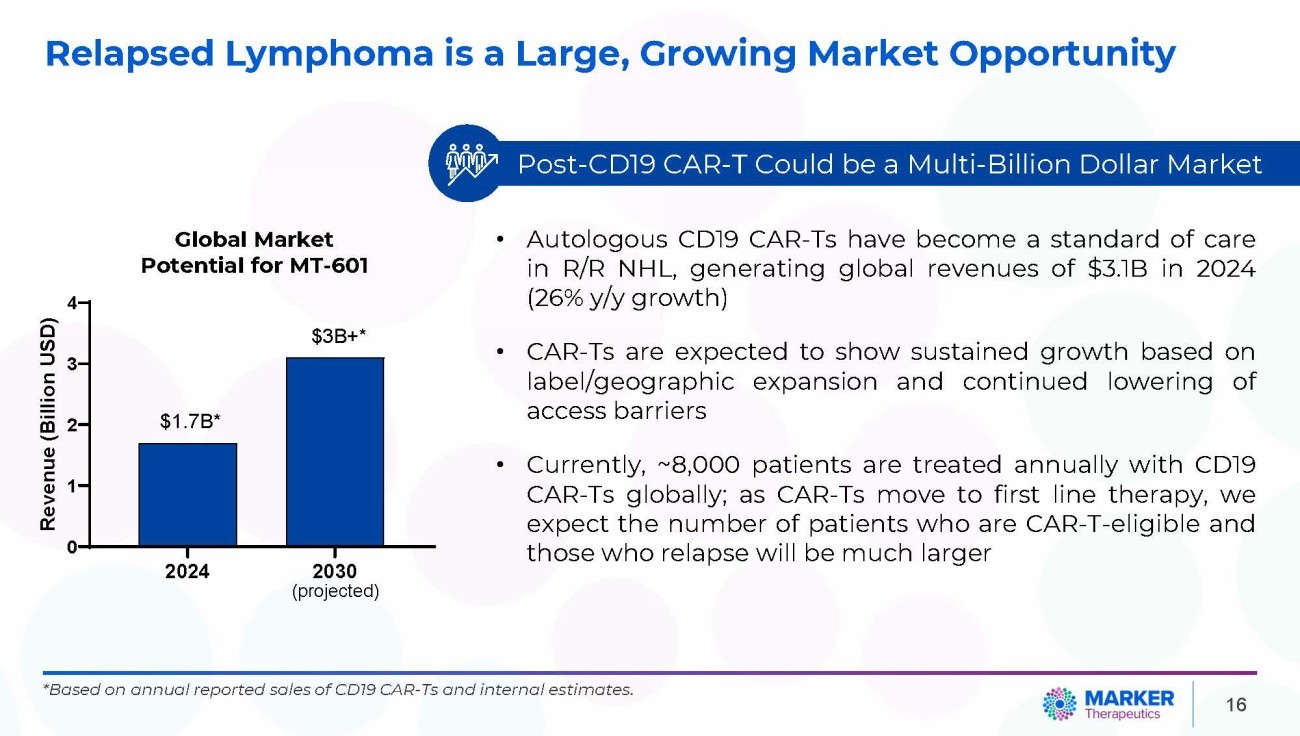
16 Relapsed Lymphoma is a Large, Growing Market Opportunity • Autologous CD 19 CAR - Ts have become a standard of care in R/R NHL, generating global revenues of $ 3 . 1 B in 2024 ( 26 % y/y growth) • CAR - Ts are expected to show sustained growth based on label/geographic expansion and continued lowering of access barriers • Currently, ~ 8 , 000 patients are treated annually with CD 19 CAR - Ts globally ; as CAR - Ts move to first line therapy, we expect the number of patients who are CAR - T - eligible and those who relapse will be much larger Global Market Potential for MT - 601 *Based on annual reported sales of CD19 CAR - Ts and internal estimates. 2024 0 1 2 3 4 Revenue (Billion USD) $1.7B* $3B+* 2030 (projected) Post - CD19 CAR - T Could be a Multi - Billion Dollar Market
Future Developments 17
MT - 401 - OTS & MT - 601 – Advancing Allogeneic and Solid Tumor Programs 18 MT - 401 Off - the - Shelf MT - 601 in Pancreatic Cancer • Manufactured from healthy donors ; Marker has cellular inventory with plans to expand • PoC studies completed with data supporting clinical benefits of technology • IND to investigate MT - 401 in an “Off - the - Shelf” setting (MT - 401 - OTS) in AML or Myelodysplastic Syndrome (MDS) granted by FDA • Orphan Drug Designation granted by FDA and the European Medicines Agency (EMA) • Non - dilutive funding from FDA, CPRIT and NIH to support clinical investigation of MT - 401 - OTS in patients with AML • FDA has granted an IND to investigate MT - 601 in patients with metastatic pancreatic cancer in combination with front - line chemotherapy • Marker received $ 9 . 5 million from CPRIT and $ 2 million from NIH SBIR to support the investigation of MT - 601 in patients with pancreatic cancer PoC, Proof - of - Concept.
Key Takeaways 19 In contrast to single antigen - targeting T cell therapies, MAR - Ts target multiple epitopes within up to 6 tumor - specific antigens, thereby reducing the possibility of tumor escape MAR - Ts do not require genetic engineering APOLLO study highlights: • MT - 601 was well - tolerated with no signs of ICANS. • 8 out of 12 NHL patients (ORR=66%) achieved objective responses, incl. 6 complete responses (CRR=50%). • 7 out of 9 HL patients (ORR=78%) achieved objective responses, incl. 1 complete response (CRR=11%). Cash and cash equivalents of $11.8M*; Current cash runway expected to finance Company into Q2 2026 (assuming no additional grant funds are received) *as of June 30, 2025.
THANK YOU 20
Exhibit 99.3

MARKER THERAPEUTICS CORPORATE PRESENTATION August 26, 2025 NASDAQ: MRKR
Forward Looking Statements Certain statements contained herein are forward - looking statements within the meaning of Section 21 E of the Securities Exchange Act of 1934 , as amended, and Section 27 A of the Securities Act of 1933 , as amended, that involve risks and uncertainties . All statements other than statements relating to historical matters including statements to the effect that we “believe”, “expect”, “anticipate”, “plan”, “target”, “intend” and similar expressions, including without limitation statements regarding Marker Therapeutics, Inc . ’s (“Marker” or the “Company”) intentions, beliefs, projections, outlook, analyses or current expectations are “forward - looking statements” . Forward - looking statements include statements concerning, among other things : the Company’s research, development and regulatory activities and expectations relating to its non - engineered multi - antigen recognizing (MAR) T cell therapies ; the effectiveness of the Company’s programs or the possible range of application and potential curative effects and safety in the treatment of diseases ; the timing, conduct and success of the Company’s clinical trials of its product candidates, including MT - 401 for the treatment of patients with Acute Myeloid Leukemia (“AML”) or Myelodysplastic Syndrome (“MDS”), MT - 401 Off - the - Shelf (“OTS”) for the treatment of patients with AML, and MT - 601 for the treatment of patients with relapsed lymphoma ; the Company’s long - term stability and cash runway ; the Company’s optimized manufacturing process ; and the future development of MAR - T cell therapies (formerly known as multiTAA - specific T cells) . Forward - looking statements are by their nature subject to risks, uncertainties and other factors which could cause actual results to differ materially from those stated in such statements . Such risks, uncertainties and factors include, but are not limited to the risks set forth in the Company’s most recent Forms 10 - K, 10 - Q and other SEC filings which are available through EDGAR at WWW . SEC . GOV . No representation or warranty (expressed or implied) is made as to, and no reliance should be placed on, the fairness, accuracy or completeness of the information contained herein . Accordingly, none of the Company, or any of its principals, partners, subsidiaries or affiliates, or any of such person’s board members, officers or employees accepts any liability whatsoever arising directly or indirectly from the use of this presentation . Certain information set forth herein includes estimates, projections and targets and involves significant elements of subjective judgement and analysis, which may or may not be correct . No representations are made as to the accuracy of such estimates, projections or targets or that all assumptions relating to such estimates, projections or targets have been considered or stated or that such estimates, projections or targets will be realized . This presentation does not purport to contain all of the information that may be required to evaluate the Company and any recipient hereof should conduct its own independent analysis of the Company and the data and information contained herein . Any forward - looking statements are not guarantees of future performance and actual results may differ materially from estimates in the forward - looking statements . Unless otherwise stated, all information in this presentation is as of the date of the cover page of this presentation, and the Company undertakes no obligation to revise these forward - looking statements to reflect events or circumstances that arise after the date hereof . 2
3 MAR - T Cell Platform MAR - T (Multi - Antigen Recognizing T cell, formerly known as multiTAA) technology was developed at Baylor College of Medicine and, we believe, offers key therapeutic and manufacturing advantages over traditional T cell therapies Attractive Safety Profile MAR - T cells are non - genetically engineered and were well - tolerated in clinical trials to date, with a favorable safety profile and no observation of immune - effector cell associated neurotoxicity syndrome (ICANS) attributed to MAR - T cell technology MT - 601 – Lead Clinical Product Marker’s lead product, MT - 601 , targets 6 tumor - specific antigens (Survivin, PRAME, NY - ESO - 1 , MAGE - A 4 , SSX 2 , WT - 1 ) for a broad tumor recognition MT - 601 - APOLLO Study MT - 601 in Phase 1 clinical trial has shown durable objective response rates in patients with lymphoma who relapsed after anti - CD 19 CAR - T cells or where CAR - T cell therapy is not an option Multiple INDs & Strong IP Position FDA cleared INDs for three MAR - T based clinical programs Strong IP position and world - wide exclusive license on MAR - T technology from Baylor College of Medicine Non - Dilutive Funding Support Ongoing efforts to obtain non - dilutive funding ; to date Marker was awarded over $ 30 million non - dilutive funding (NIH, FDA, CPRIT) Marker Therapeutics – Value Proposition

MAR - T Technology 4
5 • MAR - T cells target up to 6 antigens 1, 2 for a more potent, durable anti - tumor response. • MAR - T cells lack genetic modification; Natural T cells expanded ex vivo pose no mutagenesis risk. • MAR - Ts intend to address challenges faced by Bispecific Antibodies, CAR - T and TCR approaches. • MAR - T platform technology developed at Baylor College of Medicine. Mechanism of Action of MAR - T Cells (1) MT - 601 targets six tumor antigens (Survivin, PRAME, NY - ESO - 1, WT - 1, MAGE - A4, SSX2). (2) MT - 401 targets four tumor antigens (Survivin, PRAME, NY - ESO - 1, WT - 1). Overlapping peptides PBMC isolation MAR - T cells Activation Expansion & Infusion Apoptosis PRAME Survivin WT - 1 NY - ESO - 1 SSX2 MAGE - A4 Tumor cell TCR TRAIL FASL MAR - T cells Multi Antigen Recognition Multi Epitope Recognition Low Risk for CR S o r ICANS For Blood & S ol id Tumors Intra - & Extra - Cellular Targets No Genetic Engineering
• No genetic engineering • Natural T cell expansion • Uninterrupted cell expansion • Reproducible process • Cost - effective process PBMC, peripheral blood mononuclear cells. 6 MAR - T Cells are Generated in a Simple Manufacturing Process
MAR - T Pipeline for Hematologic Malignancies and Solid Tumors 7 PHASE 2 PHASE 1 IND PRECLINICAL PROGRAM / INDICATION HEMATOLOGIC MALIGNANCIES MT - 601 1 (APOLLO) Lymphoma – Autologous MT - 401 - OTS 2 AML – Allogenic Off - the - Shelf (OTS) SOLID TUMORS MT - 601 1 Pancreatic Cancer – Autologous AML, Acute Myeloid Leukemia. (1) MT - 601 targets six tumor antigens (Survivin, PRAME, NY - ESO - 1, WT - 1, MAGE - A4, SSX2). (2) MT - 401 targets four tumor antigens (Survivin, PRAME, NY - ESO - 1, WT - 1).
MT - 601 – APOLLO STUDY MAR - Ts targeting 6 tumor antigens for patients with lymphoma who relapsed after anti - CD 19 CAR - T cells or where CAR - T cell therapy is not an option 8
APOLLO Study Utilizes an Optimized MAR - T Cell Product 9 MARKER’S MT - 601 STUDY (APOLLO) BAYLOR STUDY (1) • MAR - T cell product targeted 5 tumor antigens • Demonstrated durable responses for up to 5 years without CRS or ICANS • Cell Dose: 10x10 6 – 40x10 6 • Manufacturing Process: • Average Potency: 77 SFU/ 2x10 5 cells • MAR - T cell product targets 6 tumor antigens for broader target specificity • Higher Cell Dose: 200x10 6 – 400x10 6 • Improved Manufacturing Process: • 4x increased potency (Average Potency: 1,200 SFU/ 2x10 5 cells) (1) Vasileiou S et al. J Clin Oncol 2021. TACTAL study, ClinicalTrials.gov Identifier: NCT01333046.
Marker MT - 601 APOLLO Clinical Trial Design Lymphoma Patient 10 MT - 601 Dose Escalation 100 - 400 x 10 6 cells N=24 STUDY DESIGN Enroll different histopathologies (e.g. DLBCL, FL, MZL, MCL, HL) Histopathology - specific (DLBCL – CAR - T and/or Bispecific relapse) DLBCL, Diffuse Large B Cell Lymphoma; FL, Follicular Lymphoma; MZL , Marginal Zone Lymphoma; MCL, Mantle Cell Lymphoma; HL, Hodgkin’s Lymphoma. MT - 601 Dose Expansion Disease - specific cohort (DLBCL) Start June 17, 2025
MT - 601 Shows Early Objective Responses in Participants with Non - Hodgkin Lymphoma (NHL) 20 0 Best Response 40 60 80 100 Percentage (%) Complete Response Partial Response Progressive Disease ORR=66% CRR=50% N = 12 Study participant diagnosed with LBCL had 10 prior treatment lines (incl . bispecific antibodies and anti - CD 19 CAR - Ts) . Study participant received 100 x 10 6 cells and achieved Complete Response at first response assessment . ( 1 ) Objective Responses in Patients Who Have Been Heavily Pre - Treated Pre - Infusion After MT - 601 Infusion 11 • Safety Favorable safety profile; No observation of ICANS • Efficacy 8 out of 12 patients achieved objective responses (66%) at first response assessment Response Rates * * Data as of June 2025. ORR, Objective Response Rate; CRR, Complete Response Rate. (1) Presentation by Geoffrey Shouse (City of Hope), 11 th Global Summit on Hematologic Malignancies, Whistler April 2024.
0 3 6 18 007 - 601 007 - 603 007 - 604 009 - 603 008 - 601 009 - 601 010 - 601 010 - 602 004 - 602 007 - 602 001 - 602 005 - 601 Patients Treated 12 Patients Treated in Phase 1 APOLLO Trial – Non - Hodgkin Lymphoma 9 12 15 Months Follow - Up MT - 601 infusion ǂ Complete Response Partial Response ǂ Continued Response Re - Infusion of MT - 601 ǂ x Death x x x x Disease Progression Response Gap • ORR=8/12 (66%); CRR=6/12 (50%) • 5 participants showed ≥ 6 months durable response ; including 3 participants with ≥ 12 months Patients Treated 1 LBCL 2 tFL/LBCL 3 tFL/LBCL 9 MZL 11 FL 6 LBCL 8 MCL 14 LBCL 19 LBCL 7 LBCL 4 LBCL 5 LBCL 21 24 Data as of June 2025
13 Study Participants with NHL show Early Objective Responses Complete Response Partial Response CR, Complete Response; PR, Partial Response; PD, Progressive Disease; LD, Lymphodepletion; FL, Follicular Lymphoma; LBCL, Large B Cell Lymphoma; MZL , Marginal Zone Lymphoma; MCL, Mantle Cell Lymphoma. Best Response Bispecific Antibodies CAR - T Therapy Disease Histology Dose Level LD Patient ID CR No Yes LBCL 200x10 6 No 1 CR Yes Yes tFL/LBCL 200x10 6 No 2 CR No No tFL/LBCL 200x10 6 No/Yes 3 CR No No MZL 200x10 6 Yes 9 CR Yes Yes FL 200x10 6 Yes 11 PR No No LBCL 200x10 6 Yes 6 PR No Yes MCL 200x10 6 Yes 8 PD Yes Yes LBCL 200x10 6 Yes 14 PD No Yes LBCL 200x10 6 Yes 19 CR Yes Yes LBCL 100x10 6 Yes 7 PD No Yes LBCL 200x10 6 No 4 PD No Yes LBCL 200x10 6 No 5 Data as of June 2025
14 Study Participants with HL show Early Objective Responses HL, Hodgkin’s Lymphoma. (1) Patient scan provided by Dr. Haitham Abdelhakim (University of Kansas). 40 Percentage (%) 20 0 Best Response Progressive Disease Partial Response Complete Response Response Rates N = 9 100 80 60 ORR=78% CRR=11% Baseline D 60 Scan Study participant diagnosed with HL had 8 prior lines of treatment . Study participant received 300 x 10 6 cells and achieved a Partial Response at first response assessment . ( 1 ) Data as of June 2025
MT - 601 Appears Safe and Well Tolerated No Dose Limiting Toxicities (DLTs) reported (doses tested ranged from 100x10 6 to 400x10 6 cells) 2 Grade 1 CRS events reported (fever; no treatment required) No ICANS reported Long term toxicities currently being assessed CRS, Cytokine Release Syndrome; ICANS, immune effector cell - associated neurotoxicity syndrome. 15 Data as of June 2025
INSIGHTS FROM GEOFFREY SHOUSE, D.O., Ph.D. Assistant Professor, City of Hope, Duarte, CA
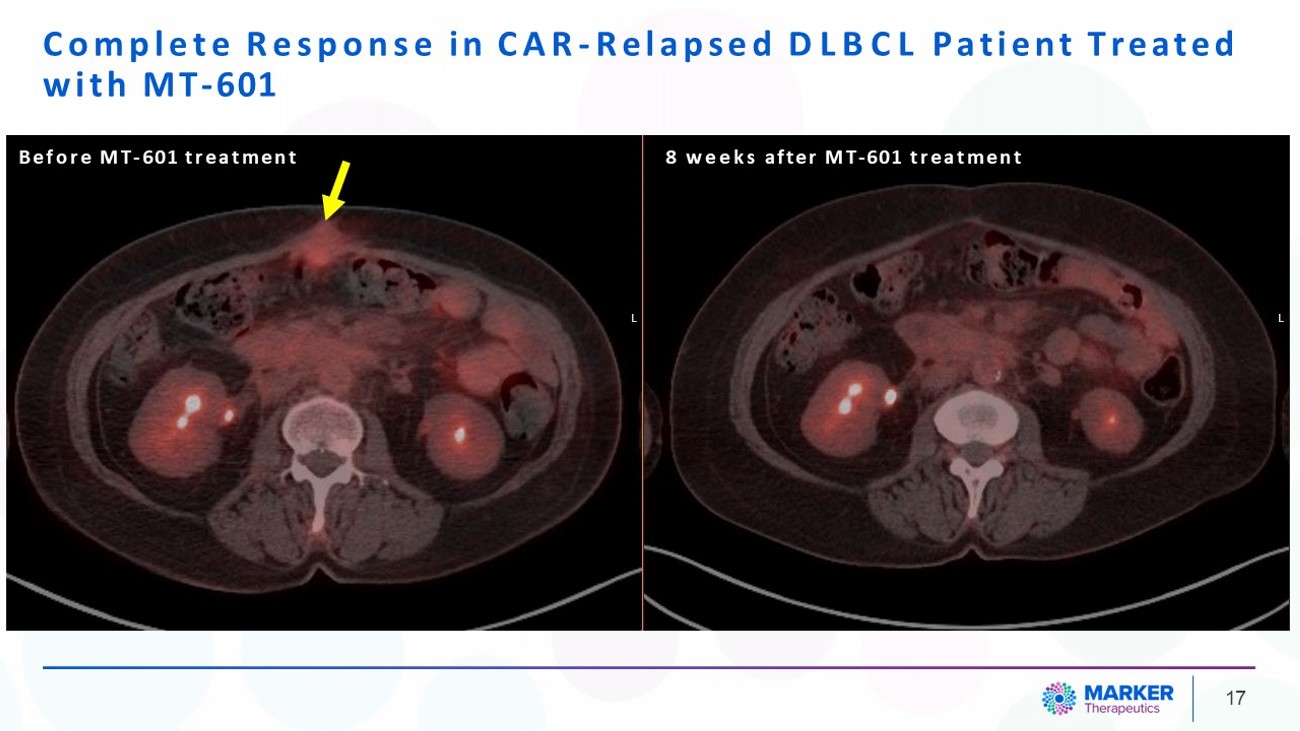
Complete Response in CAR - Relapsed DLBCL Patient Treated with MT - 601 17 Before MT - 601 treatment 8 weeks after MT - 601 treatment
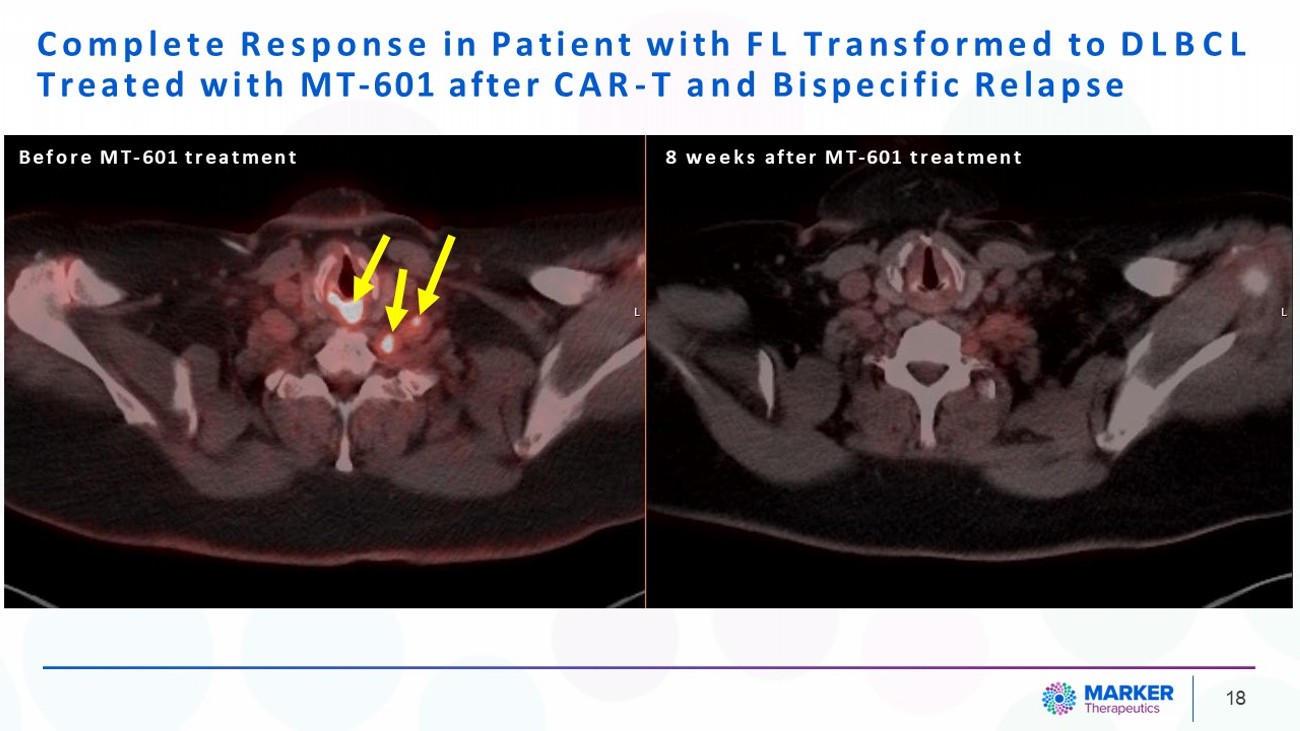
Complete Response in Patient with FL Transformed to DLBCL Treated with MT - 601 after CAR - T and Bispecific Relapse 18 Before MT - 601 treatment 8 weeks after MT - 601 treatment
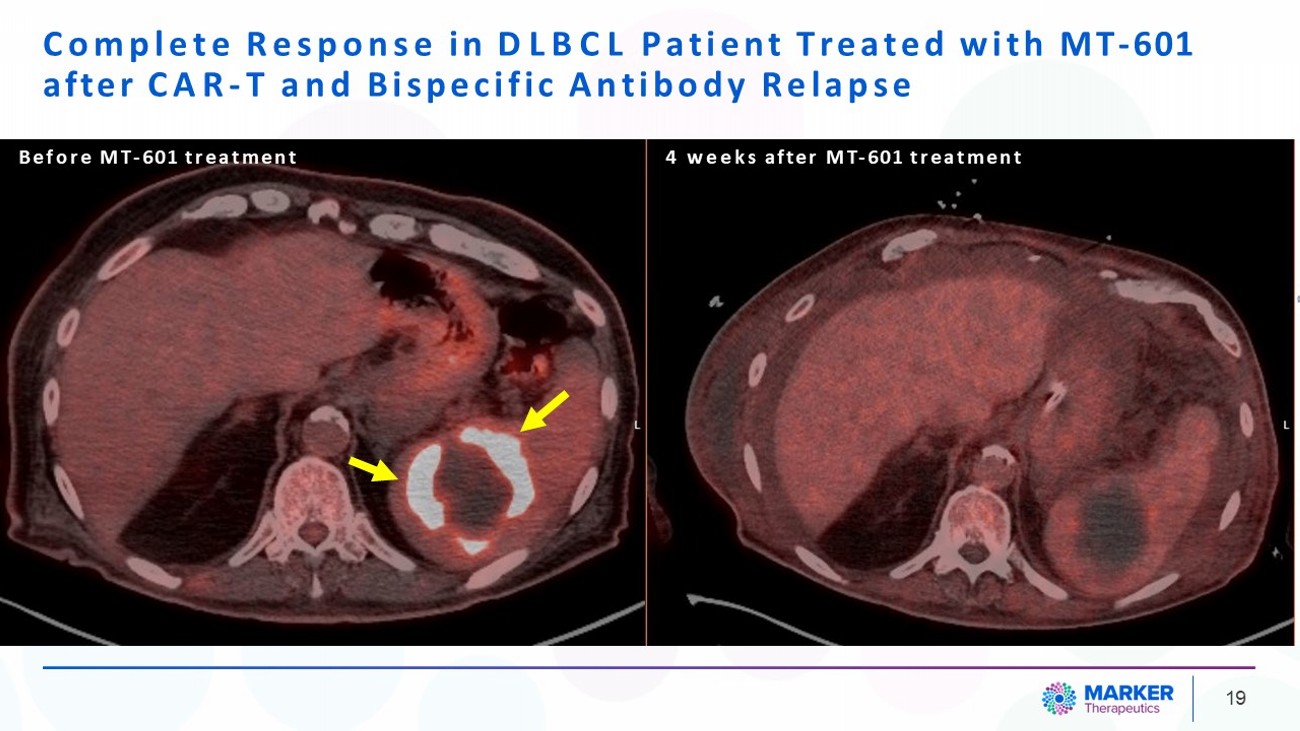
Complete Response in DLBCL Patient Treated with MT - 601 after CAR - T and Bispecific Antibody Relapse 19 Before MT - 601 treatment 4 weeks after MT - 601 treatment
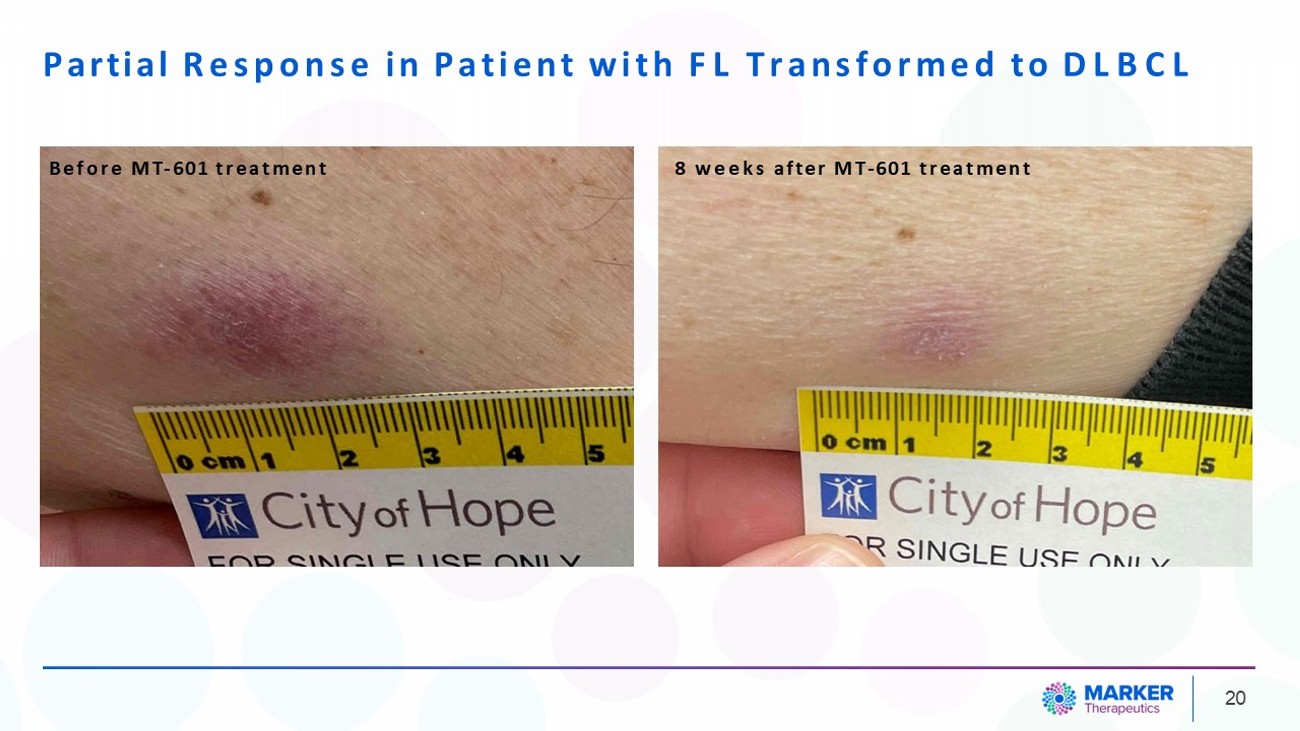
Partial Response in Patient with FL Transformed to DLBCL 20 Before MT - 601 treatment 8 weeks after MT - 601 treatment

Treatment Landscape in CAR - Relapsed DLBCL Patients
Unmet Needs in DLBCL • The treatment landscape has seen dramatic changes and continues to undergo changes associated with incorporation of novel therapies . • Even with these changes, unmet needs persist including patients that relapse after available treatments including CAR - T, stem cell transplant and those deemed not candidates for these treatments . • MT - 601 has demonstrated exceptional safety and preliminary efficacy and carries the potential to fill many of these unmet needs . 22
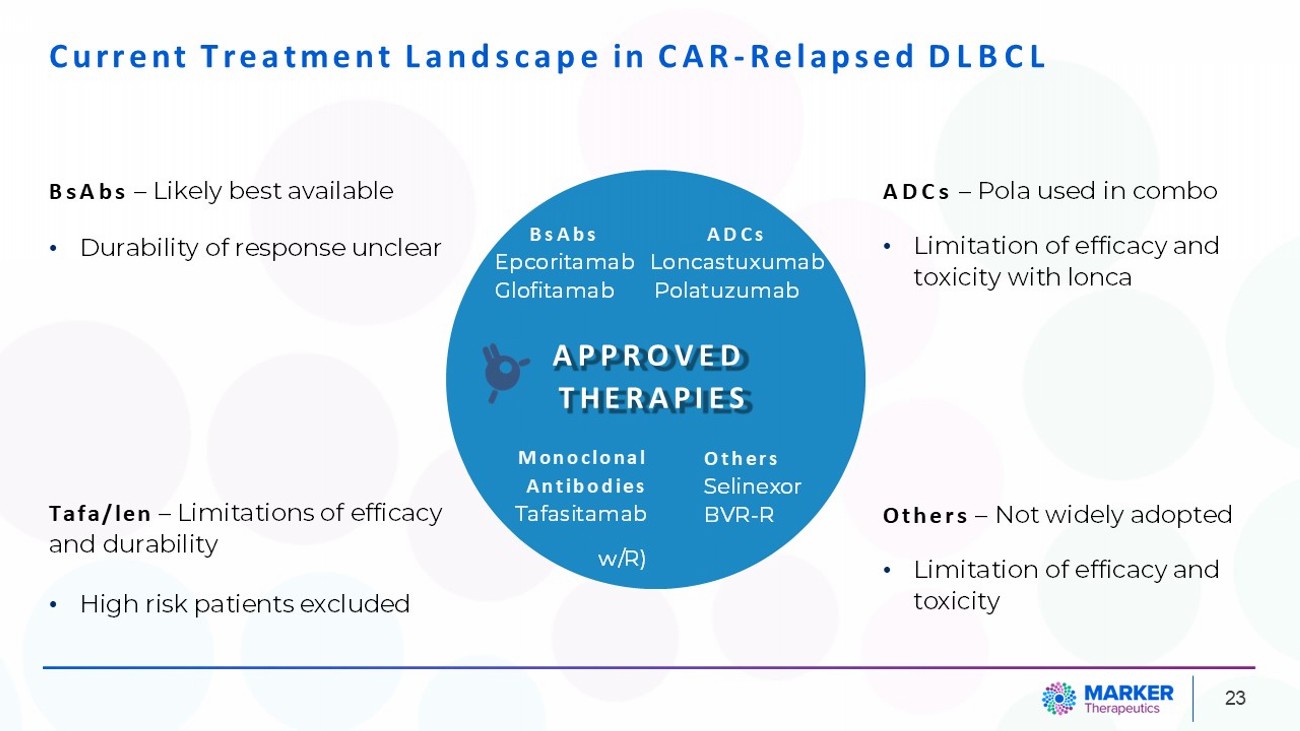
23 BsAbs ADCs Epcoritamab Loncastuxumab Glofitamab Polatuzumab APPROVED THERAPIES Monoclonal Antibodies Tafasitamab w/R) Others Selinexor BVR - R Current Treatment Landscape in CAR - Relapsed DLBCL BsAbs – Likely best available • Durability of response unclear Tafa/len – Limitations of efficacy and durability • High risk patients excluded ADCs – Pola used in combo • Limitation of efficacy and toxicity with lonca Others – Not widely adopted • Limitation of efficacy and toxicity
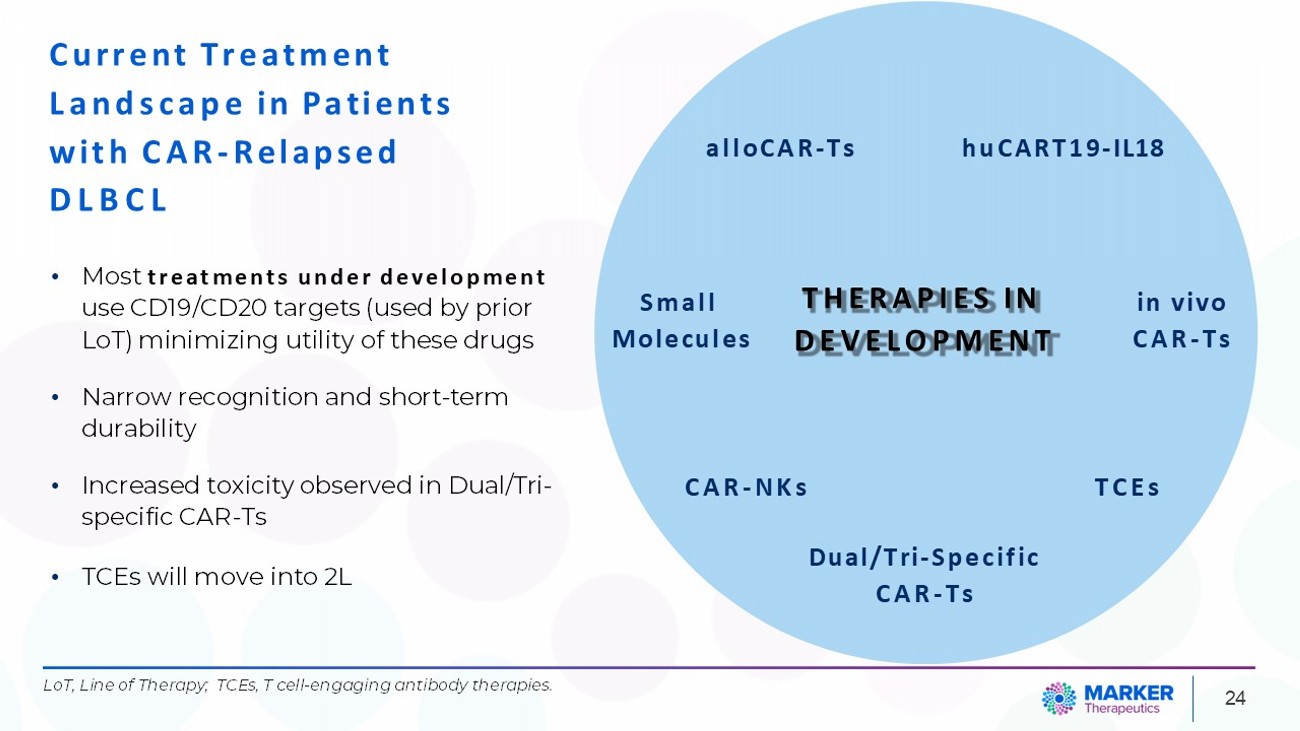
24 THERAPIES IN DEVELOPMENT alloCAR - Ts Dual/Tri - Specific CAR - Ts TCEs huCART19 - IL18 CAR - NKs in vivo CAR - Ts Small Molecules Current Treatment Landscape in Patients with CAR - Relapsed DLBCL • Most treatments under development use CD19/CD20 targets (used by prior LoT) minimizing utility of these drugs • Narrow recognition and short - term durability • Increased toxicity observed in Dual/Tri - specific CAR - Ts • TCEs will move into 2L LoT, Line of Therapy; TCEs, T cell - engaging antibody therapies.
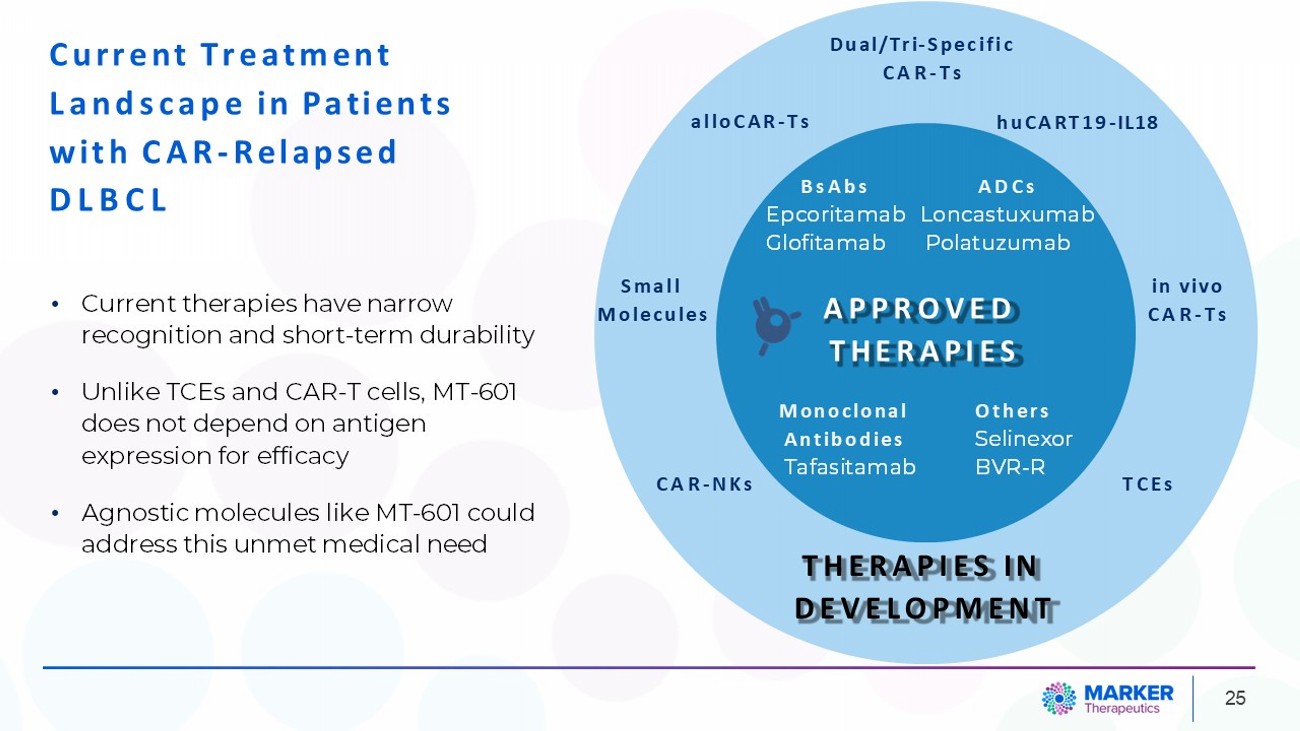
25 THERAPIES IN DEVELOPMENT BsAbs ADCs Epcoritamab Loncastuxumab Glofitamab Polatuzumab APPROVED THERAPIES Monoclonal Antibodies Tafasitamab Others Selinexor BVR - R alloCAR - Ts TCEs Dual/Tri - Specific CAR - Ts huCART19 - IL18 CAR - NKs in vivo CAR - Ts Small Molecules Current Treatment Landscape in Patients with CAR - Relapsed DLBCL • Current therapies have narrow recognition and short - term durability • Unlike TCEs and CAR - T cells, MT - 601 does not depend on antigen expression for efficacy • Agnostic molecules like MT - 601 could address this unmet medical need

MT - 601 Poised to Fill Unmet Needs in DLBCL • Despite the promise of novel therapies in DLBCL, unmet needs persist . • MT - 601 has demonstrated exceptional safety and preliminary efficacy and carries the potential to fill many of these unmet needs. 26
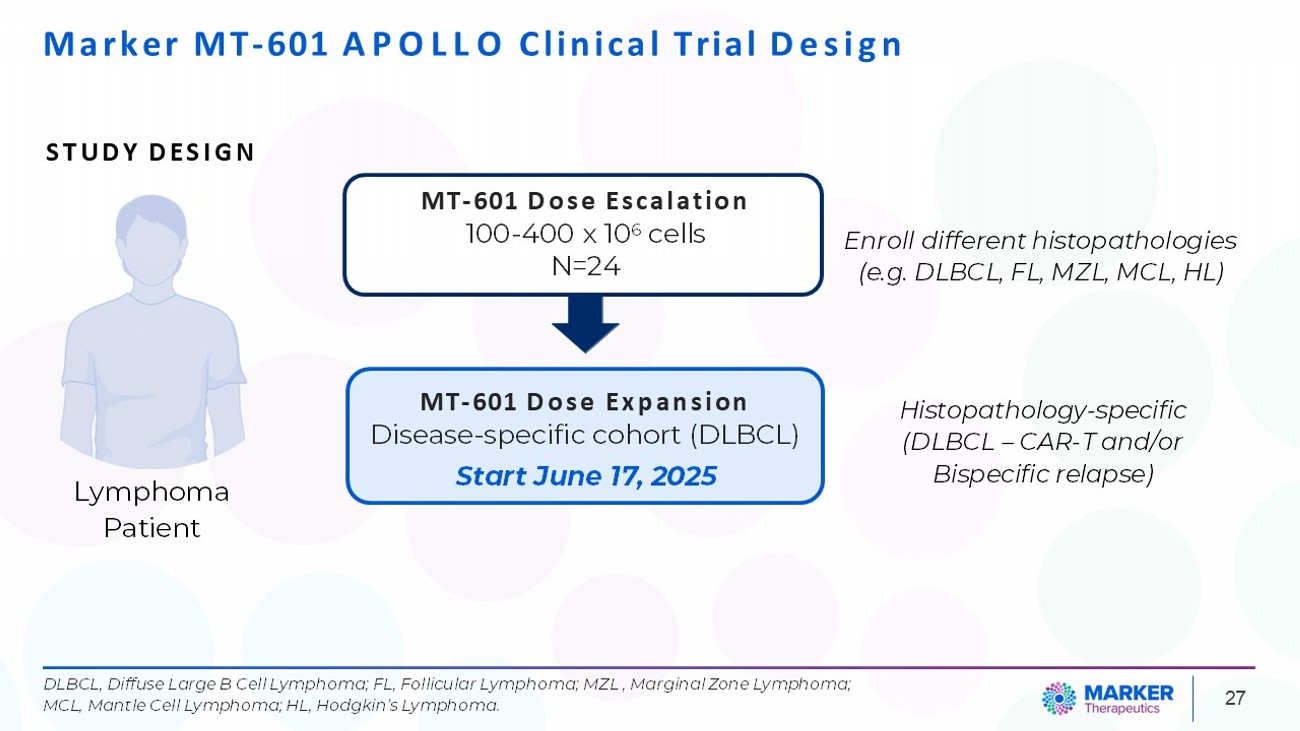
Marker MT - 601 APOLLO Clinical Trial Design Lymphoma Patient 27 MT - 601 Dose Escalation 100 - 400 x 10 6 cells N=24 STUDY DESIGN Enroll different histopathologies (e.g. DLBCL, FL, MZL, MCL, HL) Histopathology - specific (DLBCL – CAR - T and/or Bispecific relapse) DLBCL, Diffuse Large B Cell Lymphoma; FL, Follicular Lymphoma; MZL , Marginal Zone Lymphoma; MCL, Mantle Cell Lymphoma; HL, Hodgkin’s Lymphoma. MT - 601 Dose Expansion Disease - specific cohort (DLBCL) Start June 17, 2025
THANK YOU 28