Exhibit 99.1
NVESTOR DE I CK INVESTOR DECK INVESTOR DECK Preliminary Data from Phase 1 Trial
of RP-A601 May 2025 ©2025 Rocket Pharmaceuticals, Ltd. All rights reserved
FORWARD LOOKING STATEMENT AND DISCLOSURES Various statements in this presentation
concerning Rocket’s future expectations, plans and prospects that involve risks and uncertainties, as well as assumptions that, if they do not materialize or prove incorrect, could cause our results to differ materially from those expressed or
implied by such forward-looking statements. We make such forward- looking statements pursuant to the safe harbor provisions of the Private Securities Litigation Reform Act of 1995 and other federal securities laws. All statements other than
statements of historical facts contained in this release are forward-looking statements. You should not place reliance on these forward-looking statements, which often include words such as "believe," "expect," "anticipate," "intend," "plan,"
"will give," "estimate," "seek," "will," "may," "suggest" or similar terms, variations of such terms or the negative of those terms. These forward-looking statements include, but are not limited to, statements concerning Rocket’s expectations
regarding the safety and effectiveness of product candidates that Rocket is developing to treat Fanconi Anemia (FA), Leukocyte Adhesion Deficiency-I (LAD-I), Pyruvate Kinase Deficiency (PKD), Danon Disease (DD) and other diseases, the expected
timing and data readouts of Rocket’s ongoing and planned clinical trials, the expected timing and outcome of Rocket’s regulatory interactions and planned submissions, Rocket’s plans for the advancement of its DD program, including its planned
pivotal trial, and the safety, effectiveness and timing of related pre- clinical studies and clinical trials, Rocket’s ability to establish key collaborations and vendor relationships for its product candidates, Rocket’s ability to develop
sales and marketing capabilities or enter into agreements with third parties to sell and market its product candidates and Rocket’s ability to expand its pipeline to target additional indications that are compatible with its gene therapy
technologies. Although Rocket believes that the expectations reflected in the forward-looking statements are reasonable, Rocket cannot guarantee such outcomes. Actual results may differ materially from those indicated by these forward-looking
statements as a result of various important factors, including, without limitation, Rocket’s dependence on third parties for development, manufacture, marketing, sales and distribution of product candidates, the outcome of litigation,
unexpected expenditures, Rocket’s competitors’ activities, including decisions as to the timing of competing product launches, pricing and discounting, Rocket’s ability to develop, acquire and advance product candidates into, enroll a
sufficient number of patients into, and successfully complete, clinical studies, Rocket’s ability to acquire additional businesses, form strategic alliances or create joint ventures and its ability to realize the benefit of such acquisitions,
alliances or joint ventures, Rocket’s ability to obtain and enforce patents to protect its product candidates, and its ability to successfully defend against unforeseen third-party infringement claims, as well as those risks more fully
discussed in the section entitled "Risk Factors" in Rocket’s Annual Report on Form 10-K for the year ended December 31, 2024, filed February 27, 2025 with the SEC and subsequent filings with the SEC including our Quarterly Reports on Form 10-Q.
Accordingly, you should not place undue reliance on these forward-looking statements. All such statements speak only as of the date made, and Rocket undertakes no obligation to update or revise publicly any forward-looking statements, whether
as a result of new information, future events or otherwise. 2
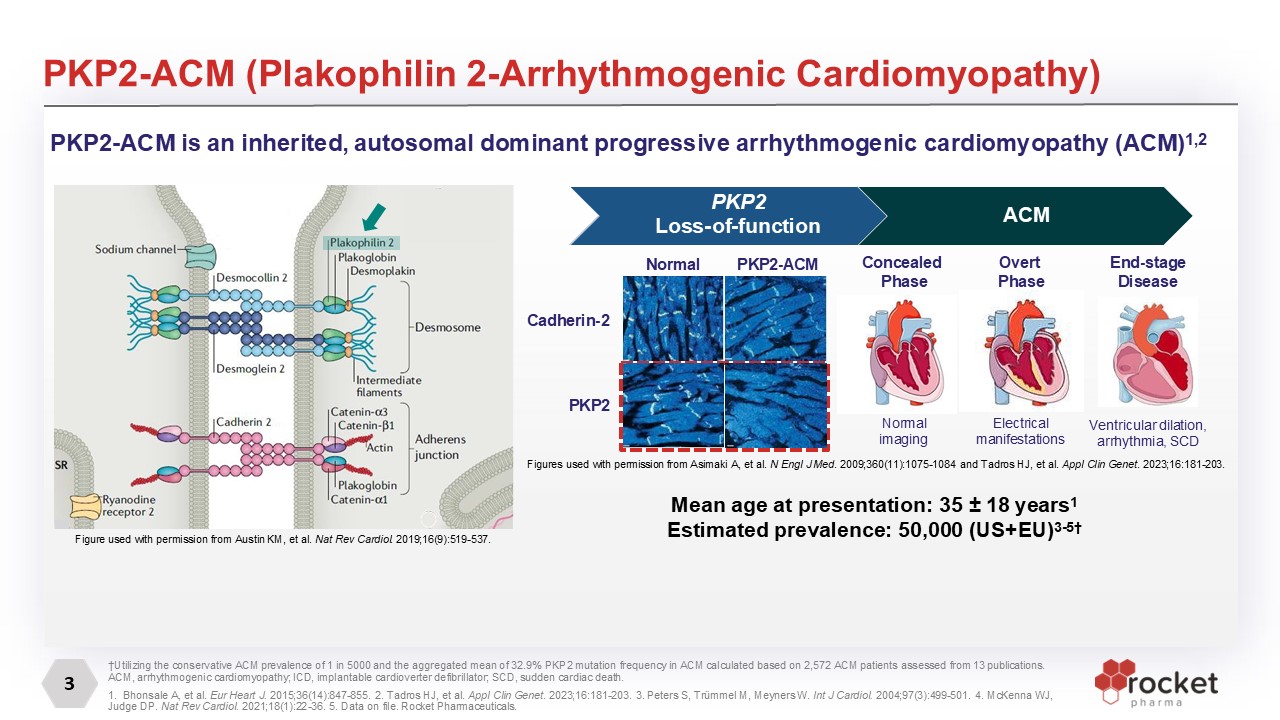
3 PKP2-ACM (Plakophilin 2-Arrhythmogenic Cardiomyopathy) Mean age at
presentation: 35 ± 18 years1 Estimated prevalence: 50,000 (US+EU)3-5† †Utilizing the conservative ACM prevalence of 1 in 5000 and the aggregated mean of 32.9% PKP2 mutation frequency in ACM calculated based on 2,572 ACM patients assessed from
13 publications. ACM, arrhythmogenic cardiomyopathy; ICD, implantable cardioverter defibrillator; SCD, sudden cardiac death. 1. Bhonsale A, et al. Eur Heart J. 2015;36(14):847-855. 2. Tadros HJ, et al. Appl Clin Genet. 2023;16:181-203. 3.
Peters S, Trümmel M, Meyners W. Int J Cardiol. 2004;97(3):499-501. 4. McKenna WJ, Judge DP. Nat Rev Cardiol. 2021;18(1):22-36. 5. Data on file. Rocket Pharmaceuticals. PKP2 Loss-of-function Normal PKP2-ACM ACM PKP2-ACM is an inherited,
autosomal dominant progressive arrhythmogenic cardiomyopathy (ACM)1,2 Cadherin-2 PKP2 Concealed Phase Overt Phase End-stage Disease Normal imaging Electrical manifestations Ventricular dilation, arrhythmia, SCD Figure used with
permission from Austin KM, et al. Nat Rev Cardiol. 2019;16(9):519-537. Figures used with permission from Asimaki A, et al. N Engl J Med. 2009;360(11):1075-1084 and Tadros HJ, et al. Appl Clin Genet. 2023;16:181-203.
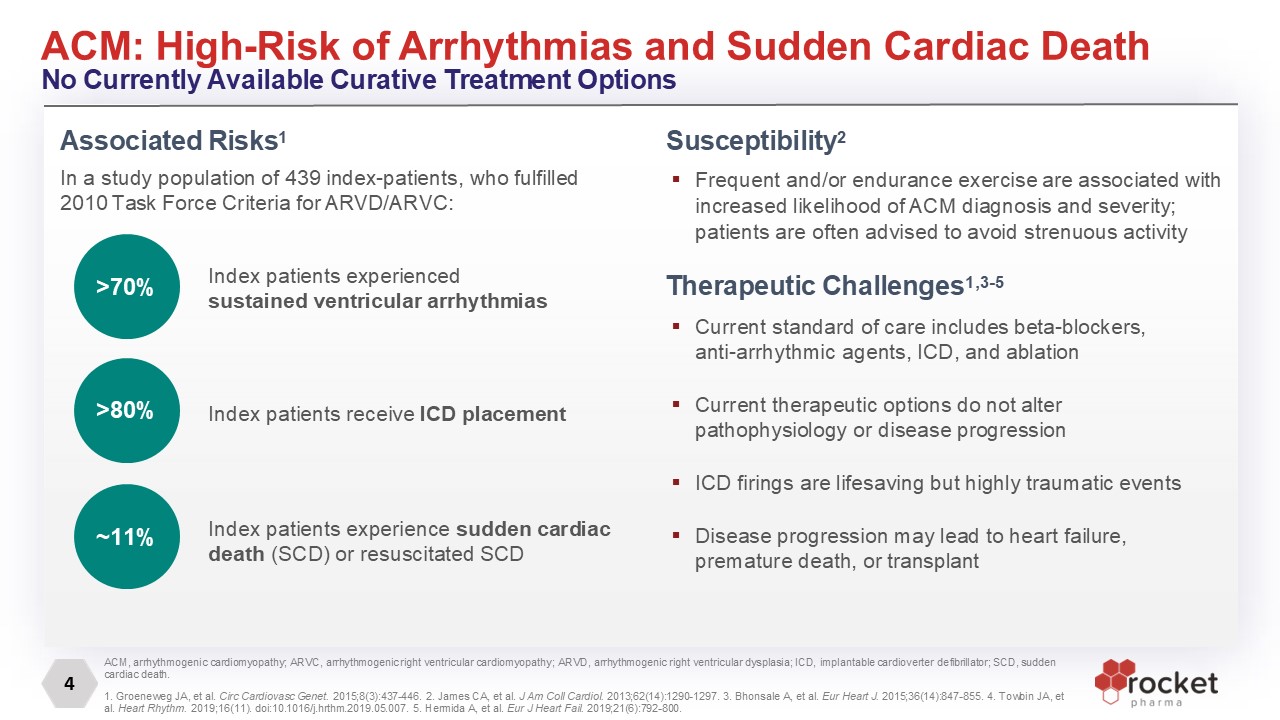
4 ACM: High-Risk of Arrhythmias and Sudden Cardiac Death No Currently Available
Curative Treatment Options ACM, arrhythmogenic cardiomyopathy; ARVC, arrhythmogenic right ventricular cardiomyopathy; ARVD, arrhythmogenic right ventricular dysplasia; ICD, implantable cardioverter defibrillator; SCD, sudden cardiac death. 1.
Groeneweg JA, et al. Circ Cardiovasc Genet. 2015;8(3):437-446. 2. James CA, et al. J Am Coll Cardiol. 2013;62(14):1290-1297. 3. Bhonsale A, et al. Eur Heart J. 2015;36(14):847-855. 4. Towbin JA, et al. Heart Rhythm. 2019;16(11).
doi:10.1016/j.hrthm.2019.05.007. 5. Hermida A, et al. Eur J Heart Fail. 2019;21(6):792-800. Associated Risks1 In a study population of 439 index-patients, who fulfilled 2010 Task Force Criteria for ARVD/ARVC: Index patients
experienced sustained ventricular arrhythmias Index patients experience sudden cardiac death (SCD) or resuscitated SCD >70% ~11% Index patients receive ICD placement >80% Therapeutic Challenges1,3-5 Current standard of care
includes beta-blockers, anti-arrhythmic agents, ICD, and ablation Current therapeutic options do not alter pathophysiology or disease progression ICD firings are lifesaving but highly traumatic events Disease progression may lead to heart
failure, premature death, or transplant Susceptibility2 Frequent and/or endurance exercise are associated with increased likelihood of ACM diagnosis and severity; patients are often advised to avoid strenuous activity
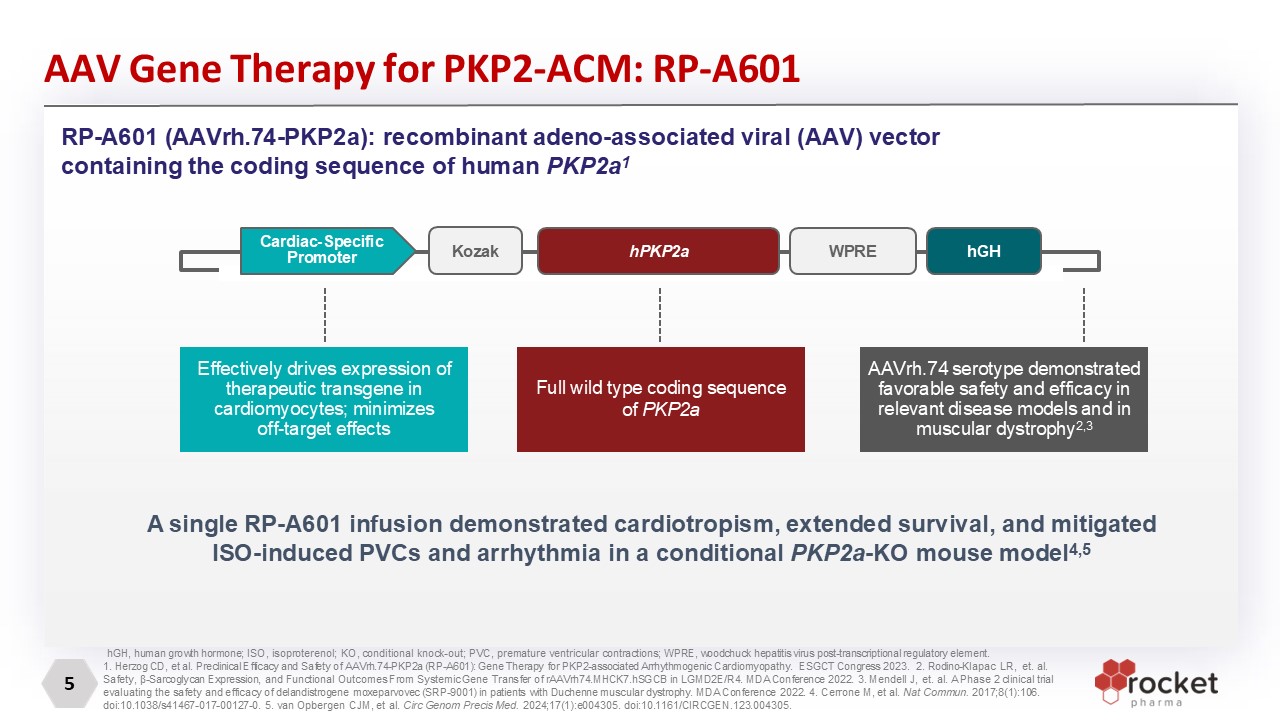
5 AAV Gene Therapy for PKP2-ACM: RP-A601 hGH, human growth hormone; ISO,
isoproterenol; KO, conditional knock-out; PVC, premature ventricular contractions; WPRE, woodchuck hepatitis virus post-transcriptional regulatory element. 1. Herzog CD, et al. Preclinical Efficacy and Safety of AAVrh.74-PKP2a (RP-A601): Gene
Therapy for PKP2-associated Arrhythmogenic Cardiomyopathy. ESGCT Congress 2023. 2. Rodino-Klapac LR, et. al. Safety, β-Sarcoglycan Expression, and Functional Outcomes From Systemic Gene Transfer of rAAVrh74.MHCK7.hSGCB in LGMD2E/R4. MDA
Conference 2022. 3. Mendell J, et. al. A Phase 2 clinical trial evaluating the safety and efficacy of delandistrogene moxeparvovec (SRP-9001) in patients with Duchenne muscular dystrophy. MDA Conference 2022. 4. Cerrone M, et al. Nat Commun.
2017;8(1):106. doi:10.1038/s41467-017-00127-0. 5. van Opbergen CJM, et al. Circ Genom Precis Med. 2024;17(1):e004305. doi:10.1161/CIRCGEN.123.004305. RP-A601 (AAVrh.74-PKP2a): recombinant adeno-associated viral (AAV) vector containing the
coding sequence of human PKP2a1 Effectively drives expression of therapeutic transgene in cardiomyocytes; minimizes off-target effects Full wild type coding sequence of PKP2a AAVrh.74 serotype demonstrated favorable safety and efficacy in
relevant disease models and in muscular dystrophy2,3 A single RP-A601 infusion demonstrated cardiotropism, extended survival, and mitigated ISO-induced PVCs and arrhythmia in a conditional PKP2a-KO mouse
model4,5 hPKP2a Kozak WPRE hGH Cardiac-Specific Promoter
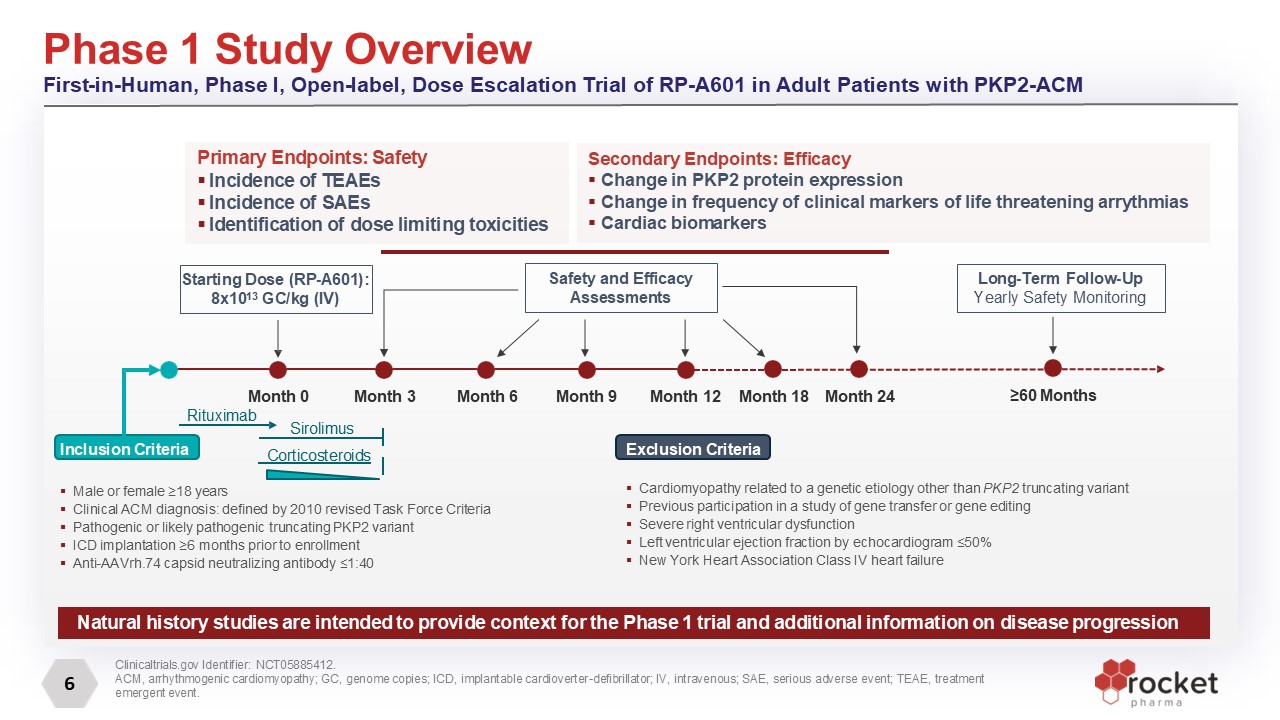
6 Phase 1 Study Overview First-in-Human, Phase I, Open-label, Dose Escalation
Trial of RP-A601 in Adult Patients with PKP2-ACM Clinicaltrials.gov Identifier: NCT05885412. ACM, arrhythmogenic cardiomyopathy; GC, genome copies; ICD, implantable cardioverter-defibrillator; IV, intravenous; SAE, serious adverse event;
TEAE, treatment emergent event. Inclusion Criteria Male or female ≥18 years Clinical ACM diagnosis: defined by 2010 revised Task Force Criteria Pathogenic or likely pathogenic truncating PKP2 variant ICD implantation ≥6 months prior to
enrollment Anti-AAVrh.74 capsid neutralizing antibody ≤1:40 Exclusion Criteria Cardiomyopathy related to a genetic etiology other than PKP2 truncating variant Previous participation in a study of gene transfer or gene editing Severe right
ventricular dysfunction Left ventricular ejection fraction by echocardiogram ≤50% New York Heart Association Class IV heart failure Starting Dose (RP-A601): 8x1013 GC/kg (IV) Month 3 Month 12 Long-Term Follow-Up Yearly Safety
Monitoring Month 6 Month 9 Rituximab Sirolimus Safety and Efficacy Assessments Primary Endpoints: Safety Incidence of TEAEs Incidence of SAEs Identification of dose limiting toxicities Month 0 Corticosteroids Month 18 Month
24 ≥60 Months Secondary Endpoints: Efficacy Change in PKP2 protein expression Change in frequency of clinical markers of life threatening arrythmias Cardiac biomarkers Natural history studies are intended to provide context for the Phase
1 trial and additional information on disease progression
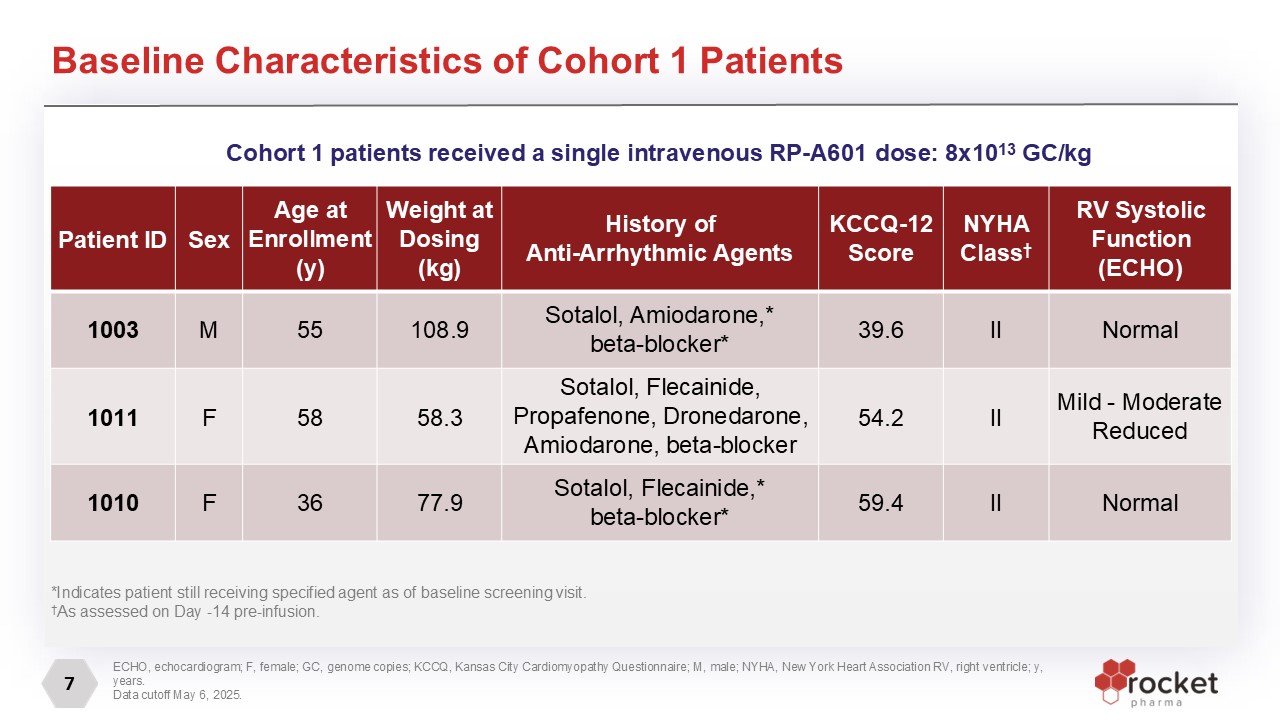
7 Baseline Characteristics of Cohort 1 Patients *Indicates patient still
receiving specified agent as of baseline screening visit. †As assessed on Day -14 pre-infusion. Patient ID Sex Age at Enrollment (y) Weight at Dosing (kg) History of Anti-Arrhythmic Agents KCCQ-12 Score NYHA Class† RV Systolic
Function (ECHO) 1003 M 55 108.9 Sotalol, Amiodarone,* beta-blocker* 39.6 II Normal 1011 F 58 58.3 Sotalol, Flecainide, Propafenone, Dronedarone, Amiodarone, beta-blocker 54.2 II Mild - Moderate
Reduced 1010 F 36 77.9 Sotalol, Flecainide,* beta-blocker* 59.4 II Normal Cohort 1 patients received a single intravenous RP-A601 dose: 8x1013 GC/kg ECHO, echocardiogram; F, female; GC, genome copies; KCCQ, Kansas City Cardiomyopathy
Questionnaire; M, male; NYHA, New York Heart Association RV, right ventricle; y, years. Data cutoff May 6, 2025.
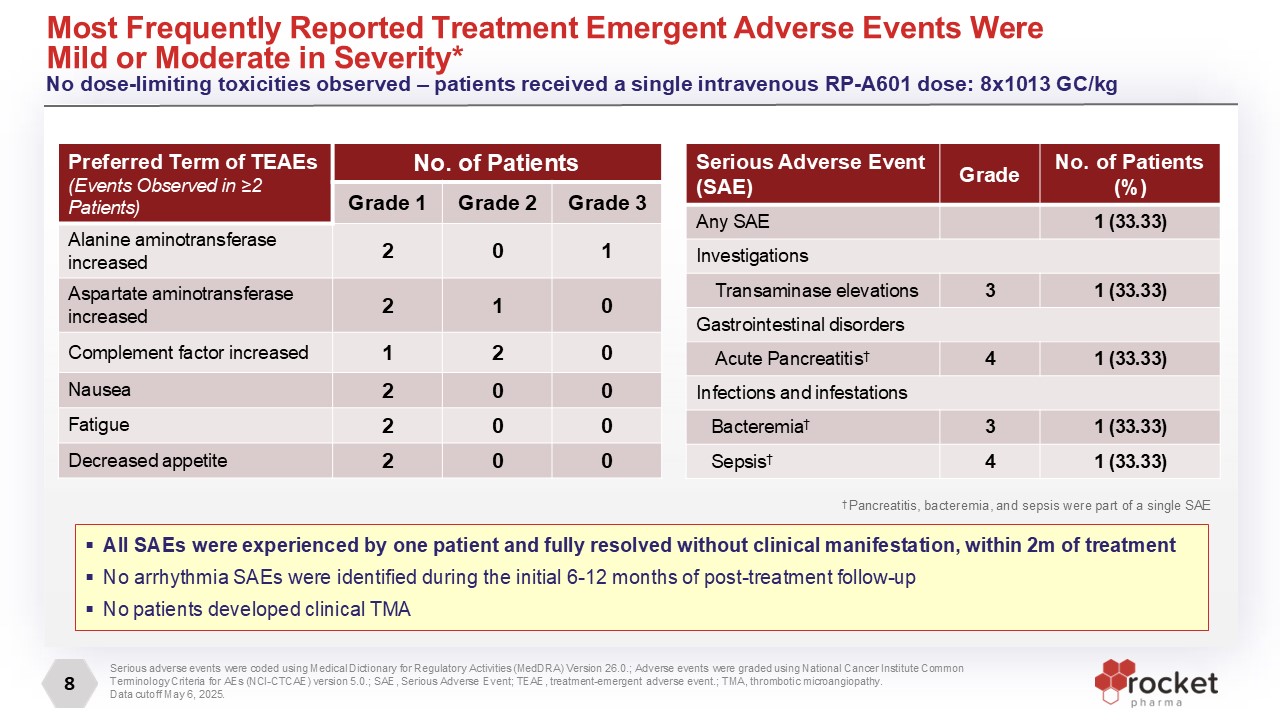
8 Most Frequently Reported Treatment Emergent Adverse Events Were Mild or
Moderate in Severity* No dose-limiting toxicities observed – patients received a single intravenous RP-A601 dose: 8x1013 GC/kg † Pancreatitis, bacteremia, and sepsis were part of a single SAE Serious adverse events were coded using Medical
Dictionary for Regulatory Activities (MedDRA) Version 26.0.; Adverse events were graded using National Cancer Institute Common Terminology Criteria for AEs (NCI-CTCAE) version 5.0.; SAE, Serious Adverse Event; TEAE, treatment-emergent adverse
event.; TMA, thrombotic microangiopathy. Data cutoff May 6, 2025. All SAEs were experienced by one patient and fully resolved without clinical manifestation, within 2m of treatment No arrhythmia SAEs were identified during the initial 6-12
months of post-treatment follow-up No patients developed clinical TMA Serious Adverse Event (SAE) Grade No. of Patients (%) Any SAE 1 (33.33) Investigations Transaminase elevations 3 1 (33.33) Gastrointestinal disorders Acute
Pancreatitis† 4 1 (33.33) Infections and infestations Bacteremia† 3 1 (33.33) Sepsis† 4 1 (33.33) Preferred Term of TEAEs (Events Observed in ≥2 Patients) No. of Patients Grade 1 Grade 2 Grade 3 Alanine aminotransferase
increased 2 0 1 Aspartate aminotransferase increased 2 1 0 Complement factor increased 1 2 0 Nausea 2 0 0 Fatigue 2 0 0 Decreased appetite 2 0 0
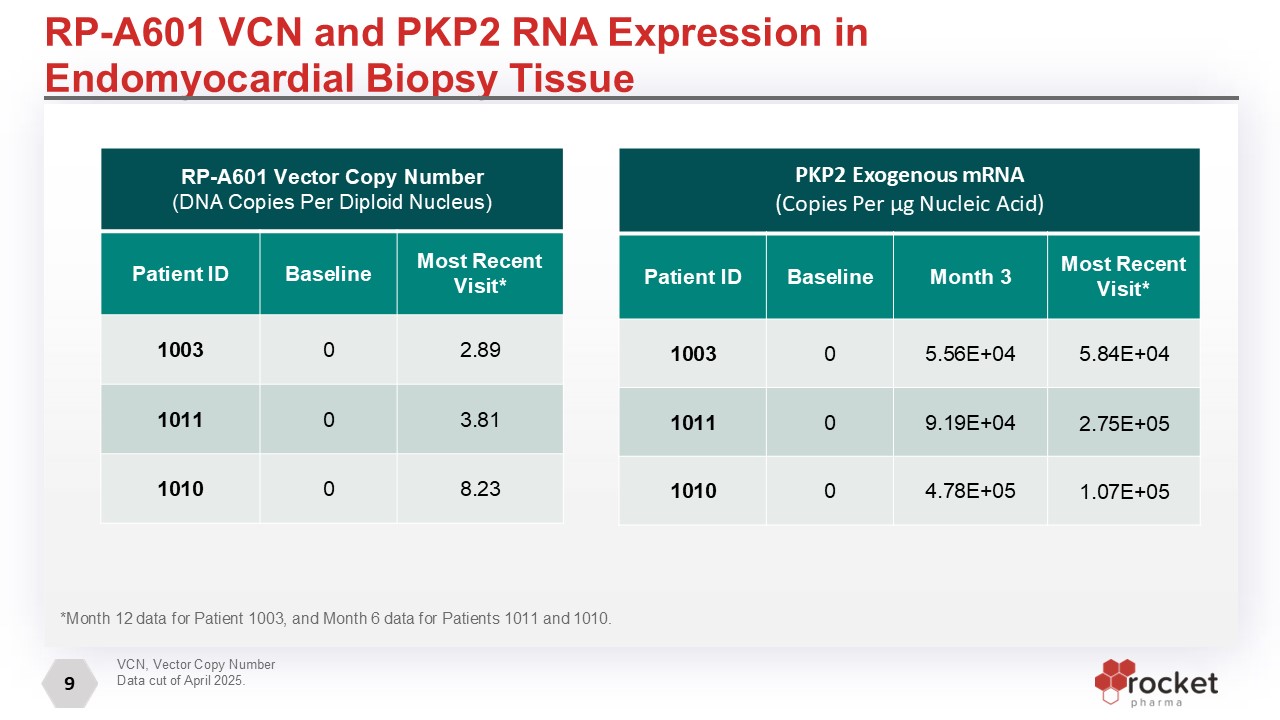
9 *Month 12 data for Patient 1003, and Month 6 data for Patients 1011 and
1010. RP-A601 VCN and PKP2 RNA Expression in Endomyocardial Biopsy Tissue RP-A601 Vector Copy Number (DNA Copies Per Diploid Nucleus) Patient ID Baseline Most Recent Visit* 1003 0 2.89 1011 0 3.81 1010 0 8.23 PKP2 Exogenous
mRNA (Copies Per μg Nucleic Acid) Patient ID Baseline Month 3 Most Recent Visit* 1003 0 5.56E+04 5.84E+04 1011 0 9.19E+04 2.75E+05 1010 0 4.78E+05 1.07E+05 VCN, Vector Copy Number Data cut of April 2025.
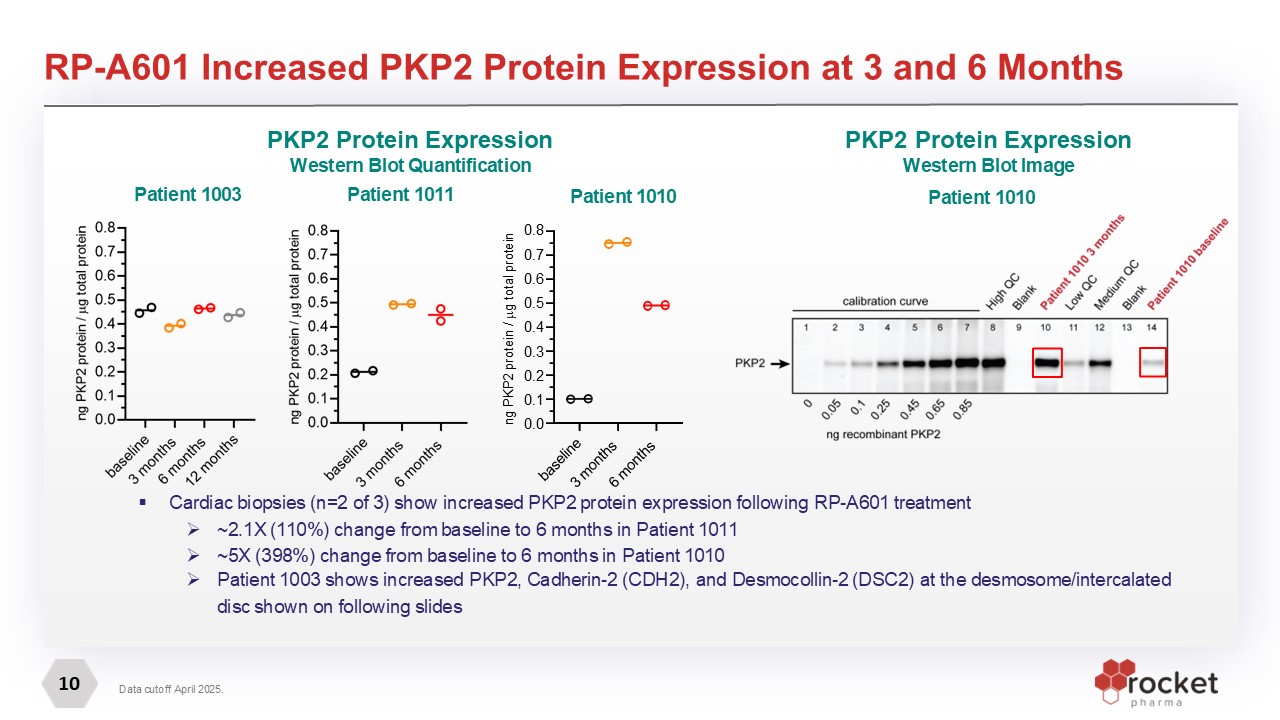
10 RP-A601 Increased PKP2 Protein Expression at 3 and 6 Months Cardiac biopsies
(n=2 of 3) show increased PKP2 protein expression following RP-A601 treatment ~2.1X (110%) change from baseline to 6 months in Patient 1011 ~5X (398%) change from baseline to 6 months in Patient 1010 Patient 1003 shows increased PKP2,
Cadherin-2 (CDH2), and Desmocollin-2 (DSC2) at the desmosome/intercalated disc shown on following slides Data cutoff April 2025. Patient 1010 Patient 1003 PKP2 Protein Expression Western Blot Quantification Patient 1011 PKP2 Protein
Expression Western Blot Image Patient 1010 baseline 3 months 6 months 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0 ng PKP2 protein / g total protein
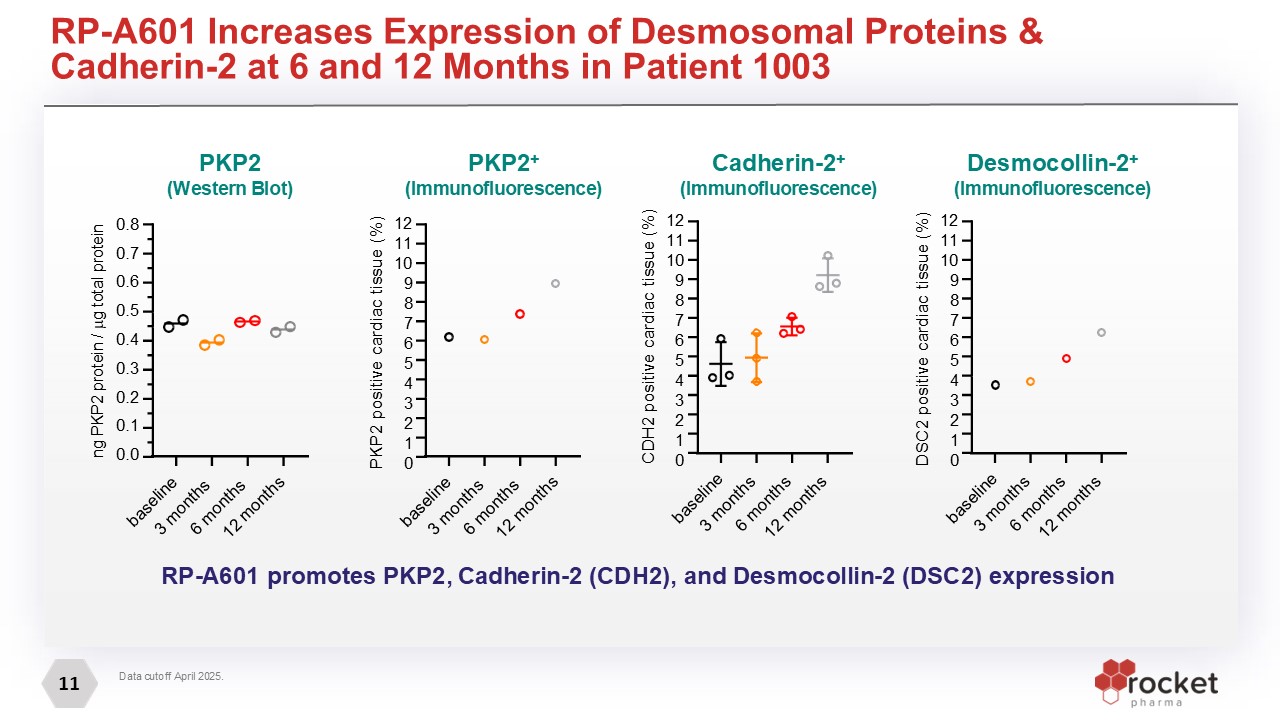
11 Data cutoff April 2025. RP-A601 Increases Expression of Desmosomal Proteins
& Cadherin-2 at 6 and 12 Months in Patient 1003 baseline 3 months 6 months 12 months 12 11 10 9 8 7 6 5 4 3 2 1 0 CDH2 positive cardiac tissue (%) baseline 3 months 6 months 12
months 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0 ng PKP2 protein / g total protein baseline 3 months 6 months 12 months 12 11 10 9 8 7 6 5 4 3 2 1 0 PKP2 positive cardiac tissue (%) baseline 3 months 6 months 12
months 12 11 10 9 8 7 6 5 4 3 2 1 0 DSC2 positive cardiac tissue (%) RP-A601 promotes PKP2, Cadherin-2 (CDH2), and Desmocollin-2 (DSC2)
expression Cadherin-2+ (Immunofluorescence) Desmocollin-2+ (Immunofluorescence) PKP2+ (Immunofluorescence) PKP2 (Western Blot)
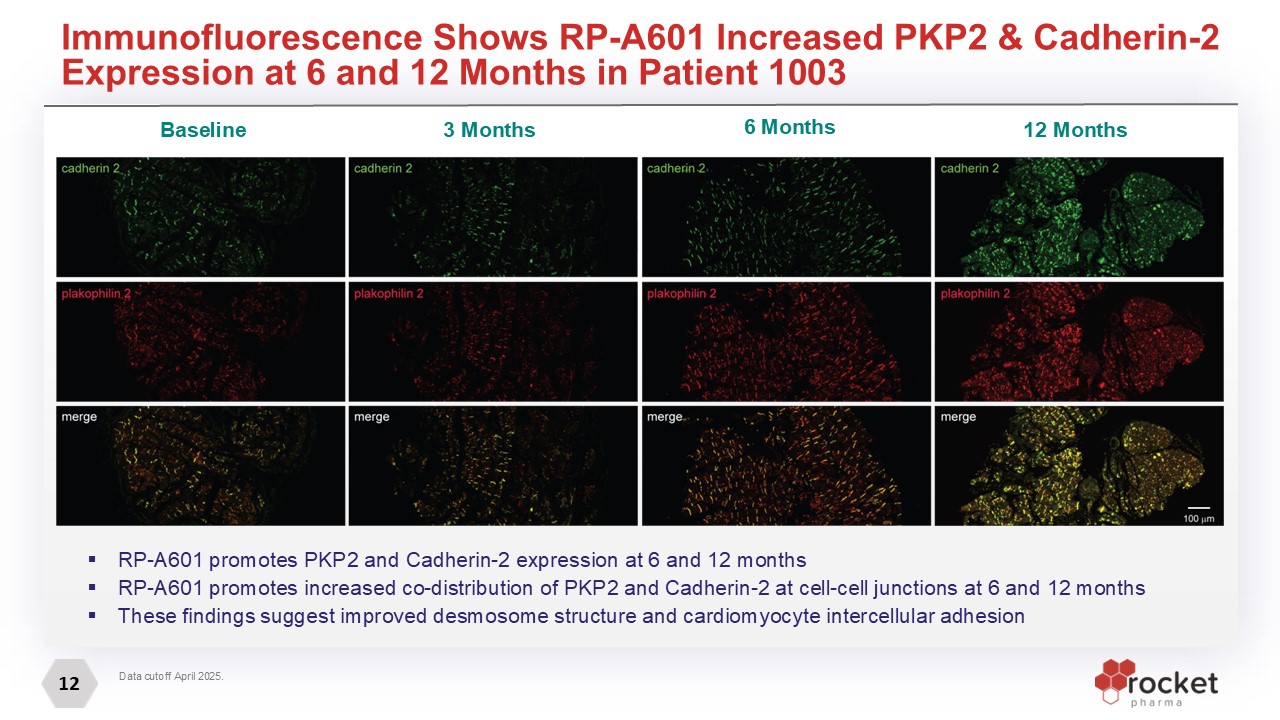
12 Data cutoff April 2025. Immunofluorescence Shows RP-A601 Increased PKP2 &
Cadherin-2 Expression at 6 and 12 Months in Patient 1003 RP-A601 promotes PKP2 and Cadherin-2 expression at 6 and 12 months RP-A601 promotes increased co-distribution of PKP2 and Cadherin-2 at cell-cell junctions at 6 and 12 months These
findings suggest improved desmosome structure and cardiomyocyte intercellular adhesion Baseline 3 Months 6 Months 12 Months
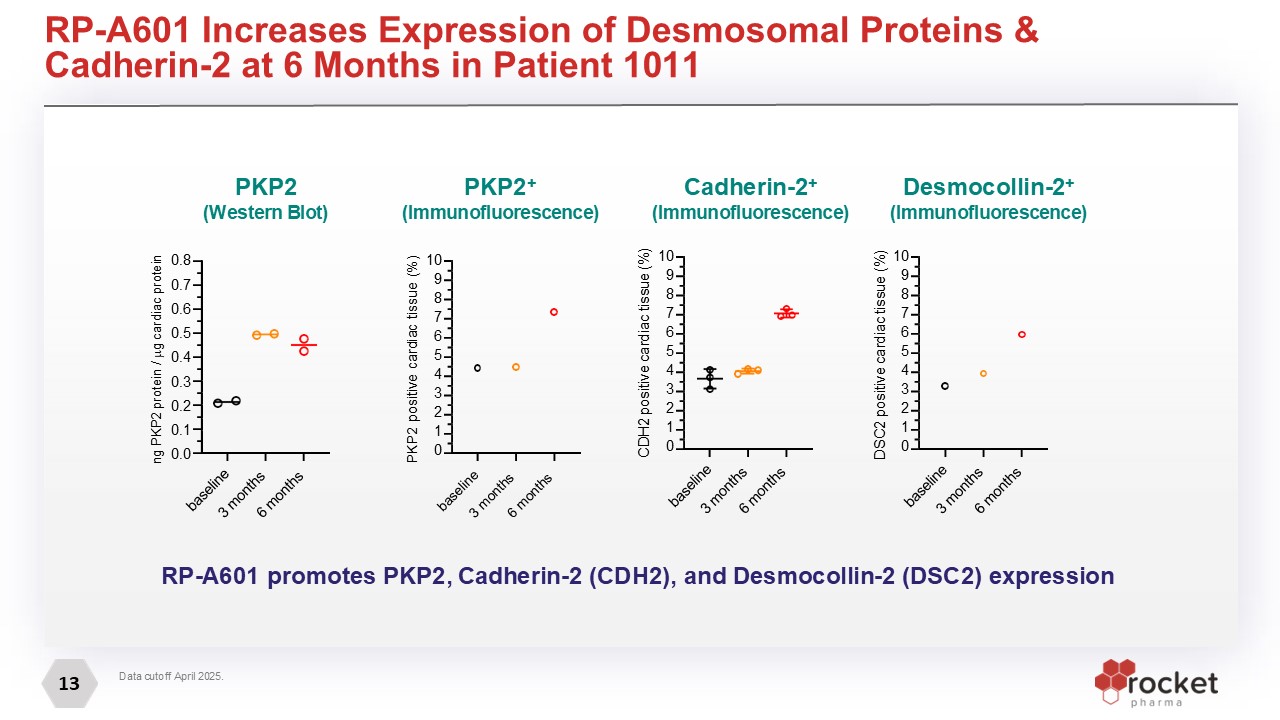
13 Data cutoff April 2025. RP-A601 Increases Expression of Desmosomal Proteins
& Cadherin-2 at 6 Months in Patient 1011 baseline 3 months 6 months 10 9 8 7 6 5 4 3 2 1 0 DSC2 positive cardiac tissue (%) baseline 3 months 6 months 10 9 8 7 6 5 4 3 2 1 0 CDH2 positive cardiac tissue
(%) baseline 3 months 6 months 10 9 8 7 6 5 4 3 2 1 0 PKP2 positive cardiac tissue (%) baseline 3 months 6 months 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0 ng PKP2 protein / g cardiac
protein Cadherin-2+ (Immunofluorescence) Desmocollin-2+ (Immunofluorescence) PKP2+ (Immunofluorescence) PKP2 (Western Blot) RP-A601 promotes PKP2, Cadherin-2 (CDH2), and Desmocollin-2 (DSC2) expression
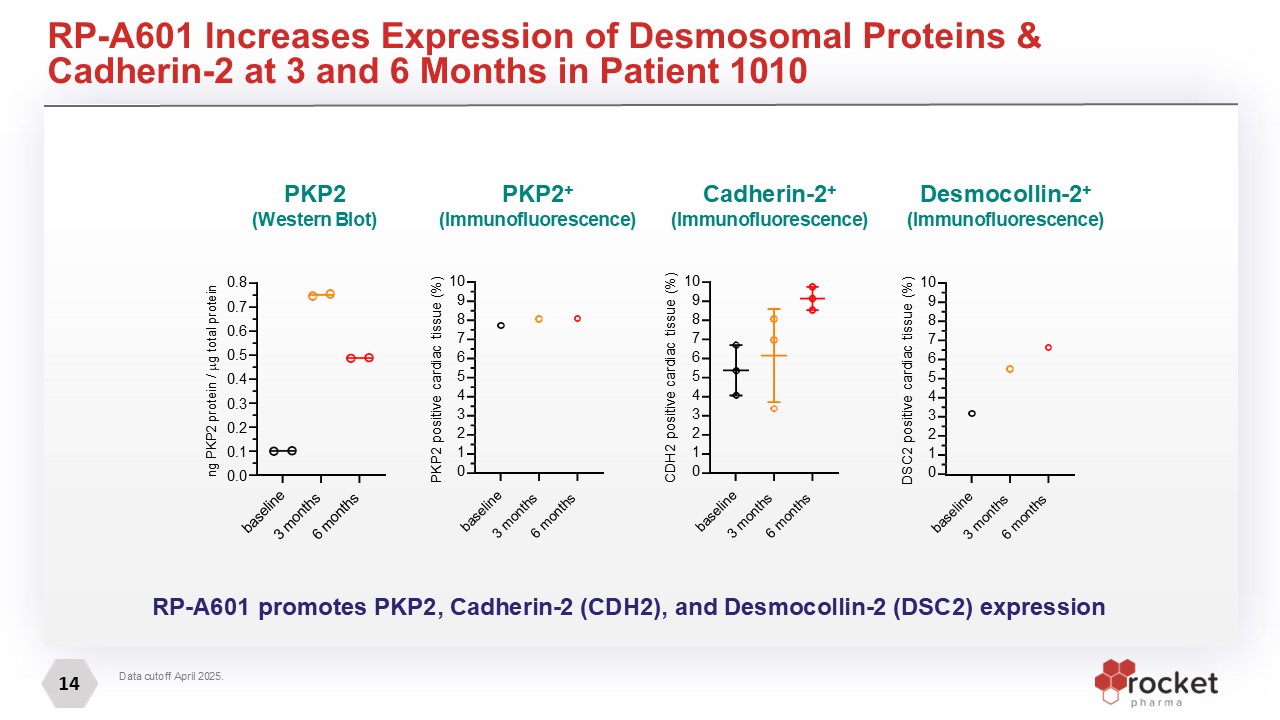
14 Data cutoff April 2025. RP-A601 Increases Expression of Desmosomal Proteins
& Cadherin-2 at 3 and 6 Months in Patient 1010 baseline 3 months 6 months 10 9 8 7 6 5 4 3 2 1 0 PKP2 positive cardiac tissue (%) baseline 3 months 6 months 10 9 8 7 6 5 4 3 2 1 0 CDH2 positive cardiac tissue
(%) baseline 3 months 6 months 10 9 8 7 6 5 4 3 2 1 0 DSC2 positive cardiac tissue (%) baseline 3 months 6 months 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0 ng PKP2 protein / g total
protein Cadherin-2+ (Immunofluorescence) Desmocollin-2+ (Immunofluorescence) PKP2+ (Immunofluorescence) PKP2 (Western Blot) RP-A601 promotes PKP2, Cadherin-2 (CDH2), and Desmocollin-2 (DSC2) expression
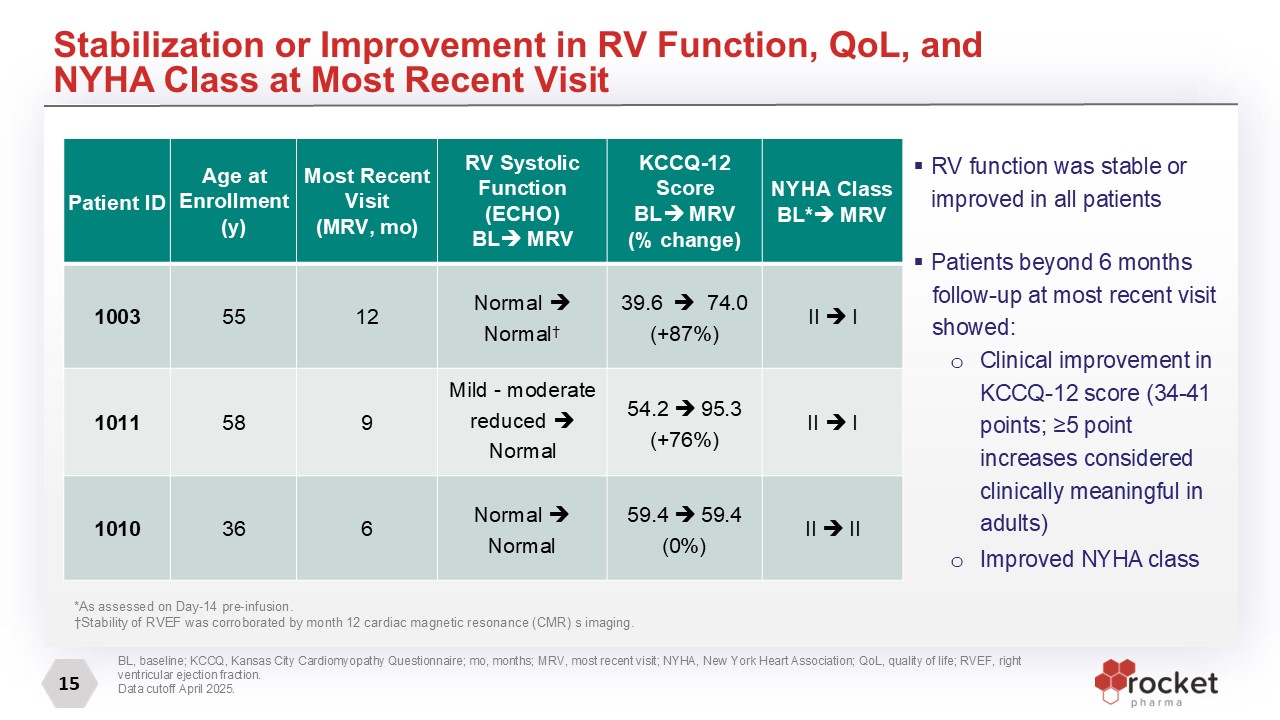
15 Stabilization or Improvement in RV Function, QoL, and NYHA Class at Most
Recent Visit Patient ID Age at Enrollment (y) Most Recent Visit (MRV, mo) RV Systolic Function (ECHO) BL MRV KCCQ-12 Score BL MRV (% change) NYHA Class BL* MRV 1003 55 12 Normal Normal† 39.6 74.0 (+87%) II
I 1011 58 9 Mild - moderate reduced Normal 54.2 95.3 (+76%) II I 1010 36 6 Normal Normal 59.4 59.4 (0%) II II RV function was stable or improved in all patients Patients beyond 6 months follow-up at most recent
visit showed: Clinical improvement in KCCQ-12 score (34-41 points; ≥5 point increases considered clinically meaningful in adults) Improved NYHA class BL, baseline; KCCQ, Kansas City Cardiomyopathy Questionnaire; mo, months; MRV, most recent
visit; NYHA, New York Heart Association; QoL, quality of life; RVEF, right ventricular ejection fraction. Data cutoff April 2025. *As assessed on Day-14 pre-infusion. †Stability of RVEF was corroborated by month 12 cardiac magnetic resonance
(CMR) s imaging.
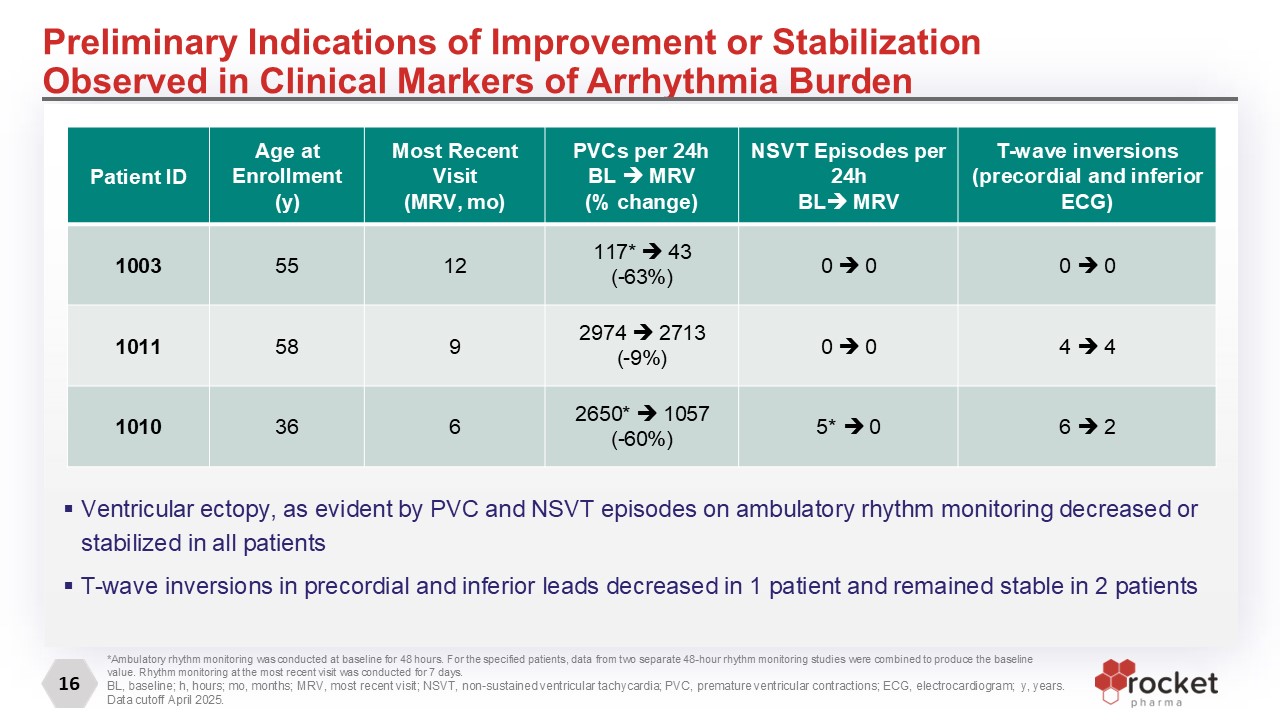
16 Preliminary Indications of Improvement or Stabilization Observed in Clinical
Markers of Arrhythmia Burden Patient ID Age at Enrollment (y) Most Recent Visit (MRV, mo) PVCs per 24h BL MRV (% change) NSVT Episodes per 24h BL MRV T-wave inversions (precordial and inferior ECG) 1003 55 12 117*
43 (-63%) 0 0 0 0 1011 58 9 2974 2713 (-9%) 0 0 4 4 1010 36 6 2650* 1057 (-60%) 5* 0 6 2 Ventricular ectopy, as evident by PVC and NSVT episodes on ambulatory rhythm monitoring decreased or stabilized in all
patients T-wave inversions in precordial and inferior leads decreased in 1 patient and remained stable in 2 patients *Ambulatory rhythm monitoring was conducted at baseline for 48 hours. For the specified patients, data from two separate
48-hour rhythm monitoring studies were combined to produce the baseline value. Rhythm monitoring at the most recent visit was conducted for 7 days. BL, baseline; h, hours; mo, months; MRV, most recent visit; NSVT, non-sustained ventricular
tachycardia; PVC, premature ventricular contractions; ECG, electrocardiogram; y, years. Data cutoff April 2025.
Summary of Initial Results From Ongoing Phase I Trial Cohort 1 Patients with
PKP2-ACM Treated with RP-A601 Demonstrated RP-A601 was generally well-tolerated with no dose-limiting toxicities observed No TMA or ventricular arrhythmias were observed Increased expression and desmosomal localization of PKP2,
Desmocollin-2, and Cadherin-2 in all patients Most evident at ≥ 6 months post-treatment of RP-A601 Preliminary indications of improvement or stabilization observed in arrhythmia burden, heart function, and quality of
life Decreased/stabilized ventricular ectopy (PVC, NSVT) on rhythm monitoring in all patients Decreased/stabilized T-wave inversions on ECG in all patients Improved/stabilized RV function Improved quality-of-life and NYHA Class in patients
followed beyond 6 months ECG, electrocardiogram; NSVT, non-sustained ventricular tachycardia; NYHA, New York Heart Association Functional classification; PVC, premature ventricular contractions; RV, right ventricular; 17 TMA, thrombotic
microangiopathy
Key Findings and Path Forward Key Findings RP-A601 was generally well tolerated
in all 3 patients SAEs were reversible without clinical manifestations, no dose-limiting toxicities observed All 3 patients in Cohort 1 demonstrated cardiac transduction with localized myocardial protein expression that was maintained or
increased up to 12-months post-infusion Initial efficacy in all patients showed early signs of disease modification across multiple clinical parameters with up to 12-months of follow-up Based on the Phase 1 trial, 8.0e13 GC/kg considered
final dose Path Forward Phase 1 (NCT05885412) is a dose-finding trial to evaluate the safety of RP-A601 With no further dose escalation, Rocket plans to design and execute a potential pivotal trial to further evaluate the efficacy and safety
of RP-A601 18

19 ©2024 Rocket Pharmaceuticals, Ltd. All rights reserved Thank You
