false
0001359931
0001359931
2025-04-26
2025-04-26
iso4217:USD
xbrli:shares
iso4217:USD
xbrli:shares
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d)
of the Securities Exchange Act of 1934
Date of Report (Date of earliest event reported):
April 26, 2025
Protara Therapeutics, Inc.
(Exact name of registrant as specified in its
charter)
| Delaware |
|
001-36694 |
|
20-4580525 |
(State or other jurisdiction of
incorporation) |
|
(Commission File No.) |
|
(IRS Employer
Identification No.) |
|
345 Park Avenue South
Third Floor
New York, NY |
|
10010 |
| (Address of principal executive offices) |
|
(Zip Code) |
Registrant’s telephone number, including
area code: (646) 844-0337
N/A
(Former name or former address, if changed since
last report.)
Check the appropriate box below if the Form 8-K
filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
| ☐ | Written
communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| ☐ | Soliciting
material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
| ☐ | Pre-commencement
communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| ☐ | Pre-commencement
communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b)
of the Act:
| Title of each class |
|
Trading Symbol(s) |
|
Name of each exchange on which registered |
| Common Stock, par value $0.001 per share |
|
TARA |
|
The Nasdaq Capital Market |
Indicate by check mark whether the registrant
is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§230.405 of this chapter) or Rule 12b-2 of the
Securities Exchange Act of 1934 (§240.12b-2 of this chapter).
Emerging growth company ☐
If an emerging growth company, indicate by check
mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting
standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Item 7.01 Regulation FD Disclosure.
On April 26, 2025, Protara Therapeutics, Inc.
(the “Company” or “Protara”) issued a press release reporting new interim clinical data on the ongoing Phase 2
ADVANCED-2 trial program (the “Press Release”). A copy of the Press Release is furnished herewith as Exhibit 99.1 to this
Current Report on Form 8-K.
On April 28, 2025, the Company also posted an
investor presentation (the “Investor Presentation”) to the “Investors—Events and Presentations” section
of the Company’s website at www.protaratx.com. The Investor Presentation will be used in connection with a conference call and webcast
today, April 28, 2025, at 8:30 am ET, to review the clinical data presented during a poster session at the 2025 American Urological Association
Annual Meeting in Las Vegas, Nevada (the “2025 AUA Conference”) and provides an update on the ongoing Phase 2 ADVANCED-2 trial
program. A copy of the Investor Presentation is furnished herewith as Exhibit 99.2 to this Current Report on Form 8-K.
The information contained in Item 7.01 of this
Current Report on Form 8-K, including Exhibits 99.1 and 99.2 attached hereto, is being furnished and shall not be deemed to be “filed”
for the purposes of Section 18 of the Exchange Act of 1934, as amended (the “Exchange Act”), or otherwise subject to the liabilities
of that section and shall not be incorporated by reference in any filing under the Securities Act of 1933, as amended, or the Exchange
Act, except as shall be expressly set forth by specific reference in such filing.
Item 8.01 Other Events.
On April 26, 2025, the Company presented updated
results from its ongoing Phase 2 open-label ADVANCED-2 trial assessing intravesical TARA-002, the Company’s investigational cell-based
therapy, in high-risk Non-Muscle Invasive Bladder Cancer (NMIBC) patients with carcinoma in situ, or CIS (± Ta/T1), who are Bacillus
Calmette-Guérin (BCG)-Unresponsive or BCG-Naïve, at a poster session at the 2025 AUA Conference. A copy of the poster, which
has been published to the “Investors—Events and Presentations” section of the Company’s website, is filed as Exhibit
99.3 to this Current Report on Form 8-K and is incorporated herein by reference.
BCG-Unresponsive Cohort
The BCG-Unresponsive dataset includes a total
of five patients, all of whom were six- and nine-month evaluable, and three of whom were evaluable at 12 months as of an April 16, 2025
data cutoff. The complete response (CR) rate at any time in BCG-Unresponsive patients was 100% (5/5). The CR rate in BCG-Unresponsive
patients was 100% (5/5) at six months, 80% (4/5) at nine months, and 67% (2/3) at 12 months.
BCG-Naïve Cohort
The BCG-Naïve dataset includes a total of
21 patients, including 16 evaluable at six months, eight at nine months, and seven at 12 months as of an April 16, 2025 data cutoff. The
CR rate at any time in BCG-Naïve patients was 76% (16/21). The CR rate in BCG-Naïve patients was 63% (10/16) at six months,
63% (5/8) at nine months, and 43% (3/7) at 12 months.
Safety
The majority of adverse events were Grade 1 and
transient with no Grade 3 or greater treatment-related adverse events (TRAEs) as assessed by study investigators. No patients discontinued
treatment due to TRAEs. The most common adverse events were in line with typical responses to bacterial immunopotentiation, such as flu-like
symptoms. The most common urinary symptoms reflect urinary tract instrumentation effects, such as bladder spasm, burning sensation, and
urinary tract infection. Most bladder irritations resolved shortly after administration or within a few hours to a few days.
Forward-Looking Statements
Statements contained in this press release regarding
matters that are not historical facts are "forward looking statements" within the meaning of the Private Securities Litigation
Reform Act of 1995. Protara may, in some cases, use terms such as “predicts,” “believes,” “potential,”
“proposed,” “continue,” “designed,” “estimates,” “anticipates,” “expects,”
“plans,” “intends,” “may,” “could,” “might,” “will,” “should”
or other words or expressions referencing future events, conditions or circumstances that convey uncertainty of future events or outcomes
to identify these forward-looking statements. Such forward-looking statements include but are not limited to, statements regarding Protara’s
intentions, beliefs, projections, outlook, analyses or current expectations concerning, among other things: Protara’s business strategy,
including its development plans for its product candidates and plans regarding the timing or outcome of existing or future clinical trials
(including reporting data from approximately 25 6-month evaluable BCG-Unresponsive patients by the end of 2025); statements related to
expectations regarding interactions with the U.S. Food and Drug Administration (FDA); Protara’s financial position; statements regarding
the anticipated safety or efficacy of Protara’s product candidates; and Protara’s outlook for the remainder of the year and
future periods. Because such statements are subject to risks and uncertainties, actual results may differ materially from those expressed
or implied by such forward-looking statements. Factors that contribute to the uncertain nature of the forward-looking statements include:
risks that Protara’s financial guidance may not be as expected, as well as risks and uncertainties associated with: Protara’s
development programs, including the initiation and completion of non-clinical studies and clinical trials and the timing of required filings
with the FDA and other regulatory agencies; general market conditions; changes in the competitive landscape; changes in Protara’s
strategic and commercial plans; Protara’s ability to obtain sufficient financing to fund its strategic plans and commercialization
efforts; having to use cash in ways or on timing other than expected; the impact of market volatility on cash reserves; failure to attract
and retain management and key personnel; the impact of general U.S. and foreign, economic, industry, market, regulatory, political
or public health conditions; and the risks and uncertainties associated with Protara’s business and financial condition in general,
including the risks and uncertainties described more fully under the caption “Risk Factors” and elsewhere in Protara's filings
and reports with the United States Securities and Exchange Commission. All forward-looking statements contained in this press release
speak only as of the date on which they were made and are based on management's assumptions and estimates as of such date. Protara undertakes
no obligation to update any forward-looking statements, whether as a result of the receipt of new information, the occurrence of future
events or otherwise, except as required by law.
Item 9.01 Financial Statements and Exhibits.
(d) Exhibits
SIGNATURES
Pursuant to the requirements
of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto
duly authorized.
Date: April 28, 2025
| |
Protara Therapeutics, Inc. |
| |
|
|
| |
By: |
/s/ Patrick Fabbio |
| |
|
Patrick Fabbio |
| |
|
Chief Financial Officer |
Exhibit 99.1

Protara
Therapeutics Announces Positive Interim Results Demonstrating Durable Responses in the
Ongoing Phase 2 ADVANCED-2 Trial of TARA-002 in
Patients with NMIBC
| ● | TARA-002 demonstrates 100% complete response rate at any time and 67%
12-month landmark complete response rate in BCG-Unresponsive patients |
| ● | TARA-002 demonstrates 76% complete response rate at any time and 43% 12-month
landmark complete response rate in BCG-Naïve patients |
| ● | Favorable safety and tolerability profile with no Grade 3 or greater treatment-related
adverse events |
| ● | On track to present updated interim data from approximately 25 six-month
evaluable BCG-Unresponsive patients by the end of 2025 |
| ● | Company to host conference call and webcast on Monday, April 28, 2025,
at 8:30 a.m. ET |
NEW YORK,
April 26, 2025 -- Protara Therapeutics, Inc. (Nasdaq:
TARA), a clinical-stage company developing transformative therapies for the treatment of cancer and rare diseases, today announced updated
results from its ongoing Phase 2 open-label ADVANCED-2 trial assessing intravesical TARA-002, the Company’s investigational cell-based
therapy, in high-risk Non-Muscle Invasive Bladder Cancer (NMIBC) patients with carcinoma in situ, or CIS (± Ta/T1), who are Bacillus
Calmette-Guérin (BCG)-Unresponsive or BCG-Naïve. The results will be featured today during an interactive poster session at
the American Urological Association 2025 Annual Meeting in Las Vegas.
“For
patients with high-risk NMIBC, there are few effective and durable therapies available other than radical cystectomy, which we know is
quite difficult for patients to tolerate,” said Tom Jayram, M.D., Director of the Advanced Therapeutics Center at Urology Associates,
and ADVANCED-2 study investigator. “TARA-002 has shown impressive efficacy, safety profile, and 12-month durability in its Phase
2 trial. In the clinic, we have seen TARA-002 become easily integrated into workflow without major hurdles for the patient or staff. This
combination of clinical activity and ease of use makes me optimistic about TARA-002 having a meaningful impact in clinical practice.”
Interim
Results
BCG-Unresponsive
Cohort
The BCG-Unresponsive
dataset includes a total of five patients, all of whom were six- and nine-month evaluable, and three of whom were evaluable at 12 months
as of an April 16, 2025 data cutoff.
| ● | The complete response
(CR) rate at any time in BCG-Unresponsive patients was 100% (5/5). |
| ● | The CR rate in BCG-Unresponsive
patients was 100% (5/5) at six months, 80% (4/5) at nine months, and 67% (2/3) at 12 months. |
BCG-Naïve
Cohort
The BCG-Naïve
dataset includes a total of 21 patients, including 16 evaluable at six months, eight at nine months, and seven at 12 months as of an April
16, 2025 data cutoff.
| ● | The CR rate at any time
in BCG-Naïve patients was 76% (16/21). |
| ● | The CR rate in BCG-Naïve
patients was 63% (10/16) at six months, 63% (5/8) at nine months, and 43% (3/7) at 12 months. |
Safety
The majority
of adverse events were Grade 1 and transient with no Grade 3 or greater treatment-related adverse events (TRAEs) as assessed by study
investigators. No patients discontinued treatment due to TRAEs. The most common adverse events were in line with typical responses to
bacterial immunopotentiation, such as flu-like symptoms. The most common urinary symptoms reflect urinary tract instrumentation effects,
such as bladder spasm, burning sensation, and urinary tract infection. Most bladder irritations resolved shortly after administration
or within a few hours to a few days.
“The
durable results shared today continue to support our conviction that TARA-002 has the potential to make a meaningful difference in the
lives of patients with NMIBC,” said Jesse Shefferman, Chief Executive Officer of Protara Therapeutics. “Notably, we are particularly
pleased with the competitive 12-month CR rates observed in the registrational BCG-Unresponsive cohort as well as the BCG-Naïve cohort.
We look forward to continuing to advance this important trial as we work toward our mission of bringing transformative therapies to patients.”
The Company
continues to expect to present an interim update with results from approximately 25 six-month evaluable BCG-Unresponsive patients by the
end of 2025.
Conference
Call and Webcast
Protara
will host a conference call and webcast to discuss the data on Monday, April 28, 2025, at 8:30 am ET. The live call can be accessed
by registering as a participant here. Upon registration, participants will receive conference
call dial-in information. A live webcast of the event can be accessed by visiting the Events and Presentations section of the Company’s
website: https://ir.protaratx.com. The webcast will be archived for a limited time following the presentation.
About
ADVANCED-2
ADVANCED-2
(NCT05951179) is a Phase 2 open-label trial assessing intravesical TARA-002 in NMIBC patients with carcinoma in situ or CIS (±
Ta/T1) who are Bacillus Calmette-Guérin (BCG)-Unresponsive (n≈100) and BCG-Naïve (n=31). The BCG-Unresponsive cohort
has been designed to be registrational in alignment with the U.S. Food and Drug Administration’s 2024 BCG-Unresponsive
Non-muscle Invasive Bladder Cancer: Developing Drugs and Biological Products for Treatment, Draft Guidance for Industry.
About
TARA-002
TARA-002
is an investigational cell therapy in development for the treatment of NMIBC and of LMs, for which it has been granted Rare Pediatric
Disease Designation by the U.S. Food and Drug Administration. TARA-002 was developed from the same master cell bank of genetically
distinct group A Streptococcus pyogenes as OK-432, a broad immunopotentiator marketed as Picibanil® in Japan by Chugai Pharmaceutical
Co., Ltd. Protara has successfully shown manufacturing comparability between TARA-002 and OK-432.
When TARA-002
is administered, it is hypothesized that innate and adaptive immune cells within the cyst or tumor are activated and produce a pro-inflammatory
response with release of cytokines such as tumor necrosis factor (TNF)-alpha, interferon (IFN)-gamma IL-6, IL-10, IL-12. TARA-002 also
directly kills tumor cells and triggers a host immune response by inducing immunogenic cell death, which further enhances the antitumor
immune response.
About
Non-Muscle Invasive Bladder Cancer (NMIBC)
Bladder
cancer is the 6th most common cancer in the United States, with NMIBC representing approximately 80% of bladder cancer diagnoses.
Approximately 65,000 patients are diagnosed with NMIBC in the United States each year. NMIBC is cancer found in the tissue that
lines the inner surface of the bladder that has not spread into the bladder muscle.
About Protara
Therapeutics, Inc.
Protara
is a clinical-stage biotechnology company committed to advancing transformative therapies for people with cancer and rare diseases. Protara’s
portfolio includes its lead candidate, TARA-002, an investigational cell-based therapy in development for the treatment of non-muscle
invasive bladder cancer (NMIBC) and lymphatic malformations (LMs). The Company is evaluating TARA-002 in an ongoing Phase 2 trial in NMIBC
patients with carcinoma in situ (CIS) who are unresponsive or naïve to treatment with Bacillus Calmette-Guérin (BCG), as well
as a Phase 2 trial in pediatric patients with LMs. Additionally, Protara is developing IV Choline Chloride, an investigational phospholipid
substrate replacement for patients on parenteral nutrition who are otherwise unable to meet their choline needs via oral or enteral routes.
For more information, visit www.protaratx.com.
Forward-Looking
Statements
Statements
contained in this press release regarding matters that are not historical facts are “forward looking statements” within the
meaning of the Private Securities Litigation Reform Act of 1995. Protara may, in some cases, use terms such as “predicts,”
“believes,” “potential,” “proposed,” “continue,” “designed,” “estimates,”
“anticipates,” “expects,” “plans,” “intends,” “may,” “could,”
“might,” “will,” “should” or other words or expressions referencing future events, conditions or circumstances
that convey uncertainty of future events or outcomes to identify these forward-looking statements. Such forward-looking statements include
but are not limited to, statements regarding Protara’s intentions, beliefs, projections, outlook, analyses or current expectations
concerning, among other things: Protara’s business strategy, including its development plans for its product candidates and plans
regarding the timing or outcome of existing or future clinical trials (including reporting data from approximately 25 6-month evaluable
BCG-Unresponsive patients by the end of 2025); statements related to expectations regarding interactions with the U.S. Food and Drug Administration
(FDA); Protara’s financial position; statements regarding the anticipated safety or efficacy of Protara’s product candidates;
and Protara’s outlook for the remainder of the year and future periods. Because such statements are subject to risks and uncertainties,
actual results may differ materially from those expressed or implied by such forward-looking statements. Factors that contribute to the
uncertain nature of the forward-looking statements include: risks that Protara’s financial guidance may not be as expected, as well
as risks and uncertainties associated with: Protara’s development programs, including the initiation and completion of non-clinical
studies and clinical trials and the timing of required filings with the FDA and other regulatory agencies; general market conditions;
changes in the competitive landscape; changes in Protara’s strategic and commercial plans; Protara’s ability to obtain sufficient
financing to fund its strategic plans and commercialization efforts; having to use cash in ways or on timing other than expected; the
impact of market volatility on cash reserves; failure to attract and retain management and key personnel; the impact of general U.S. and
foreign, economic, industry, market, regulatory, political or public health conditions; and the risks and uncertainties associated with
Protara’s business and financial condition in general, including the risks and uncertainties described more fully under the caption
“Risk Factors” and elsewhere in Protara’s filings and reports with the United States Securities and Exchange Commission.
All forward-looking statements contained in this press release speak only as of the date on which they were made and are based on management’s
assumptions and estimates as of such date. Protara undertakes no obligation to update any forward-looking statements, whether as a result
of the receipt of new information, the occurrence of future events or otherwise, except as required by law.
Company Contact:
Justine O’Malley
Protara Therapeutics
[email protected]
646-817-2836
Exhibit 99.2
Interim Data Presentation from the American Urological Association Annual Meeting April 2025
Forward Looking Statements 2 Statements contained in this presentation regarding matters that are not historical facts are "forward looking statements" within the meaning of the Private Securities Litigation Reform Act of 1995 . Protara may, in some cases, use terms such as “predicts,” “believes,” “potential,” “proposed,” “continue,” “designed,” “estimates,” “anticipates,” “expects,” “plans,” “intends,” “may,” “could,” “might,” “will,” “should” or other words or expressions referencing future events, conditions or circumstances that convey uncertainty of future events or outcomes to identify these forward - looking statements . Such forward - looking statements include but are not limited to, statements regarding Protara’s intentions, beliefs, projections, outlook, analyses or current expectations concerning, among other things : Protara’s business strategy, including its development plans for its product candidates and plans regarding the timing or outcome of existing or future clinical trials (including reporting data from approximately 25 6 - month evaluable BCG - Unresponsive patients by the end of 2025 ) ; statements related to expectations regarding interactions with the U . S . Food and Drug Administration (FDA) ; Protara’s financial position ; statements regarding the anticipated safety or efficacy of Protara’s product candidates ; and Protara’s outlook for the remainder of the year and future periods . Because such statements are subject to risks and uncertainties, actual results may differ materially from those expressed or implied by such forward - looking statements . Factors that contribute to the uncertain nature of the forward - looking statements include : risks that Protara’s financial guidance may not be as expected, as well as risks and uncertainties associated with : Protara’s development programs, including the initiation and completion of non - clinical studies and clinical trials and the timing of required filings with the FDA and other regulatory agencies ; general market conditions ; changes in the competitive landscape ; changes in Protara’s strategic and commercial plans ; Protara’s ability to obtain sufficient financing to fund its strategic plans and commercialization efforts ; having to use cash in ways or on timing other than expected ; the impact of market volatility on cash reserves ; failure to attract and retain management and key personnel ; the impact of general U . S . and foreign, economic, industry, market, regulatory, political or public health conditions ; and the risks and uncertainties associated with Protara’s business and financial condition in general, including the risks and uncertainties described more fully under the caption “Risk Factors” and elsewhere in Protara's filings and reports with the United States Securities and Exchange Commission . All forward - looking statements contained in this presentation speak only as of the date on which they were made and are based on management's assumptions and estimates as of such date . Protara undertakes no obligation to update any forward - looking statements, whether as a result of the receipt of new information, the occurrence of future events or otherwise, except as required by law . © 2025 Protara Therapeutics. All Rights Reserved – Do Not Copy or Distribute. |
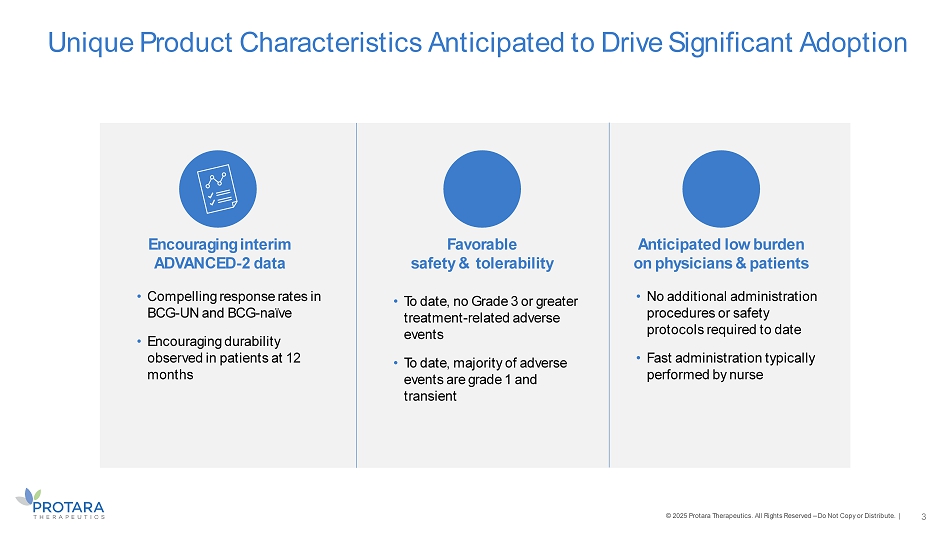
Unique Product Characteristics Anticipated to Drive Significant Adoption • Compelling response rates in BCG - UN and BCG - naïve • Encouraging durability observed in patients at 12 months 3 • To date, no Grade 3 or greater treatment - related adverse events • To date, majority of adverse events are grade 1 and transient • No additional administration procedures or safety protocols required to date • Fast administration typically performed by nurse Encouraging interim ADVANCED - 2 data Favorable safety & tolerability Anticipated low burden on physicians & patients © 2025 Protara Therapeutics. All Rights Reserved – Do Not Copy or Distribute. |
TARA - 002 Lyophilized, Inactivated Group A Streptococcus pyogenes
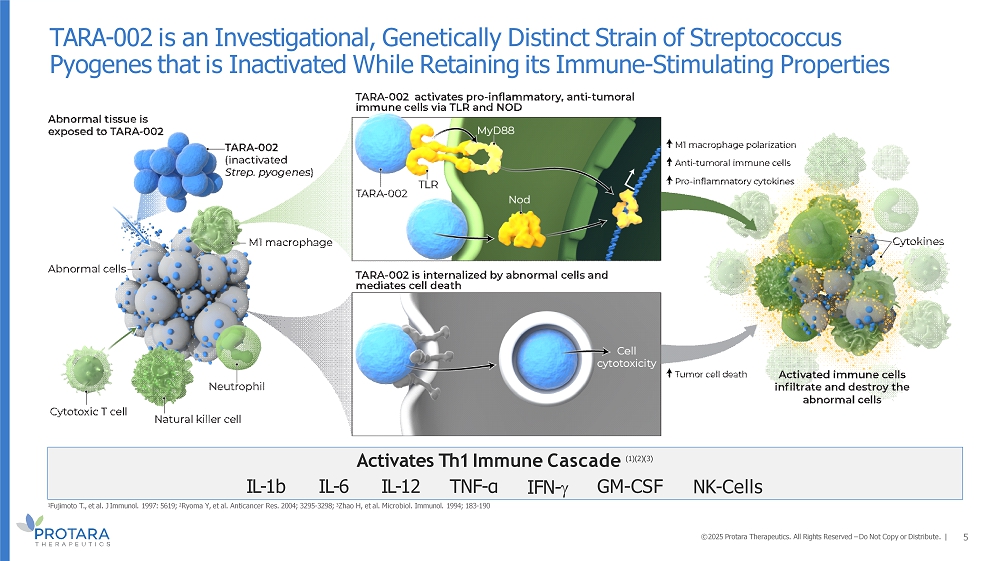
Activates Th1 Immune Cascade (1)(2)(3) TARA - 002 is an Investigational, Genetically Distinct Strain of Streptococcus Pyogenes that is Inactivated While Retaining its Immune - Stimulating Properties 5 NK - Cells IL - 1b IL - 6 IL - 12 TNF - α IFN - GM - CSF 1 Fujimoto T., et al. J Immunol. 1997: 5619; 2 Ryoma Y, et al. Anticancer Res. 2004; 3295 - 3298; 3 Zhao H, et al. Microbiol. Immunol. 1994; 183 - 190 © 2025 Protara Therapeutics. All Rights Reserved – Do Not Copy or Distribute. |
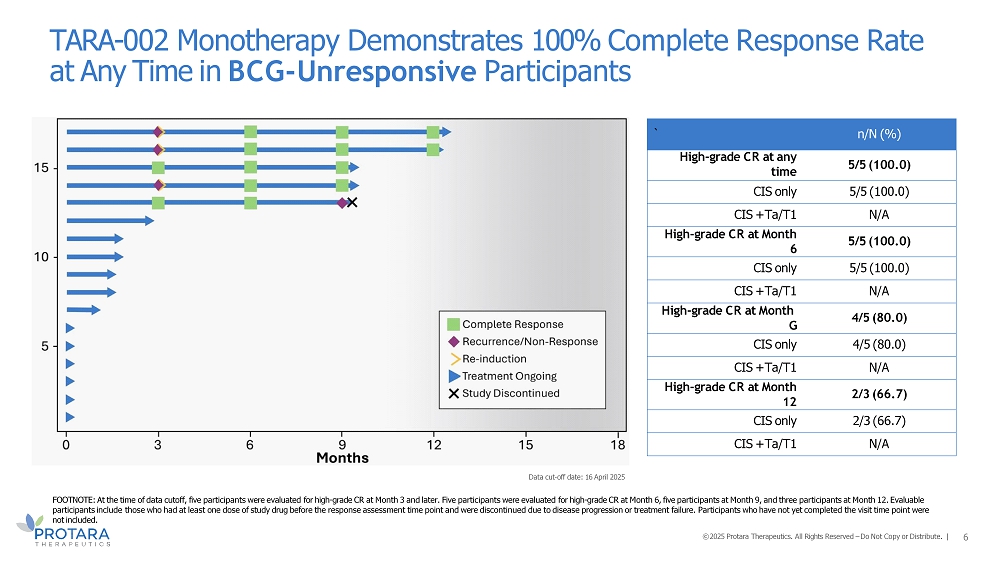
Data cut - off date: 16 April 2025 TARA - 002 Monotherapy Demonstrates 100% Complete Response Rate at Any Time in BCG - Unresponsive Participants 6 n/N (%) ` 5/5 (100.0) High - grade CR at any time 5/5 (100.0) CIS only N/A CIS + Ta/T1 5/5 (100.0) High - grade CR at Month 6 5/5 (100.0) CIS only N/A CIS + Ta/T1 4/5 (80.0) High - grade CR at Month G 4/5 (80.0) CIS only N/A CIS + Ta/T1 2/3 (66.7) High - grade CR at Month 12 2/3 (66.7) CIS only N/A CIS + Ta/T1 FOOTNOTE: At the time of data cutoff, five participants were evaluated for high - grade CR at Month 3 and later. Five participants were evaluated for high - grade CR at Month 6, five participants at Month 9, and three participants at Month 12. Evaluable participants include those who had at least one dose of study drug before the response assessment time point and were discontinued due to disease progression or treatment failure. Participants who have not yet completed the visit time point were not included. © 2025 Protara Therapeutics. All Rights Reserved – Do Not Copy or Distribute. |
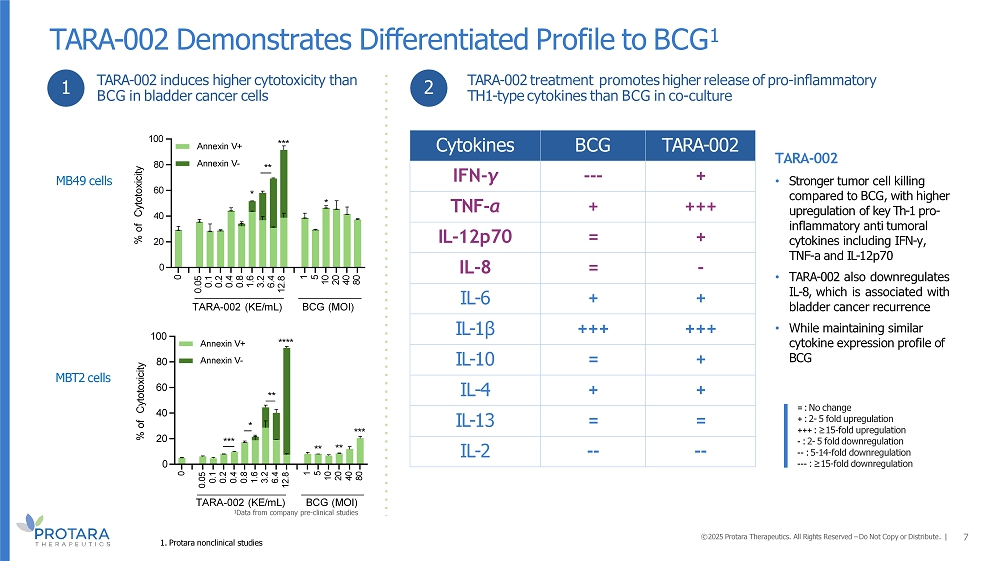
TARA - 002 BCG Cytokines + -- - IFN - γ +++ + TNF - α + = IL - 12p70 - = IL - 8 + + IL - 6 +++ +++ IL - 1β + = IL - 10 + + IL - 4 = = IL - 13 - - - - IL - 2 TARA - 002 Demonstrates Differentiated Profile to BCG 1 7 = : No change + : 2 - 5 fold upregulation +++ : ≥ 15 - fold upregulation - : 2 - 5 fold downregulation - - : 5 - 14 - fold downregulation -- - : ≥ 15 - fold downregulation 1 2 TARA - 002 (KE/mL) BCG (MOI) 1 Data from company pre - clinical studies MB49 cells MBT2 cells TARA - 002 induces higher cytotoxicity than BCG in bladder cancer cells TARA - 002 treatment promotes higher release of pro - inflammatory TH1 - type cytokines than BCG in co - culture 0 0.05 0.1 0.2 0.4 0.8 1.6 3.2 6.4 12.8 1 5 10 20 40 80 0 20 40 60 80 100 % of Cytotoxicity *** * ** **** *** ** ** Annexin V+ Annexin V - 0 0.05 0.1 0.2 0.4 0.8 1.6 3.2 6.4 12.8 1 5 10 20 40 80 0 20 40 60 80 100 % of Cytotoxicity TARA - 002 (KE/mL) BCG (MOI) *** ** * * Annexin V - Annexin V+ TARA - 002 • Stronger tumor cell killing compared to BCG, with higher upregulation of key Th - 1 pro - inflammatory anti tumoral cytokines including IFN - y, TNF - a and IL - 12p70 • TARA - 002 also downregulates IL - 8 , which is associated with bladder cancer recurrence • While maintaining similar cytokine expression profile of BCG 1. Protara nonclinical studies © 2025 Protara Therapeutics. All Rights Reserved – Do Not Copy or Distribute. |
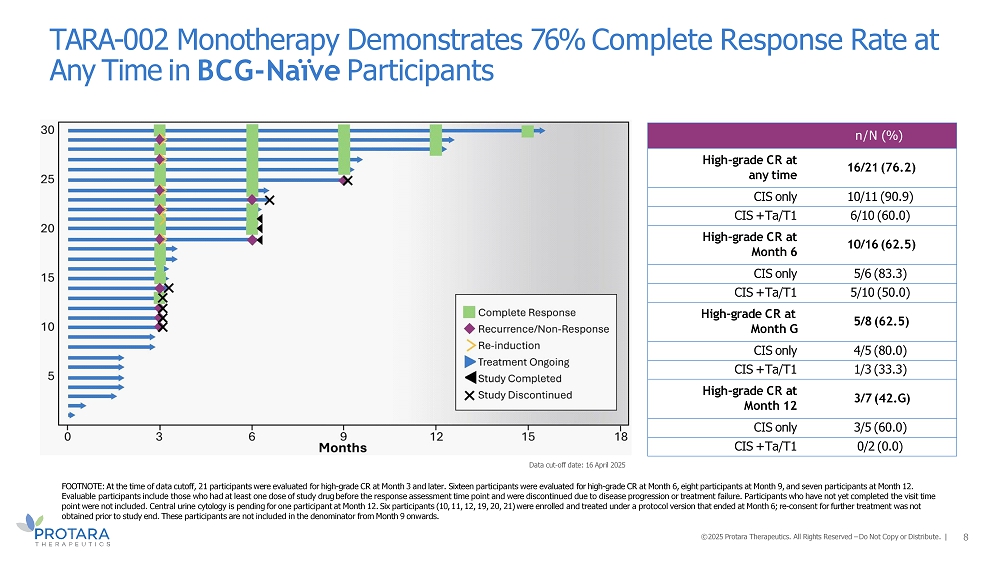
Data cut - off date: 16 April 2025 FOOTNOTE: At the time of data cutoff, 21 participants were evaluated for high - grade CR at Month 3 and later. Sixteen participants were evaluated for high - grade CR at Month 6, eight participants at Month 9, and seven participants at Month 12. Evaluable participants include those who had at least one dose of study drug before the response assessment time point and were discontinued due to disease progression or treatment failure. Participants who have not yet completed the visit time point were not included. Central urine cytology is pending for one participant at Month 12. Six participants (10, 11, 12, 19, 20, 21) were enrolled and treated under a protocol version that ended at Month 6; re - consent for further treatment was not obtained prior to study end. These participants are not included in the denominator from Month 9 onwards. TARA - 002 Monotherapy Demonstrates 76% Complete Response Rate at Any Time in BCG - Naïve Participants 8 n/N (%) 16/21 (76.2) High - grade CR at any time 10/11 (90.9) CIS only 6/10 (60.0) CIS + Ta/T1 10/16 (62.5) High - grade CR at Month 6 5/6 (83.3) CIS only 5/10 (50.0) CIS + Ta/T1 5/8 (62.5) High - grade CR at Month G 4/5 (80.0) CIS only 1/3 (33.3) CIS + Ta/T1 3/7 (42.G) High - grade CR at Month 12 3/5 (60.0) CIS only 0/2 (0.0) CIS + Ta/T1 © 2025 Protara Therapeutics. All Rights Reserved – Do Not Copy or Distribute. |
Favorable and Well - tolerated Safety Profile Across BCG Exposures 9 Data cut - off date: 16 April 2025 Grade 4/5 Grade 3 Grade 2 Grade 1 Any Grade N=43 0 8 (19) 13 (30) 26 (60) 32 (74) Participants with TEAEs ^, n (%) 0 0 1 (2) 12 (28) 13 (30) Participants with Related TEAEs ^, n (%) 0 0 0 6 (14) 6 (14) Dysuria 0 0 0 4 (9) 4 (9) Bladder spasm 0 0 0 3 (7) 3 (7) Fatigue 0 0 0 3 (7) 3 (7) Micturition urgency 0 0 0 2 (5) 2 (5) Haematuria 0 0 0 1 (2) 1 (2) Bladder discomfort 0 6 (14) 2 (5) 0 6 (14) Participants with Serious TEAEs ^ + , n (%) 0 0 0 0 0 Participants with Related TEAEs leading to Study Drug Withdrawal , n (%) ABBREVIATIONS: TEAE = Treatment - Emergent Adverse Event FOOTNOTE: A total of 43 participants were exposed to at least one dose of TARA - 002; 13 were BCG - unresponsive and 30 were BCG - naïve. Adverse events that are recorded after the initiation of treatment are classified as TEAEs. Severity of adverse event is based on NCI - CTCAE Version 5.0. Non - treatment - related serious TEAEs included urosepsis, urinary tract infection, small intestinal obstruction, incarcerated hernia, hydronephrosis, cellulitis, lower urinary tract symptoms, and ataxia. © 2025 Protara Therapeutics. All Rights Reserved – Do Not Copy or Distribute. |

Q&A 10

APPENDIX
Abbreviations: CR = complete response; CIS = carcinoma in situ *Aligned with the FDA’s 2024 BCG Unresponsive NMIBC: Developing Drugs and Biologics for Treatment Guidance for Industry. †Residual CIS and/or recurrence of HGTa Primary endpoint of high - grade complete response (CR) at any time at 6 months; Key secondary of 12 - month DOR TARA - 002 in NMIBC: ADVANCED - 2 Clinical Trial Design 12 DAY 1 MONTH 3 MONTH 6 MONTH 18 MONTH 60 REGISTRATIONAL DESIGN*: BCG - Unresponsive (CIS “ Ta/T1) BCG Naïve (CIS “ Ta/T1) Induction (N=100) 6 weekly instillations Induction (N=27) 6 weekly instillations CR, Maintenance (months 3 - 18) 3 weekly instillations every 3 months Follow - up Follow - up CR, Maintenance (months 3 - 18) 3 weekly instillations every 3 months Maintenance (months 6 - 18) 3 weekly instillations every 3 months Maintenance (months 6 - 18) 3 weekly instillations every 3 months Re - Induction (if eligible*) 6 weekly instillations Re - Induction (if eligible*) 6 weekly instillations Follow - up Follow - up © 2025 Protara Therapeutics. All Rights Reserved – Do Not Copy or Distribute. |
ADVANCED - 2: Demographics and Baseline Characteristics 13 Data cut - off date: 16 April 2025 ABBREVIATIONS: ECOG= Eastern Cooperative Oncology Group; n = number of participants FOOTNOTE: *The swimmer’s plot excludes 2 participants who withdrew prior to the response assessment; The safety analysis excludes 6 participants who had not yet been exposed to TARA - 002. † The swimmer’s plot excludes 1 participant who withdrew prior to the response assessment; The safety analysis excludes 1 participant who had not yet been exposed to TARA - 002. BCG - naïve N = 31 † BCG - unresponsive N = 1G* Age, years 71.0 (45, 89) 80.0 (47, 92) Median (Min, Max) Sex, n (%) 25/31 (80.6) 15/19 (78.9) Male Race, n (%) 29/31 (93.5) 16/19 (84.2) White 1/31 (3.2) 0/19 (0.0) Black 0/31 (0.0) 2/19 (10.5) Asian 1/31 (3.2) 1/19 (5.3) Not reported Ethnicity, n (%) 28/31 (90.3) 19/19 (100.0) Non - Hispanic ECOG score, n (%) 25/30 (83.3) 13/15 (86.7) 0 Baseline Diagnosis, n (%) 18/31 (58.1) 16/17 (94.1) CIS only 9/31 (29.0) 1/17 (5.9) CIS + Ta 4/31 (12.9) 0/17 (0.0) CIS + T1 © 2025 Protara Therapeutics. All Rights Reserved – Do Not Copy or Distribute. |
Exhibit 99.3
SAFETY TABLE 4. FAVORABLE AND WELL - TOLERATED SAFETY PROFILE ACROSS BCG EXPOSURES Grade 4/5 Grade 3 Grade 2 Grade 1 Any Grade N=43 0 (0) 8 (19) 13 (30) 26 (60) 32 (74) Participants with TEAEs, n (%) 0 (0) 0 (0) 1 (2) 12 (28) 13 (30) Participants with Related TEAEs, n (%) 0 (0) 6 (14) 2 (5) 0 (0) 6 (14) Participants with Serious TEAEs, n (%) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) Participants with Related TEAEs Leading to Study Drug Withdrawal, n (%) ABBREVIATIONS: TEAE = Treatment - Emergent Adverse Event FOOTNOTE: A total of 43 participants were exposed to at least one dose of TARA - 002; 13 were BCG - unresponsive and 30 were BCG - naïve. Adverse events that are recorded after the initiation of treatment are classified as TEAEs. Severity of adverse event is based on NCI - CTCAE Version 5.0. Non - treatment - related serious TEAEs included urosepsis, urinary tract infection, small intestinal obstruction, incarcerated hernia, hydronephrosis, cellulitis, lower urinary tract symptoms, and ataxia. • Majority of TEAEs were Grade 1 and transient ( Table 4 ). • No participants experienced treatment - related serious AEs (SAEs) or related TEAEs leading to withdrawal or death ( Table 4 ). • Common urinary AEs reflect urinary tract instrumentation effects, such as bladder spasm, burning sensation, and UTI. • Systemic AEs were consistent with the known safety profile of an immune - potentiating drug, such as flu - like symptoms. Baseline Characteristics TABLE 1. BASELINE DEMOGRAPHICS AND CLINICAL CHARACTERISTICS BCG - unresponsive N=1G* BCG - naïve N=31 † Age, years Median 80.0 71.0 Min, max 47, 92 45, 89 Sex, n (%) Male 15/19 (78.9) 25/31 (80.6) Race, n (%) White Black Asian Not reported 16/19 (84.2) 0/19 (0.0) 2/19 (10.5) 1/19 (5.3) 29/31 (93.5) 1/31 (3.2) 0/31 (0.0) 1/31 (3.2) Ethnicity, n (%) Non - Hispanic 19/19 (100.0) 28/31 (90.3) ECOG Score, n (%) 0 13/15 (86.7) 25/30 (83.3) Baseline Diagnosis, n (%) CIS Only CIS+Ta CIS+T1 16/17 (94.1) 1/17 (5.9) 0/17 (0.0) 18/31 (58.1) 9/31 (29.0) 4/31 (12.9) ABBREVIATIONS: ECOG= Eastern Cooperative Oncology Group; n = number of participants FOOTNOTE: *Figure 2 excludes 2 participants who withdrew prior to the response assessment; Table 4 excludes 6 participants who had not yet been exposed to TARA - 002. † Figure 3 excludes 1 participant who withdrew prior to the response assessment; Table 4 excludes 1 participant who had not yet been exposed to TARA - 002. RESULTS Presented at the American Urological Association Annual Meeting, April 2C - 2G, 2025; Las Vegas, Nevada DISCLOSURE: This study is funded by Protara Therapeutics, Inc. Digital and print editorial services powered by Princeton Biomedical Comm., LLC. Preliminary Efficacy and Safety Results From ADVANCED - 2: A Phase - 2 Open - label Study of Intravesical TARA - 002 In Adults With High - grade Non - muscle Invasive Bladder Cancer Gautam Jayram 1 , Eugene Kramolowsky 2 , Myroslava Doronina 3 , William Tabayoyong 4 , Brian Mazzarella 5 , Jacqueline Zummo 6 , Wei Sun 6 , Khushboo Belani 6 , Eppie Brown 6 , Andrea DiFiglia 6 , Claire Middleton 6 , Brian Desch 6 , Chen Ǫuin Lam 7 , Neal Shore 8 , Zoreslava Lysak 3 , Evgeny Levenko 3 1 Urology Associates P.C., Nashville, TN, United States; 2 Virginia Urology, Richmond, Virginia, United States; 3 Arensia Exploratory Medicine LLC, Kyiv, Ukraine; 4 Department of Urology, University of Rochester, Rochester, NY, United States; 5 Urology Austin, Austin, Texas, United States; 6 Protara Therapeutics, Inc., New York, NY, United States; 7 Pharmapace Inc., San Diego, CA, United States; 8 Carolina Urologic Research Center, Myrtle Beach, SC, United States CONCLUSIONS • TARA - 002 was well tolerated and demonstrated encouraging clinical activity in both BCG - naïve and BCG - unresponsive participants with high - risk NMIBC with CIS “ Ta/T1. • TARA - 002 demonstrated encouraging durability of response up to 12 months after initiation of TARA - 002 therapy in both BCG - naïve and BCG - unresponsive participants. • These interim findings support the potential of TARA - 002 as an intravesical immunotherapy for high - risk NMIBC. • Additional data from this study will further the understanding of the efficacy and safety profile of TARA - 002 in both BCG - naïve and BCG - unresponsive high - risk NMIBC patients. Response Assessment FIGURE 2. TARA - 002 MONOTHERAPY DEMONSTRATES 100% HIGH - GRADE COMPLETE RESPONSE AT ANY TIME IN BCG - UNRESPONSIVE PARTICIPANTS 0 3 6 12 15 18 Complete Response Recurrence/Non - Response Re - induction Treatment Ongoing Study Discontinued 9 Months 15 10 5 • For BCG - naïve participants, the rate of high - grade CR at any time was 76% (16 of 21), 63% (10 of 16) at Month 6, 63% (5 of 8) at Month 9, and 43% (3 of 7) at Month 12. • Among BCG - naïve participants who achieved a CR at Month 3 and remained on study, 86% (6 of 7) maintained their response through Month 6. Of those evaluable at later time points, 75% (3 of 4) maintained a response through Month 9, 100% (2 of 2) maintained a response at Month 12 • Of the five BCG - naïve participants who did not achieve an initial CR and received re - induction, the CR rate at Month 6 was 80% (4 of 5). • For BCG - unresponsive participants, the rate of high - grade CR at any time was 100% (5 of 5), 100% (5 of 5) at Month 6, 80% (4 of 5) at Month 9, and 67% (2 of 3) at Month 12. • Among the three BCG - unresponsive participants who did not achieve an initial CR and received re - induction, all converted to a CR by Month 6, which was maintained at Month 9 (100%, 3 of 3). TABLE 2. TARA - 002 MONOTHERAPY DEMONSTRATES PROMISING EFFICACY AND ENCOURAGING DURABILITY IN BCG - UNRESPONSIVE PARTICIPANTS FIGURE 3. TARA - 002 MONOTHERAPY DEMONSTRATES 76% HIGH - GRADE COMPLETE RESPONSE AT ANY TIME IN BCG - NAÏVE PARTICIPANTS 0 3 6 12 15 18 Complete Response Recurrence/Non - Response Re - induction Treatment Ongoing Study Completed Study Discontinued 9 Months 30 25 20 15 10 5 TABLE 3. TARA - 002 MONOTHERAPY DEMONSTRATES PROMISING EFFICACY AND ENCOURAGING DURABILITY IN BCG - NAÏVE PARTICIPANTS BCG - unresponsive n/N (%) High - grade CR at any time CIS only 5/5 (100.0) 5/5 (100.0) CIS + Ta/T1 High - grade CR at Month 6 N/A 5/5 (100.0) CIS only 5/5 (100.0) CIS + Ta/T1 N/A High - grade CR at Month G CIS only 4/5 (80.0) 4/5 (80.0) CIS + Ta/T1 N/A High - grade CR at Month 12 CIS only CIS + Ta/T1 2/3 (66.7) 2/3 (66.7) N/A BCG - naïve n/N (%) High - grade CR at any time CIS only CIS + Ta/T1 High - grade CR at Month 6 16/21 (76.2) 10/11 (90.9) 6/10 (60.0) 10/16 (62.5) CIS only 5/6 (83.3) CIS + Ta/T1 5/10 (50.0) High - grade CR at Month G 5/8 (62.5) CIS only CIS + Ta/T1 High - grade CR at Month 12 4/5 (80.0) 1/3 (33.3) 3/7 (42.G) CIS only CIS + Ta/T1 3/5 (60.0) 0/2 (0.0) INTRODUCTION • Effective management of non - muscle invasive bladder cancer (NMIBC) remains a critical unmet medical need, further complicated by an ongoing shortage and limited availability of Bacillus Calmette - Guérin (BCG). • TARA - 002 is a unique formulation containing inactivated cells of Streptococcus pyogene s (Group A, type 3) Su strain administered intravesically. • TARA - 002 is a broad spectrum immune potentiator that elicits a TH1 pro - inflammatory cytokine response. • This study reports updated efficacy and safety data of TARA - 002 in participants with NMIBC with CIS “ Ta/T1, including 9 - month and 12 - month evaluable participants. METHODS • ADVANCED - 2 (NCT05951179) is an ongoing, actively enrolling, Phase 2, open - label study to evaluate the safety and efficacy of intravesical instillation of TARA - 002 (40 KE) in adults ≥18 years with BCG - unresponsive and BCG - naïve (defined as patients who have never been exposed and those who have not received intravesical BCG for at least 24 months) NMIBC with CIS “ Ta/T1 who have active disease ( Figure 1 ). • The primary endpoint is high - grade complete response (CR) at any time up to Month 6. • Key secondary endpoint is durability of response at Month 12. • Participants are followed for safety throughout the study. • The data cutoff date is April 16, 2025. FIGURE 1. ADVANCED - 2 STUDY SCHEMA REGISTRATIONAL DESIGN*: BCG - unresponsive (CIS “ Ta/T1) Induction (N=100) CR, Maintenance (months 3 - 18) Follow up 6 weekly instillations 3 weekly instillations every 3 months Re - induction (if eligible † ) Maintenance (months 6 - 18) Follow up 6 weekly instillations 3 weekly instillations every 3 months Day 1 Month 3 Month 6 Month 18 Month 60 BCG - naïve (CIS “ Ta/T1) Induction (N=31) CR, Maintenance (months 3 - 18) Follow up 6 weekly instillations 3 weekly instillations every 3 months Re - induction (if eligible † ) Maintenance (months 6 - 18) Follow up 6 weekly instillations 3 weekly instillations every 3 months Day 1 Month 3 Month 6 Month 18 Month 60 ABBREVIATIONS: BCG = Bacillus Calmette - Guérin; CR = complete response; CIS = carcinoma in situ ; FDA = Food and Drug Administration; HG = high - grade *Aligned with the U.S. FDA’s 2024 BCG - unresponsive NMIBC: Developing Drugs and Biologics for Treatment Guidance for Industry. †Residual CIS and/or recurrence of HGTa • Enrollment of BCG - unresponsive participants is ongoing. • Enrollment of BCG - naïve participants is complete. FOOTNOTE (FIGURE 3 AND TABLE 3): At the time of data cutoff, 21 participants were evaluated for high - grade CR at Month 3 and later. Sixteen participants were evaluated for high - grade CR at Month 6, 8 participants at Month 9, and 7 participants at Month 12. Evaluable participants include those who had at least one dose of study drug before the response assessment time point and were discontinued due to disease progression or treatment failure. Participants who have not yet completed the visit time point were not included. Central urine cytology is pending for 1 participant at Month 12. Six participants (10, 11, 12, 19, 20, 21) were enrolled and treated under a protocol version that ended at Month 6; re - consent for further treatment was not obtained prior to study end. These participants are not included in the denominator from Month 9 onwards. FOOTNOTE (FIGURE 2 AND TABLE 2 ) : At the time of data cutoff, 5 participants were evaluated for high - grade CR at Month 3 and later . Five participants were evaluated for high - grade CR at Month 6 , 5 participants at Month 9 , and 3 participants at Month 12 . Evaluable participants include those who had at least one dose of study drug before the response assessment time point and were discontinued due to disease progression or treatment failure . Participants who have not yet completed the visit time point were not included .