
Exhibit 99.2 Corporate Presentation August 2022
Cautionary note regarding forward-looking statements This presentation
contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. These statements may be identified by the use of words such as, but not limited to, anticipate, believe, continue, could, estimate,
expect, intend, may, might, plan, potential, predict, project, should, target, will, or would or other similar terms or expressions that concern our expectations, plans and intentions. Forward-looking statements include, without limitation,
statements regarding our expectations, strategies, plans and intentions. Forward-looking statements are neither historical facts nor assurances of future performance. Instead, they are based on our current beliefs, expectations, and assumptions. New
risks and uncertainties may emerge from time to time, and it is not possible to predict all risks and uncertainties. No representations or warranties (expressed or implied) are made about the accuracy of any such forward-looking statements. Such
forward-looking statements are subject to a number of material risks and uncertainties including but not limited to: the efficacy and safety of VRDN-001 and VRDN-002 for the treatment of TED; the relationship between the results from the positive
data from the ongoing Phase 1/2 clinical trial of VRDN-001 and the first-in-human Phase 1 clinical trial of VRDN-002 and results of future of ongoing clinical trials; the timing, progress and plans for our ongoing and future research and clinical
development programs; trial protocols for ongoing clinical trials, including the clinical trials for VRDN-001 and VRDN 002; expectations regarding the timing for data, including the expected timing of additional data from the ongoing Phase 1/2
clinical trial of VRDN-001 and the first-in-human Phase 1 clinical trial of VRDN-002; uncertainty and potential delays related to clinical drug development; the duration and impact of regulatory delays in our clinical programs; the timing of and our
ability to obtain and maintain regulatory approvals for our therapeutic candidates, including VRDN-001 and VRDN-002; manufacturing risks; competition from other therapies or products; other matters that could affect the sufficiency of existing cash,
cash equivalents and short-term investments to fund operations; our financial position and its projected cash runway; our future operating results and financial performance; the clinical utility of our therapeutic candidates and our intellectual
property position; the timing of pre-clinical and clinical trial activities and reporting results from same; the effects from the COVID-19 pandemic on our research, development and business activities and operating results, including those risks set
forth under the caption Risk Factors in our Annual Report on Form 10-K filed with the Securities and Exchange Commission (SEC) on March 11, 2022 and other subsequent disclosure documents filed with the SEC. The forward-looking statements in this
presentation represent our views as of the date of this presentation. Neither we, nor our affiliates, advisors, or representatives, undertake any obligation to publicly update or revise any forward-looking statement, whether as a result of new
information, future events or otherwise, except as required by law. These forward-looking statements should not be relied upon as representing our views as of any date subsequent to the date of this presentation. This presentation also contains
estimates and other statistical data made by independent parties and by us relating to market size and other data about our industry. This data involves a number of assumptions and limitations, and you are cautioned not to give undue weight to such
estimates. In addition, projections, assumptions and estimates of our future performance and the future performance of the markets in which we operate are necessarily subject to a high degree of uncertainty and risk. 2
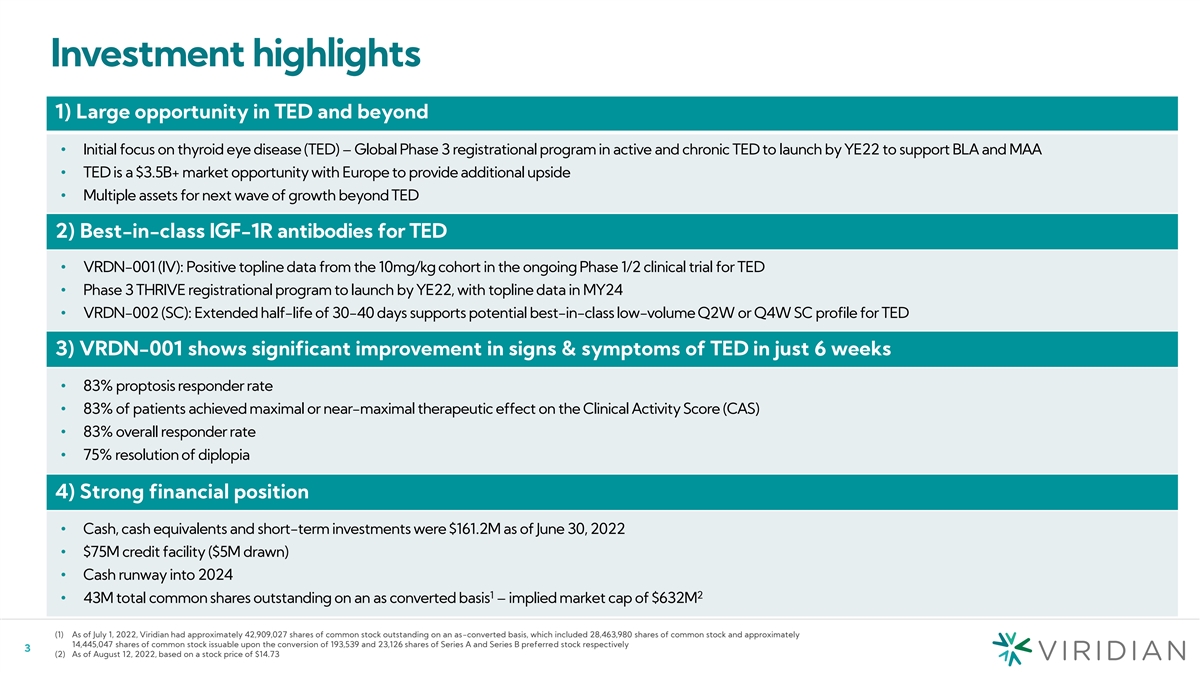
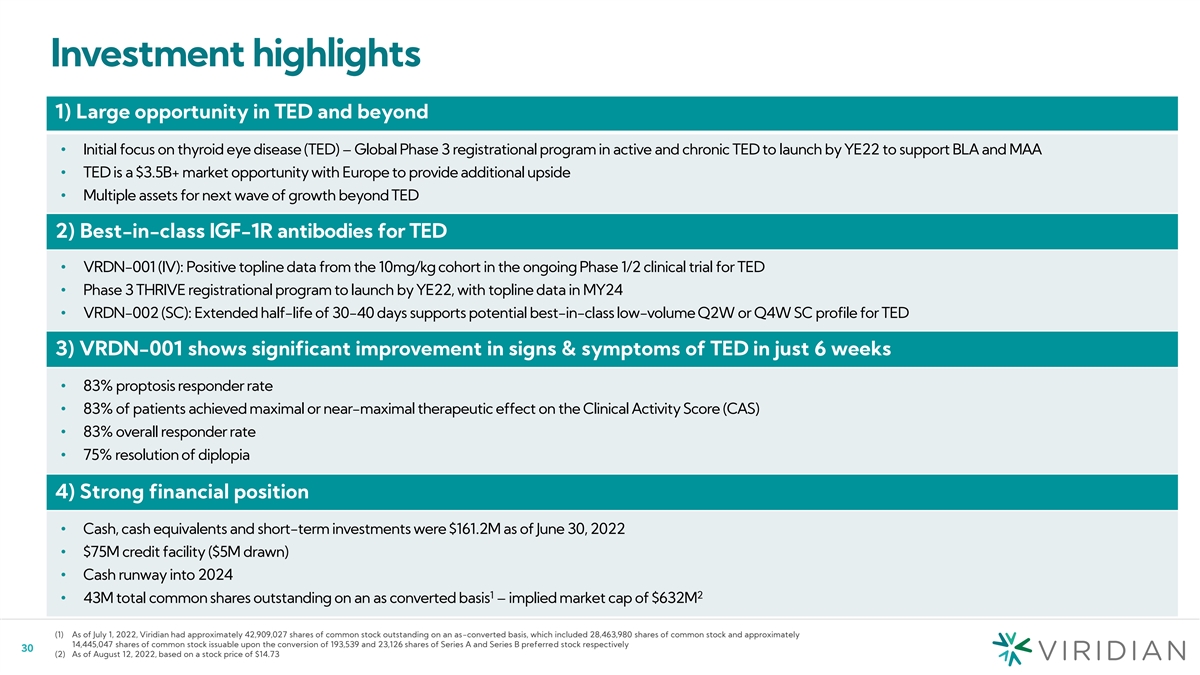
Investment highlights 1) Large opportunity in TED and beyond •
Initial focus on thyroid eye disease (TED) – Global Phase 3 registrational program in active and chronic TED to launch by YE22 to support BLA and MAA • TED is a $3.5B+ market opportunity with Europe to provide additional upside •
Multiple assets for next wave of growth beyond TED 2) Best-in-class IGF-1R antibodies for TED • VRDN-001 (IV): Positive topline data from the 10mg/kg cohort in the ongoing Phase 1/2 clinical trial for TED • Phase 3 THRIVE registrational
program to launch by YE22, with topline data in MY24 • VRDN-002 (SC): Extended half-life of 30-40 days supports potential best-in-class low-volume Q2W or Q4W SC profile for TED 3) VRDN-001 shows significant improvement in signs & symptoms
of TED in just 6 weeks • 83% proptosis responder rate • 83% of patients achieved maximal or near-maximal therapeutic effect on the Clinical Activity Score (CAS) • 83% overall responder rate • 75% resolution of diplopia 4)
Strong financial position • Cash, cash equivalents and short-term investments were $161.2M as of June 30, 2022 • $75M credit facility ($5M drawn) • Cash runway into 2024 1 2 • 43M total common shares outstanding on an as
converted basis – implied market cap of $632M (1) As of July 1, 2022, Viridian had approximately 42,909,027 shares of common stock outstanding on an as-converted basis, which included 28,463,980 shares of common stock and approximately
14,445,047 shares of common stock issuable upon the conversion of 193,539 and 23,126 shares of Series A and Series B preferred stock respectively 3 (2) As of August 12, 2022, based on a stock price of $14.73
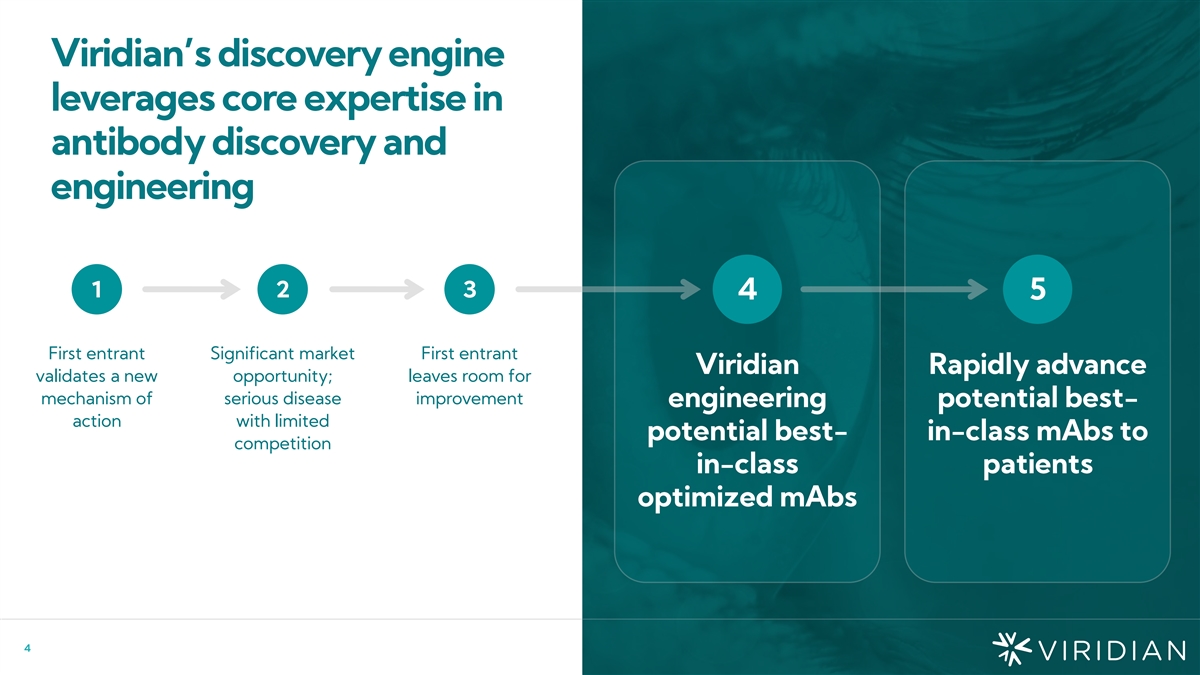
Viridian’s discovery engine leverages core expertise in antibody
discovery and engineering 1 2 3 4 5 First entrant Significant market First entrant Viridian Rapidly advance validates a new opportunity; leaves room for mechanism of serious disease improvement engineering potential best- action with limited
potential best- in-class mAbs to competition in-class patients optimized mAbs 4 Strategy
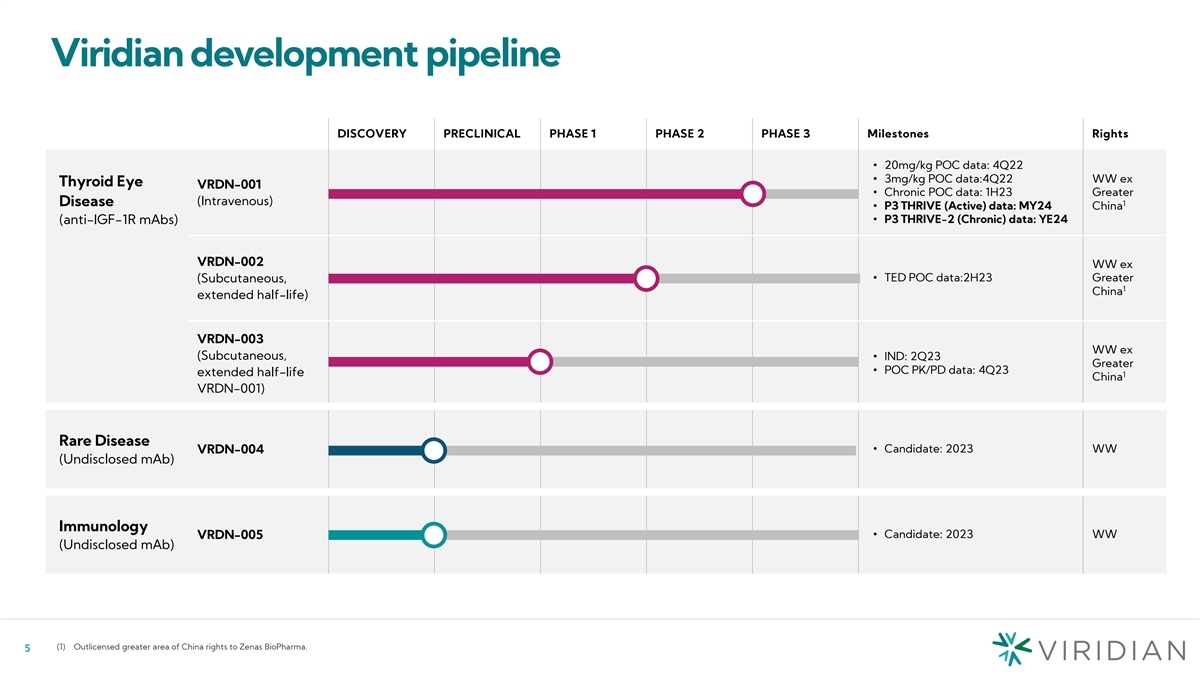
Viridian development pipeline DISCOVERY PRECLINICAL PHASE 1 PHASE 2
PHASE 3 Milestones Rights • 20mg/kg POC data: 4Q22 • 3mg/kg POC data:4Q22 WW ex Thyroid Eye VRDN-001 • Chronic POC data: 1H23 Greater (Intravenous) Disease 1 • P3 THRIVE (Active) data: MY24 China (anti-IGF-1R mAbs)• P3
THRIVE-2 (Chronic) data: YE24 VRDN-002 WW ex • TED POC data:2H23 Greater (Subcutaneous, 1 China extended half-life) VRDN-003 WW ex (Subcutaneous, • IND: 2Q23 Greater • POC PK/PD data: 4Q23 extended half-life 1 China VRDN-001) Rare
Disease • Candidate: 2023 WW VRDN-004 (Undisclosed mAb) Immunology VRDN-005• Candidate: 2023 WW (Undisclosed mAb) (1) Outlicensed greater area of China rights to Zenas BioPharma. 5
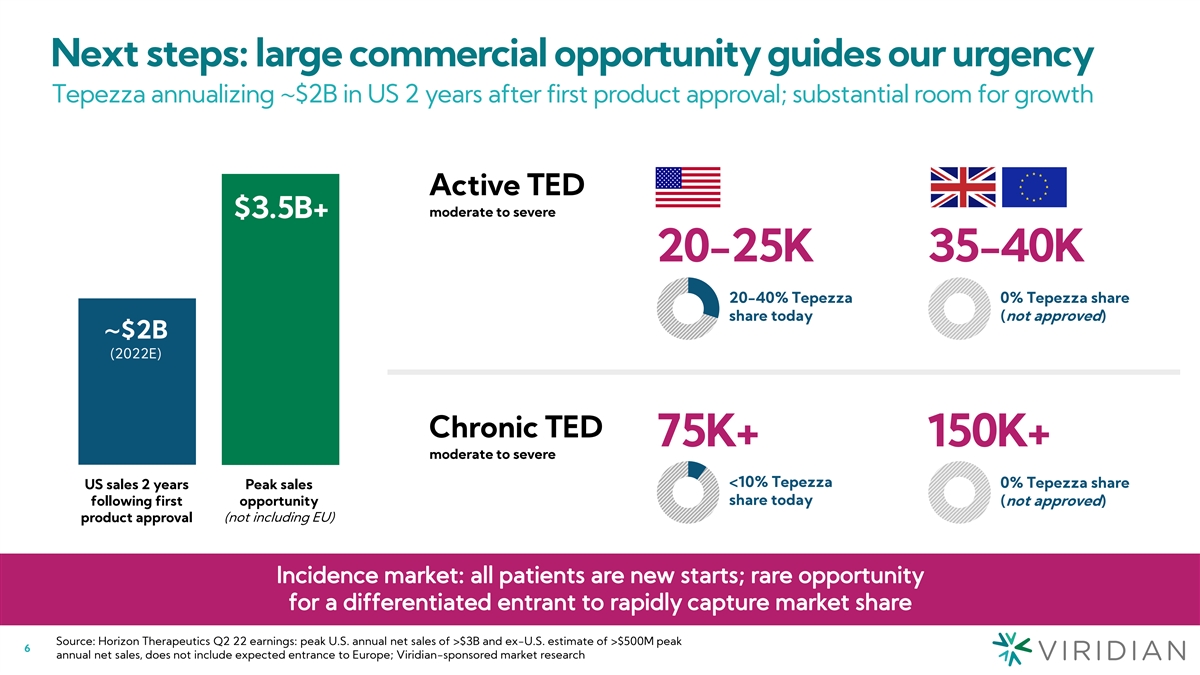
Next steps: large commercial opportunity guides our urgency Tepezza
annualizing ~$2B in US 2 years after first product approval; substantial room for growth Active TED moderate to severe $3.5B+ 20-25K 35-40K 20-40% Tepezza 0% Tepezza share share today (not approved) ~$2B (2022E) Chronic TED 75K+ 150K+ moderate to
severe <10% Tepezza 0% Tepezza share US sales 2 years Peak sales share today following first opportunity (not approved) product approval (not including EU) Source: Horizon Therapeutics Q2 22 earnings: peak U.S. annual net sales of >$3B and
ex-U.S. estimate of >$500M peak 6 annual net sales, does not include expected entrance to Europe; Viridian-sponsored market research

VRDN-001 Potential best-in-class IV treatment for TED 7
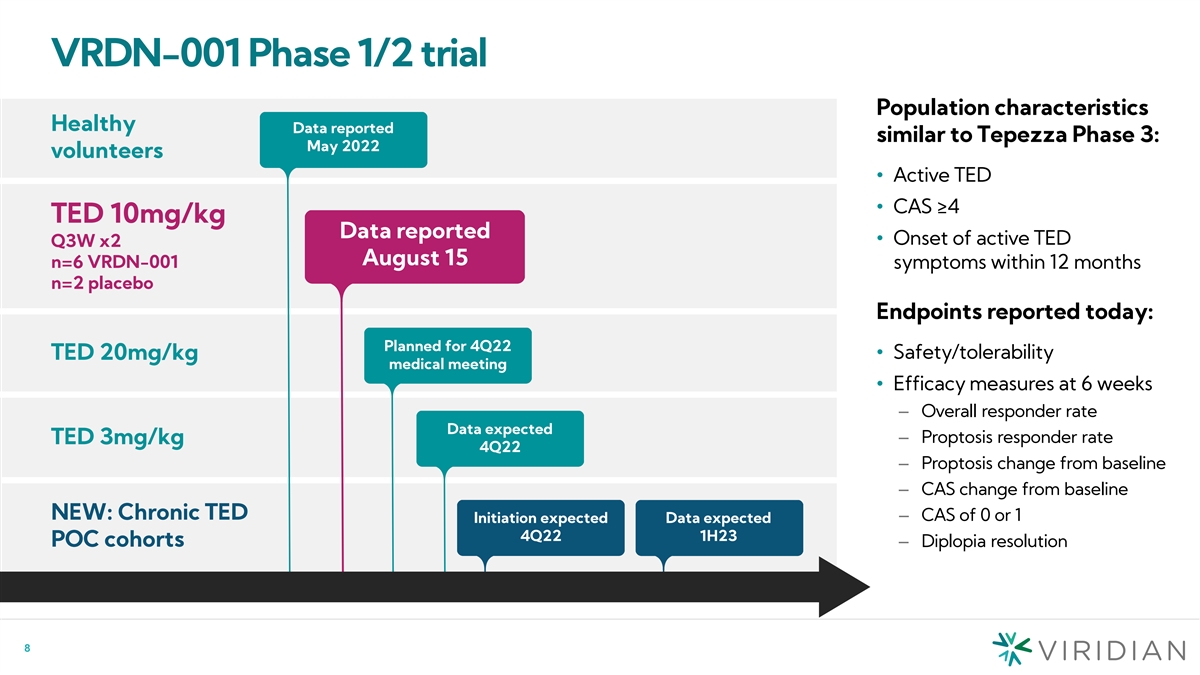
VRDN-001 Phase 1/2 trial Population characteristics Healthy Data
reported similar to Tepezza Phase 3: May 2022 volunteers • Active TED • CAS ≥4 TED 10mg/kg Data reported • Onset of active TED Q3W x2 August 15 n=6 VRDN-001 symptoms within 12 months n=2 placebo Endpoints reported today:
Planned for 4Q22 • Safety/tolerability TED 20mg/kg medical meeting • Efficacy measures at 6 weeks – Overall responder rate Data expected – Proptosis responder rate TED 3mg/kg 4Q22 – Proptosis change from baseline
– CAS change from baseline NEW: Chronic TED – CAS of 0 or 1 Initiation expected Data expected 4Q22 1H23 POC cohorts– Diplopia resolution 8
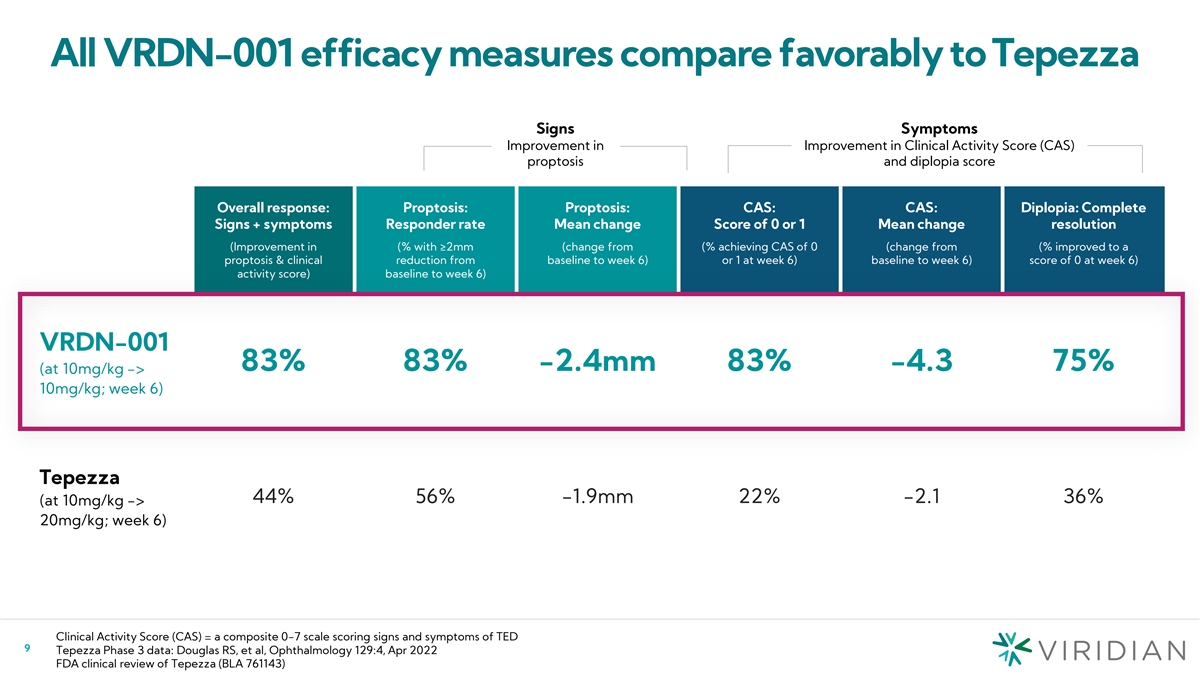
All VRDN-001 efficacy measures compare favorably to Tepezza Signs
Symptoms Improvement in Improvement in Clinical Activity Score (CAS) proptosis and diplopia score Overall response: Proptosis: Proptosis: CAS: CAS: Diplopia: Complete Signs + symptoms Responder rate Mean change Score of 0 or 1 Mean change resolution
(Improvement in (% with ≥2mm (change from (% achieving CAS of 0 (change from (% improved to a proptosis & clinical reduction from baseline to week 6) or 1 at week 6) baseline to week 6) score of 0 at week 6) activity score) baseline to
week 6) VRDN-001 83% 83% -2.4mm 83% -4.3 75% (at 10mg/kg -> 10mg/kg; week 6) Tepezza 44% 56% -1.9mm 22% -2.1 36% (at 10mg/kg -> 20mg/kg; week 6) Clinical Activity Score (CAS) = a composite 0-7 scale scoring signs and symptoms of TED 9 Tepezza
Phase 3 data: Douglas RS, et al, Ophthalmology 129:4, Apr 2022 FDA clinical review of Tepezza (BLA 761143)
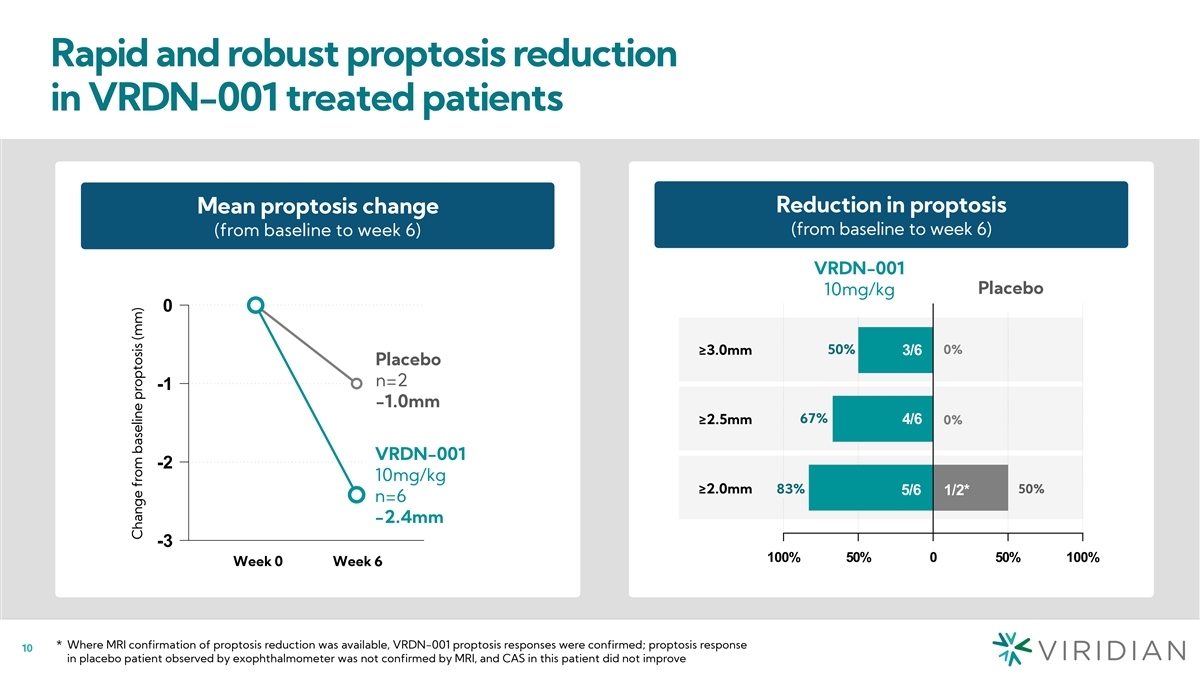
Rapid and robust proptosis reduction in VRDN-001 treated patients
Change in proptosis (mm) Reduction in proptosis Mean proptosis change Reduction in proptosis (from baseline to week 6) (from baseline to week 6) (from baseline to week 6) (from baseline to week 6) VRDN-001 Active Pla Plac cebo ebo 10mg/kg 0 50% 0%
≥3.0mm 3/6 ³ 3.0mm Placebo Placebo n=2 3 -1 n = 2 -1.0mm ≥2.5mm 67% 4/6 ³ 2.5mm 0% VRDN-001 VRDN-001 -2 10mg/kg 10mg/kg ³ 2.0mm ≥2.0mm 83% 50% 5/6 1/2* n = 6 n=6 -2.4mm -3 100% 50% 0 50% 100% W We ee ek k 0 0 W We ee
ek k 6 6 * Where MRI confirmation of proptosis reduction was available, VRDN-001 proptosis responses were confirmed; proptosis response 10 in placebo patient observed by exophthalmometer was not confirmed by MRI, and CAS in this patient did not
improve Change from baseline proptosis (mm)
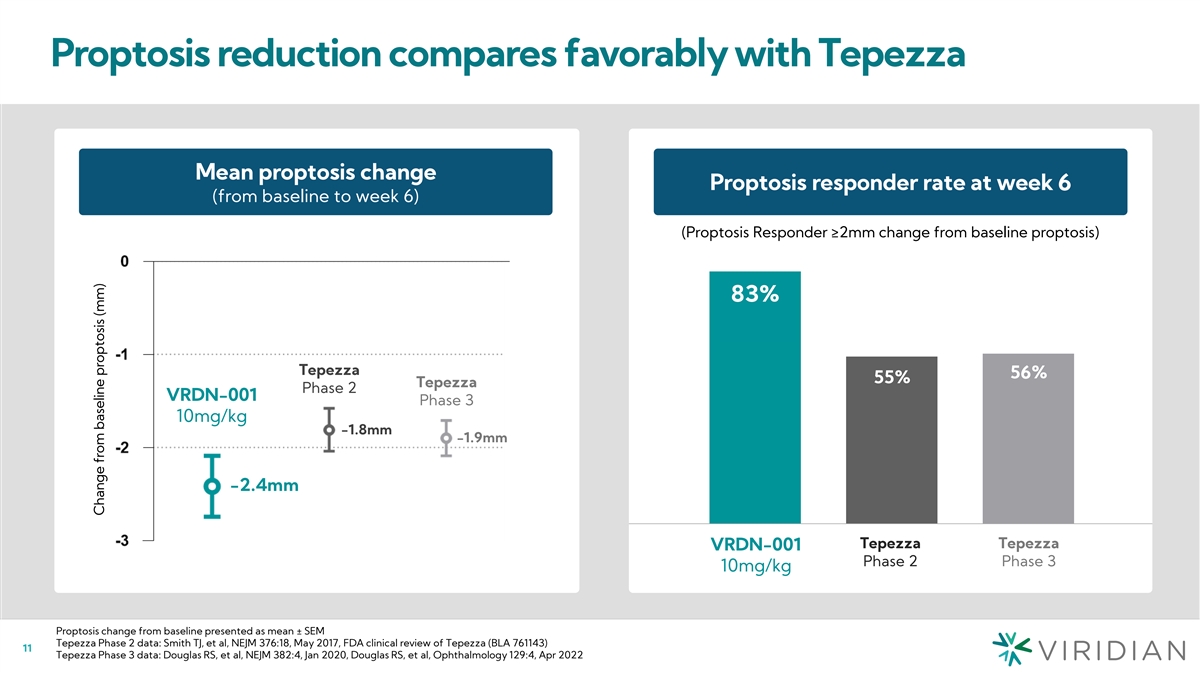
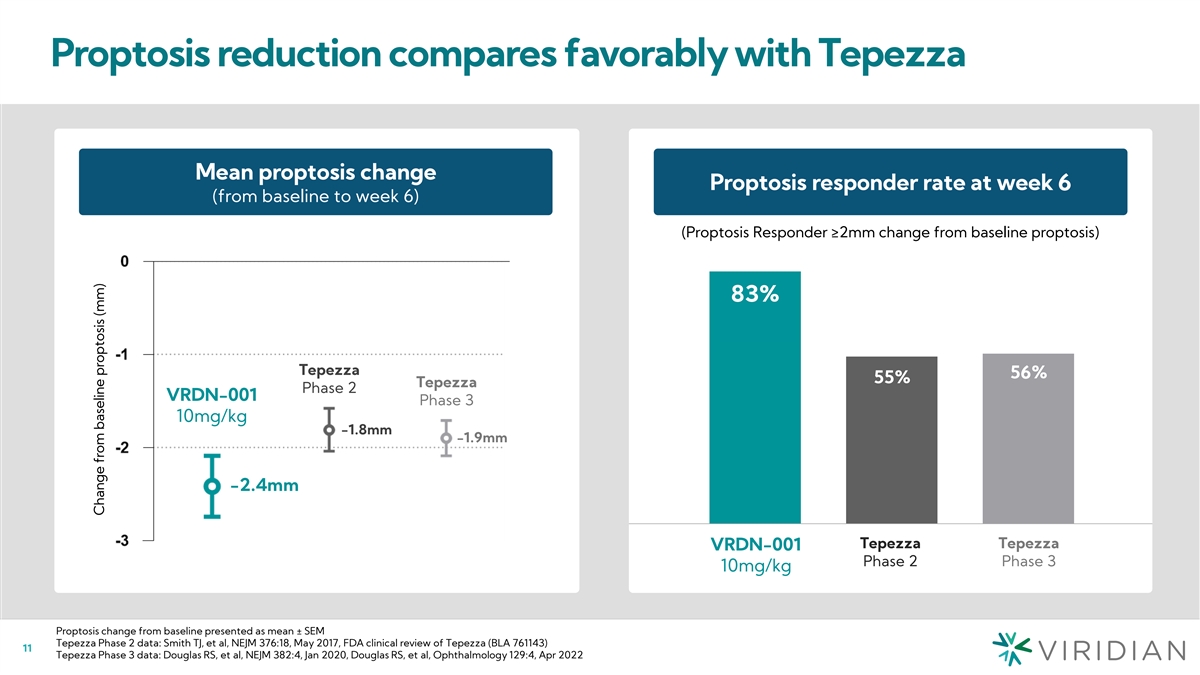
Proptosis reduction compares favorably with Tepezza Mean proptosis
change Proptosis responder rate at week 6 Proptosis response rate at week 6 (from baseline to week 6) (Proptosis Responder ≥2mm change from baseline proptosis) 83% 83% Tepezza 56% 56% 55% 55% Tepezza Phase 2 VRDN-001 Phase 3 10mg/kg -1.8mm
-1.9mm -2.4mm VRDN-001 Tepezza Tepezza Tepezza Tepezza VRDN-001 10mg/kg Phas Phase e 2 2 Phas Phase e 3 3 10mg/kg Proptosis change from baseline presented as mean ± SEM Tepezza Phase 2 data: Smith TJ, et al, NEJM 376:18, May 2017, FDA clinical
review of Tepezza (BLA 761143) 11 Tepezza Phase 3 data: Douglas RS, et al, NEJM 382:4, Jan 2020, Douglas RS, et al, Ophthalmology 129:4, Apr 2022 Change from baseline proptosis (mm)
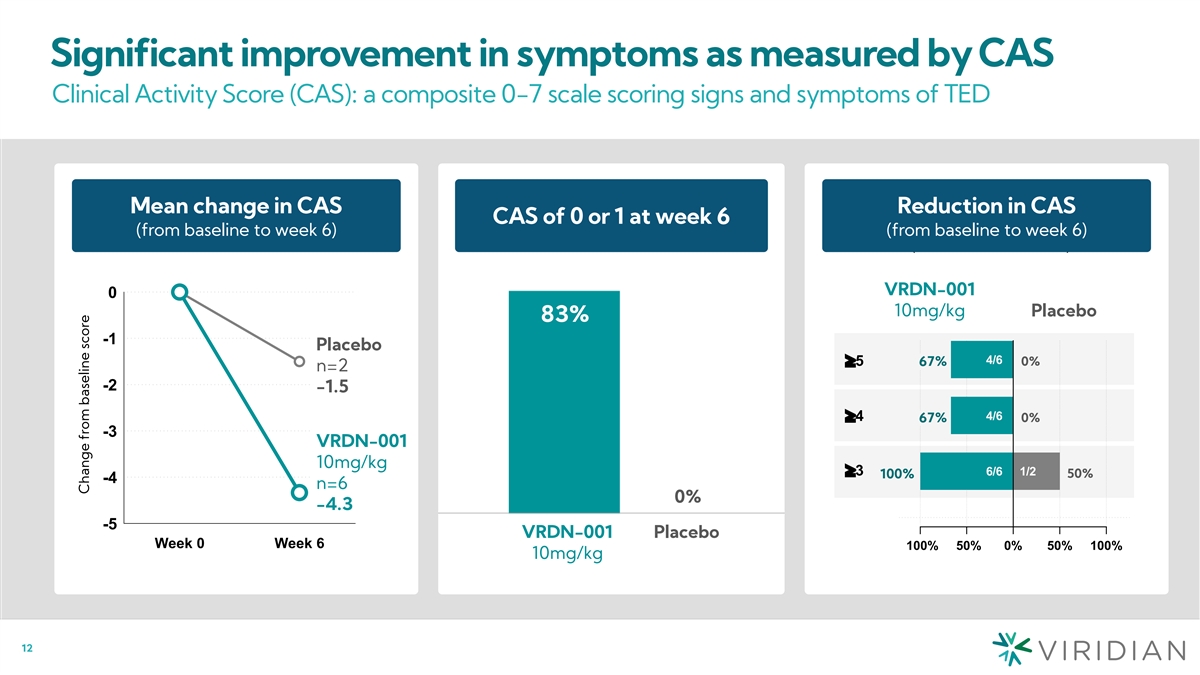
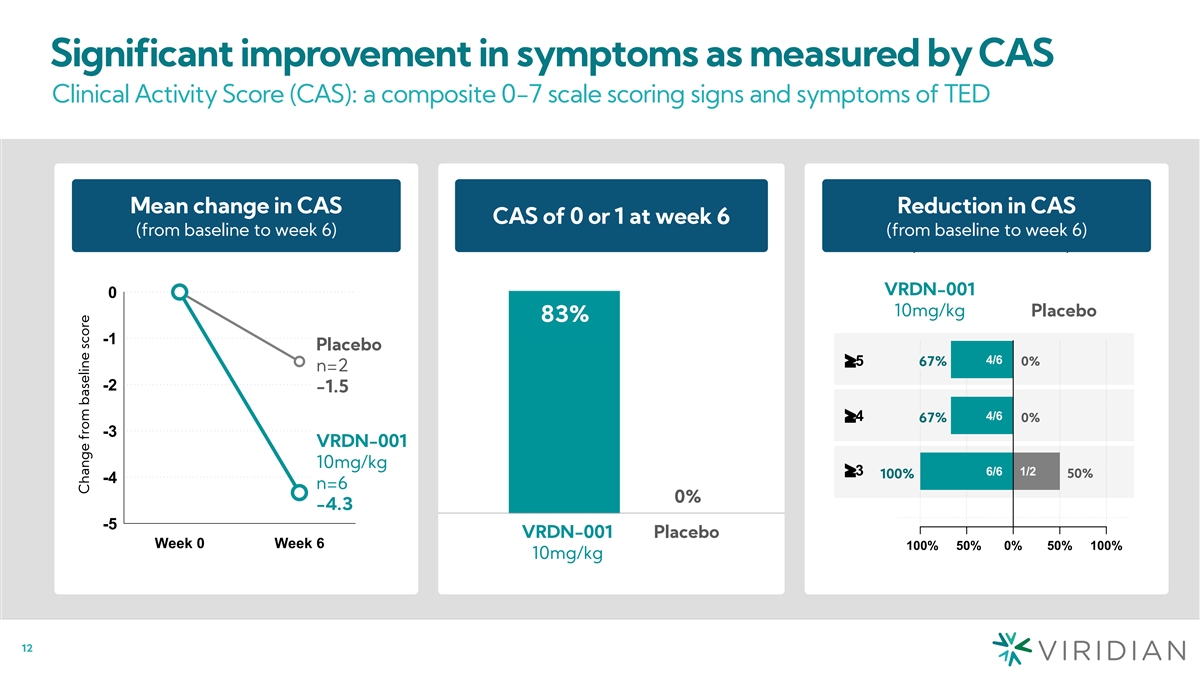
Significant improvement in symptoms as measured by CAS Clinical
Activity Score (CAS): a composite 0-7 scale scoring signs and symptoms of TED Change in CAS score Mean change in CAS Reduction in CAS CAS of 0 or 1 at week 6 (from baseline to week 6) Reduction in CAS score (from baseline to week 6) (from baseline
to week 6) (from baseline to week 6) VRDN-001 0 10mg/kg Placebo 83% -1 Placebo 4/6 ³5 67% 0% n=2 -2 -1.5 4/6 ³4 67% 0% -3 VRDN-001 10mg/kg ³3 6/6 1/2 50% 100% -4 n=6 0% -4.3 -5 VRDN-001 Placebo Week 0 Week 6 -100% -50% 0% 50% 100%
10mg/kg 12 Change from baseline score
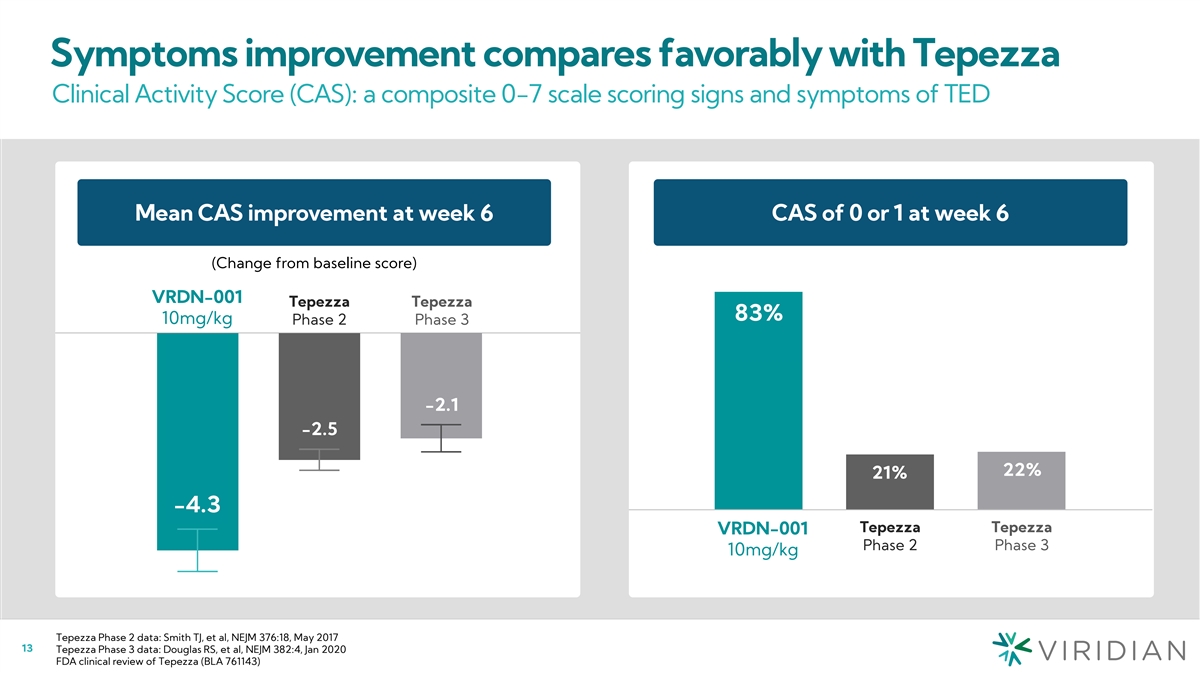
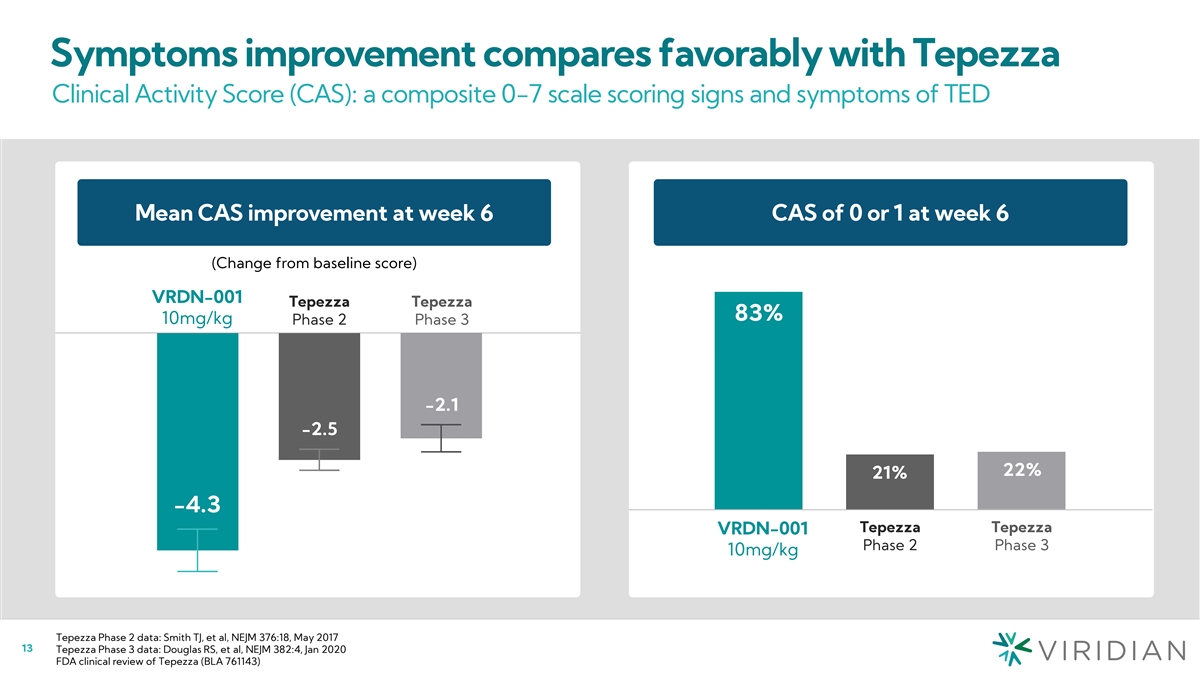
Symptoms improvement compares favorably with Tepezza Clinical Activity
Score (CAS): a composite 0-7 scale scoring signs and symptoms of TED Mean CAS Change CAS of 0 or 1 at week 6 Mean CAS improvement at week 6 CAS of 0 or 1 at week 6 (to week 6) (Change from baseline score) Tepezza VRDN-001 Tepezza VRDN-001 Tepezza
Tepezza 83% Phase 2 10mg/kg Phase 3 83% 10mg/kg Phase 2 Phase 3 -4.3 -2.5 -2.1 -2.1 -2.5 22% 21% 22% 21% -4.3 Tepezza Tepezza VRD VRDN N -0 - 0001 1 Tepezza Tepezza Phase 2 Phase 3 10mg/kg Phase 2 Phase 3 10mg/kg Tepezza Phase 2 data: Smith TJ, et
al, NEJM 376:18, May 2017 13 Tepezza Phase 3 data: Douglas RS, et al, NEJM 382:4, Jan 2020 FDA clinical review of Tepezza (BLA 761143)
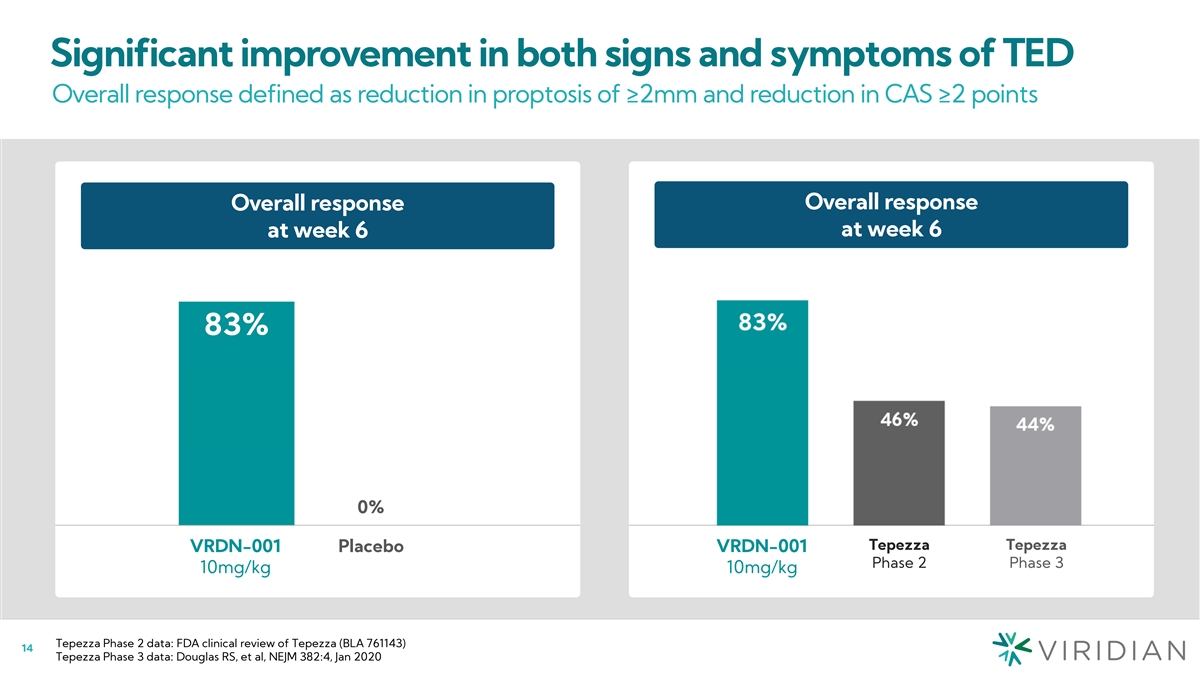
Significant improvement in both signs and symptoms of TED Overall
response defined as reduction in proptosis of ≥2mm and reduction in CAS ≥2 points Overall response Overall response Overall response at week 6 at week 6 at week 6 (% responder) 83% 83% 3 5/6 0% 0% Tepezza Tepezza VRDN-001 Placebo
VRDN-001 VRDN-001 Placebo Phase 2 Phase 3 10mg/kg 10mg/kg 10mg/kg Tepezza Phase 2 data: FDA clinical review of Tepezza (BLA 761143) 14 Tepezza Phase 3 data: Douglas RS, et al, NEJM 382:4, Jan 2020
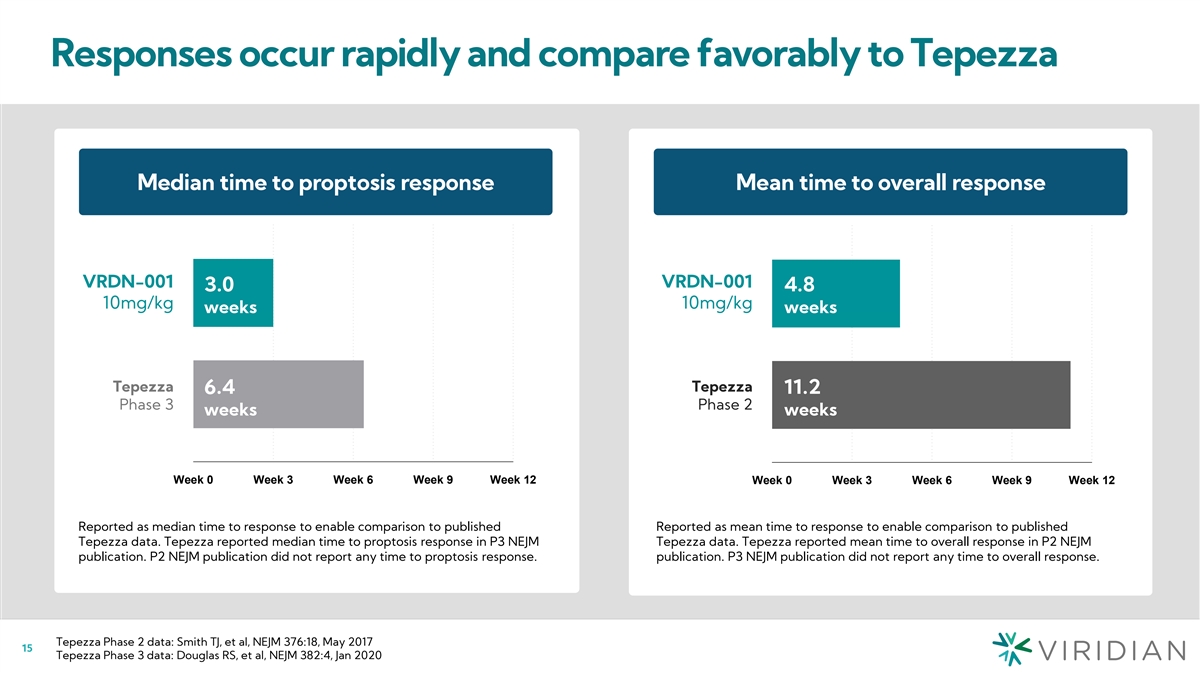
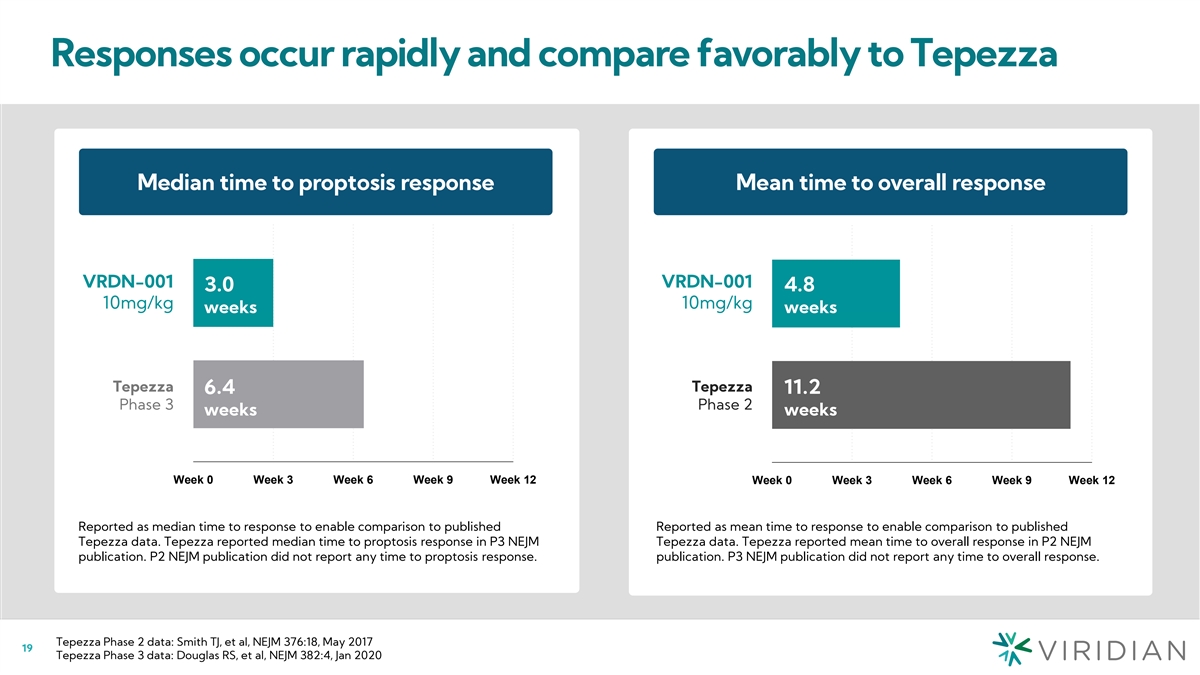
Responses occur rapidly and compare favorably to Tepezza Mean time to
response (weeks) Median time to proptosis response Mean time to overall response Mean time to response (weeks) VRDN-001 VRDN-001 VRDN-001 VRDN-001 3.0 4.8 3.0 4.8 10mg/kg 10mg/kg 10mg/kg 10mg/kg weeks weeks Tepez Tepezzz aa Tepezza Tepezza 6.4 11.2
6.4 11.2 Phase 3 Phase 2 Phase 3 Phase 2 weeks weeks Week 0 Week 3 Week 6 Week 9 Week 12 Week 0 Week 3 Week 6 Week 9 Week 12 Reported as median time to response to enable comparison to published Reported as mean time to response to enable comparison
to published Tepezza data. Tepezza reported median time to proptosis response in P3 NEJM Tepezza data. Tepezza reported mean time to overall response in P2 NEJM publication. P2 NEJM publication did not report any time to proptosis response.
publication. P3 NEJM publication did not report any time to overall response. Tepezza Phase 2 data: Smith TJ, et al, NEJM 376:18, May 2017 15 Tepezza Phase 3 data: Douglas RS, et al, NEJM 382:4, Jan 2020
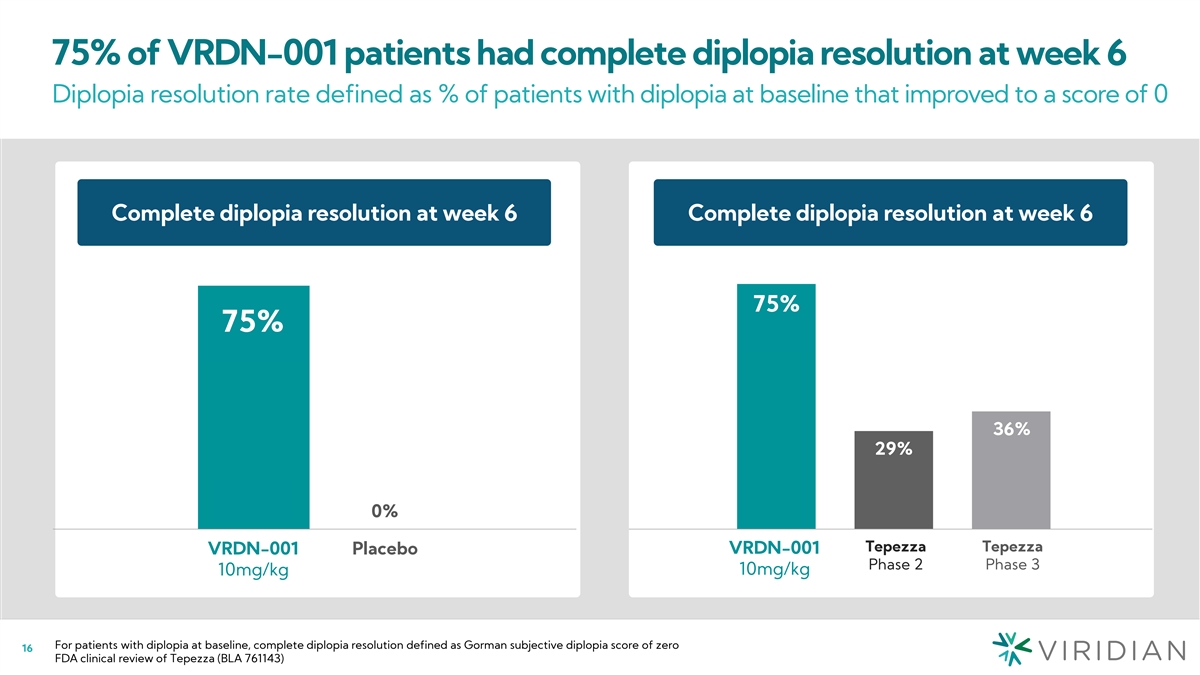
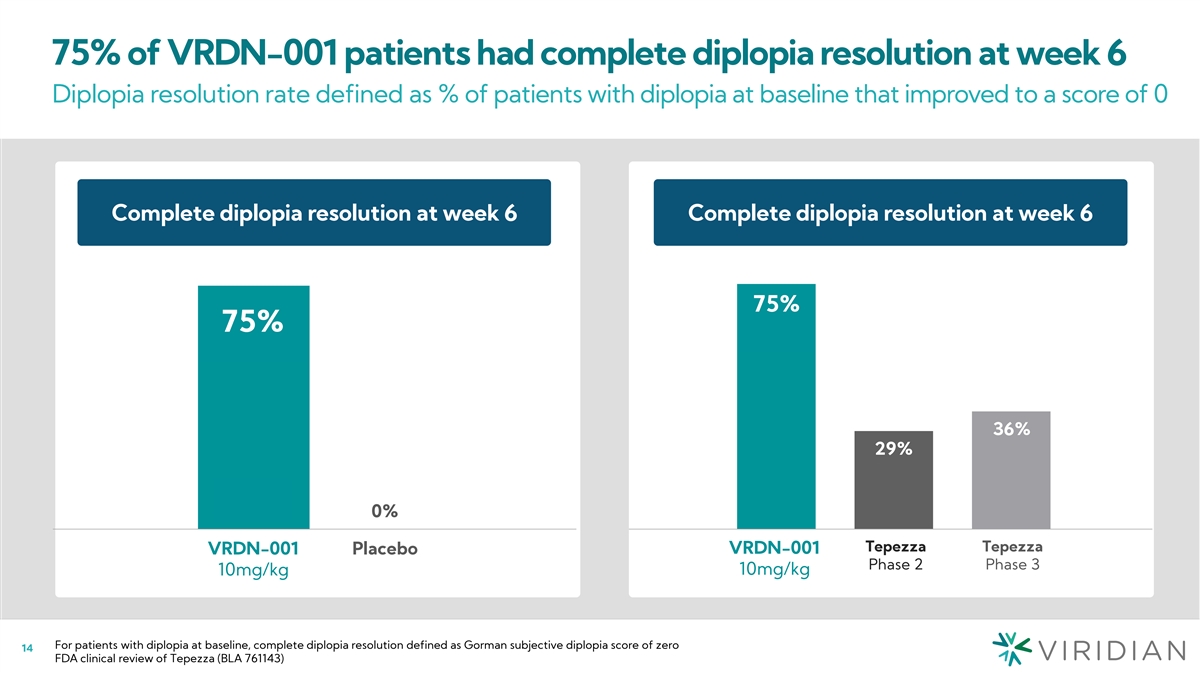
75% of VRDN-001 patients had complete diplopia resolution at week 6
Diplopia resolution rate defined as % of patients with diplopia at baseline that improved to a score of 0 Diplopia resolution vs. Tepezza Complete diplopia resolution at week 6 Complete dip( l% op rie as r pe os no de lu rs t)ion at week 6 *Diplopia
resolution (dg) 75% 75% 75% 75% 36% 36% 30% 29% 0% 0% 3/4 0/1 Tepezza Tepez Tepezzz aa V Tepez RDN-0z 01 a VRDN-001 VRDN-001 Placebo VRDN-001 Placebo Phase 2 Phase 3 10mg/kg Phase 2 Phase 3 10mg/kg 10mg/k 10mg/kg g For patients with diplopia at
baseline, complete diplopia resolution defined as Gorman subjective diplopia score of zero 16 FDA clinical review of Tepezza (BLA 761143)
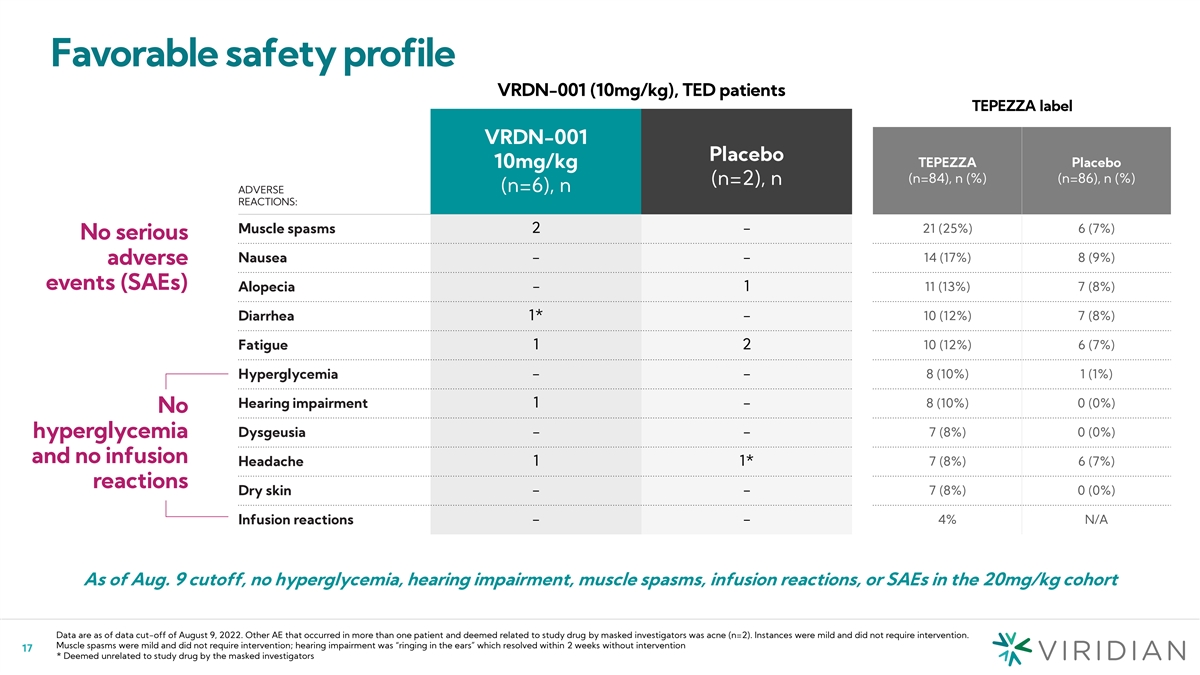
Favorable safety profile VRDN-001 (10mg/kg), TED patients TEPEZZA label
VRDN-001 Placebo TEPEZZA Placebo 10mg/kg (n=84), n (%) (n=86), n (%) (n=2), n (n=6), n ADVERSE REACTIONS: 21 (25%) 6 (7%) Muscle spasms 2 - No serious Nausea - - 14 (17%) 8 (9%) adverse events (SAEs) Alopecia - 1 11 (13%) 7 (8%) 1* - 10 (12%) 7 (8%)
Diarrhea Fatigue 1 2 10 (12%) 6 (7%) Hyperglycemia - - 8 (10%) 1 (1%) Hearing impairment 1 - 8 (10%) 0 (0%) No 7 (8%) 0 (0%) Dysgeusia - - hyperglycemia and no infusion Headache 1 1* 7 (8%) 6 (7%) reactions Dry skin - - 7 (8%) 0 (0%) - - 4% N/A
Infusion reactions As of Aug. 9 cutoff, no hyperglycemia, hearing impairment, muscle spasms, infusion reactions, or SAEs in the 20mg/kg cohort Data are as of data cut-off of August 9, 2022. Other AE that occurred in more than one patient and deemed
related to study drug by masked investigators was acne (n=2). Instances were mild and did not require intervention. Muscle spasms were mild and did not require intervention; hearing impairment was “ringing in the ears” which resolved
within 2 weeks without intervention 17 * Deemed unrelated to study drug by the masked investigators
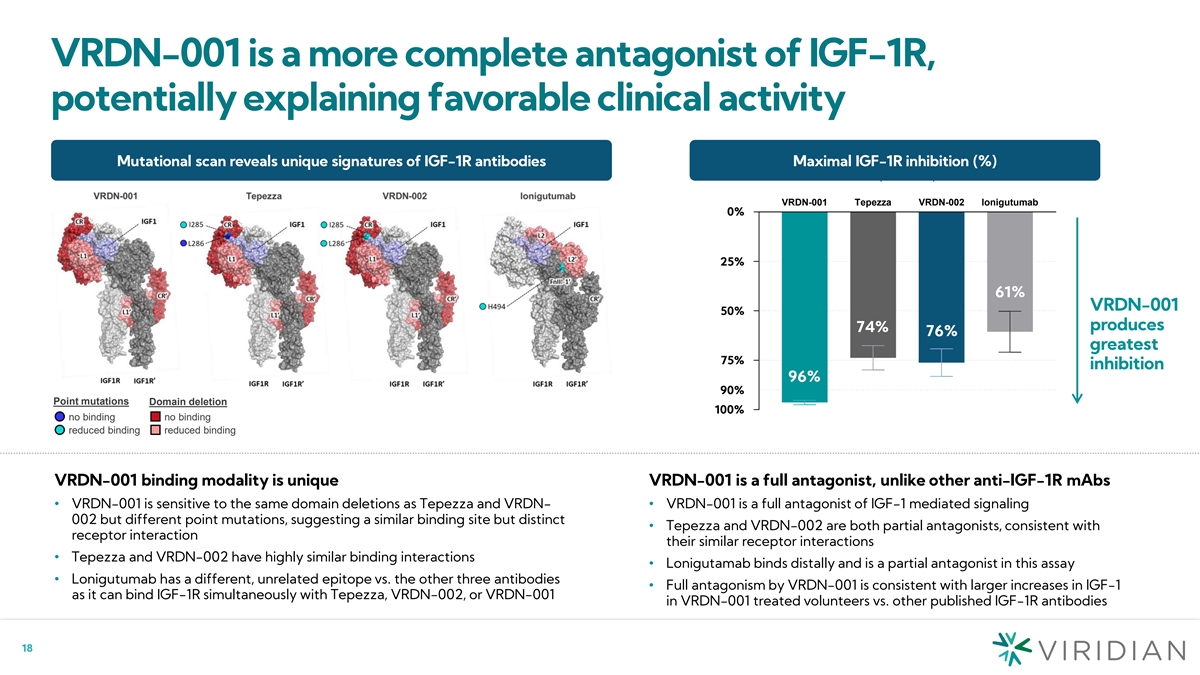
VRDN-001 is a more complete antagonist of IGF-1R, potentially
explaining favorable clinical activity Mutational scan reveals unique signatures of IGF-1R antibodies Maximal IGF-1R inhibition (%) Residual IGF-1R activity (% Inhibition) VRDN-001 Tepezza VRDN-002 lonigutumab 10% 00% 4% 26% 24% 39% 25 7% 5% 61%
VRDN-001 50 5% 0% produces 74% 76% greatest 75 2% 5% inhibition 96% 10% 90% Point mutations Domain deletion 100% 0% no binding no binding reduced binding reduced binding VRDN-001 binding modality is unique VRDN-001 is a full antagonist, unlike other
anti-IGF-1R mAbs • VRDN-001 is sensitive to the same domain deletions as Tepezza and VRDN-• VRDN-001 is a full antagonist of IGF-1 mediated signaling 002 but different point mutations, suggesting a similar binding site but distinct
• Tepezza and VRDN-002 are both partial antagonists, consistent with receptor interaction their similar receptor interactions • Tepezza and VRDN-002 have highly similar binding interactions • Lonigutamab binds distally and is a
partial antagonist in this assay • Lonigutumab has a different, unrelated epitope vs. the other three antibodies • Full antagonism by VRDN-001 is consistent with larger increases in IGF-1 as it can bind IGF-1R simultaneously with
Tepezza, VRDN-002, or VRDN-001 in VRDN-001 treated volunteers vs. other published IGF-1R antibodies 18
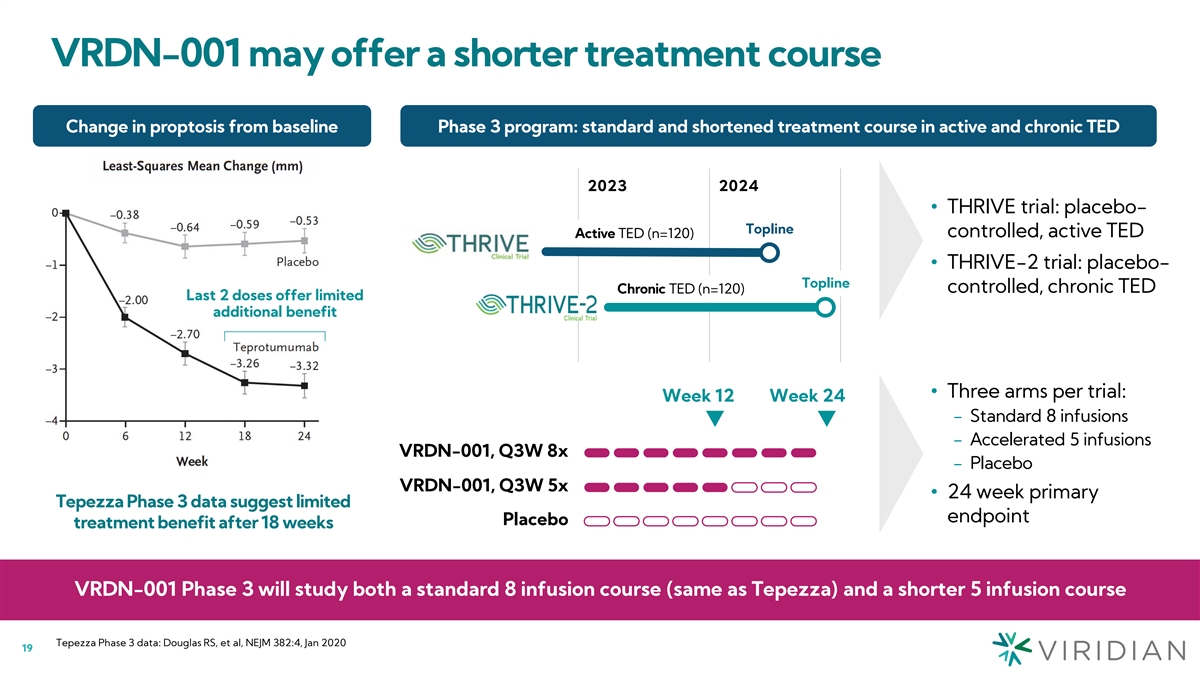
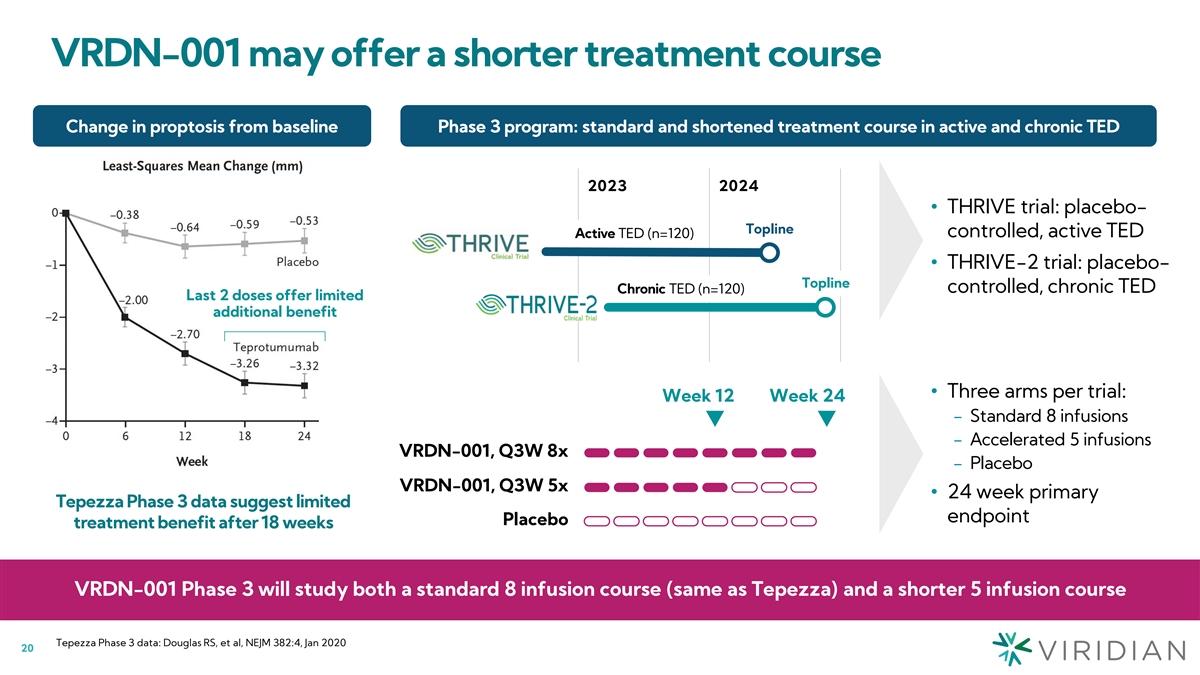
VRDN-001 may offer a shorter treatment course Change in proptosis from
baseline Phase 3 program: standard and shortened treatment course in active and chronic TED 2023 2024 • THRIVE trial: placebo- Topline controlled, active TED Active TED (n=120) • THRIVE-2 trial: placebo- Topline controlled, chronic TED
Chronic TED (n=120) Last 2 doses offer limited additional benefit • Three arms per trial: Week 12 Week 24 − Standard 8 infusions − Accelerated 5 infusions VRDN-001, Q3W 8x − Placebo VRDN-001, Q3W 5x • 24 week primary
Tepezza Phase 3 data suggest limited endpoint Placebo treatment benefit after 18 weeks VRDN-001 Phase 3 will study both a standard 8 infusion course (same as Tepezza) and a shorter 5 infusion course Tepezza Phase 3 data: Douglas RS, et al, NEJM
382:4, Jan 2020 19
VRDN-002 Potential best-in-class subcutaneous treatment for TED
20
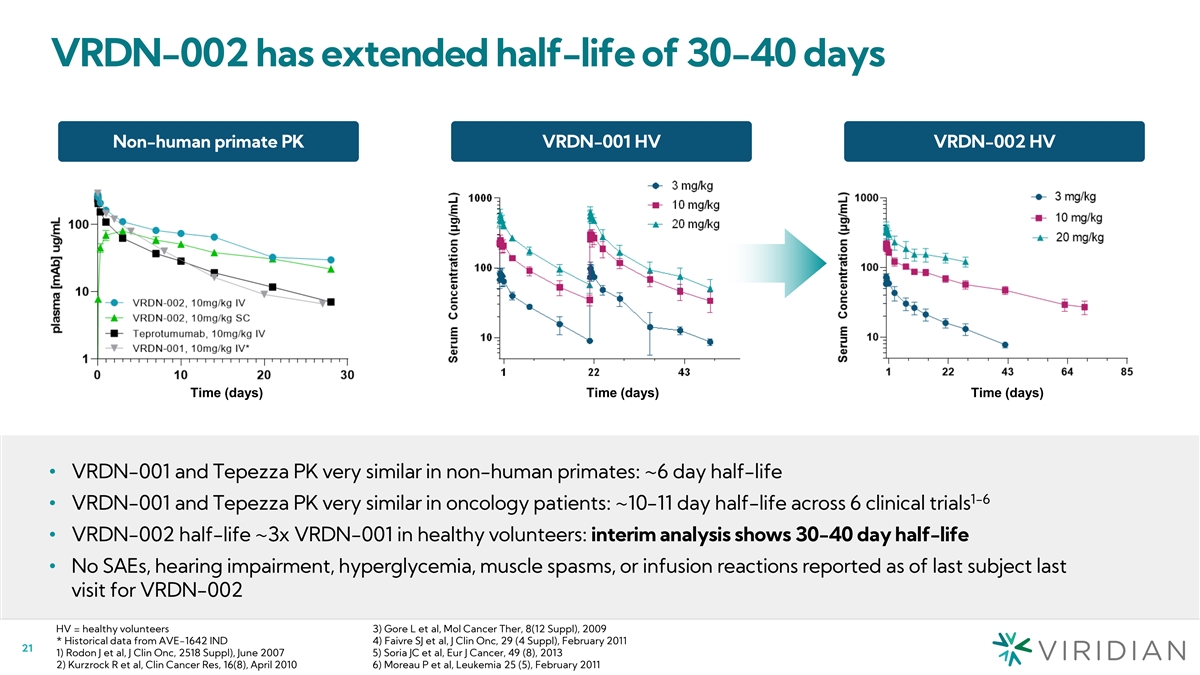
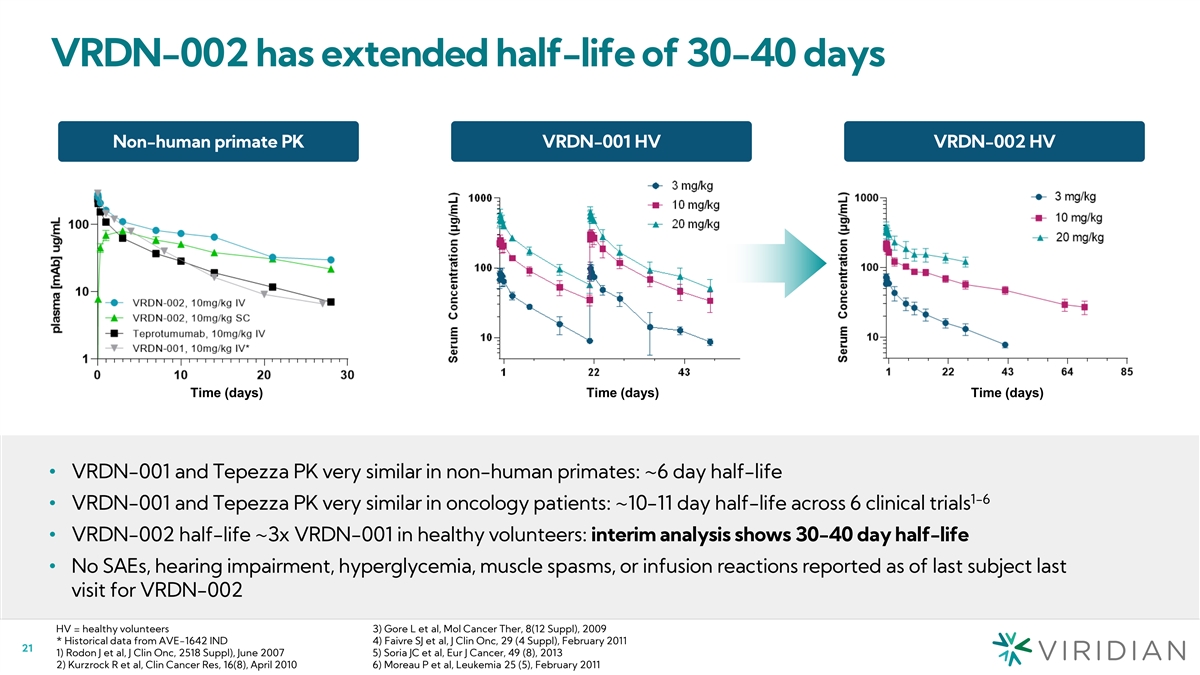
VRDN-002 has extended half-life of 30-40 days Non-human primate PK
VRDN-001 HV VRDN-002 HV Time (days) Time (days) Time (days) • VRDN-001 and Tepezza PK very similar in non-human primates: ~6 day half-life 1-6 • VRDN-001 and Tepezza PK very similar in oncology patients: ~10-11 day half-life across 6
clinical trials • VRDN-002 half-life ~3x VRDN-001 in healthy volunteers: interim analysis shows 30-40 day half-life • No SAEs, hearing impairment, hyperglycemia, muscle spasms, or infusion reactions reported as of last subject last visit
for VRDN-002 HV = healthy volunteers 3) Gore L et al, Mol Cancer Ther, 8(12 Suppl), 2009 * Historical data from AVE-1642 IND 4) Faivre SJ et al, J Clin Onc, 29 (4 Suppl), February 2011 21 1) Rodon J et al, J Clin Onc, 2518 Suppl), June 2007 5) Soria
JC et al, Eur J Cancer, 49 (8), 2013 2) Kurzrock R et al, Clin Cancer Res, 16(8), April 2010 6) Moreau P et al, Leukemia 25 (5), February 2011
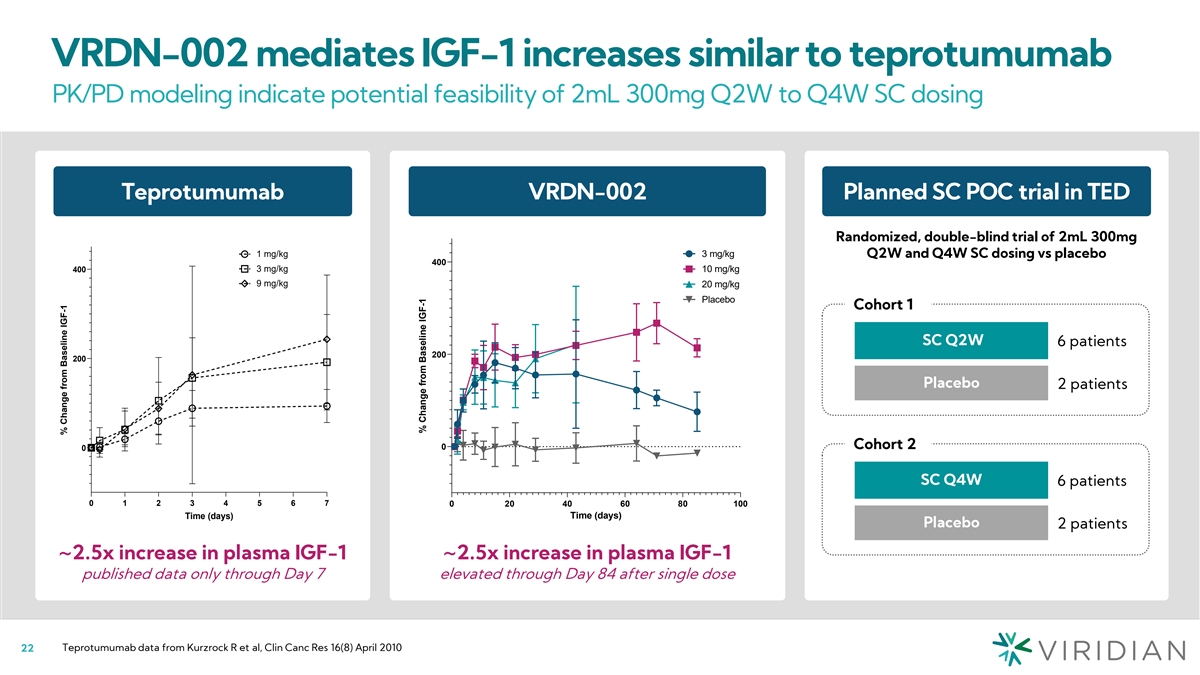
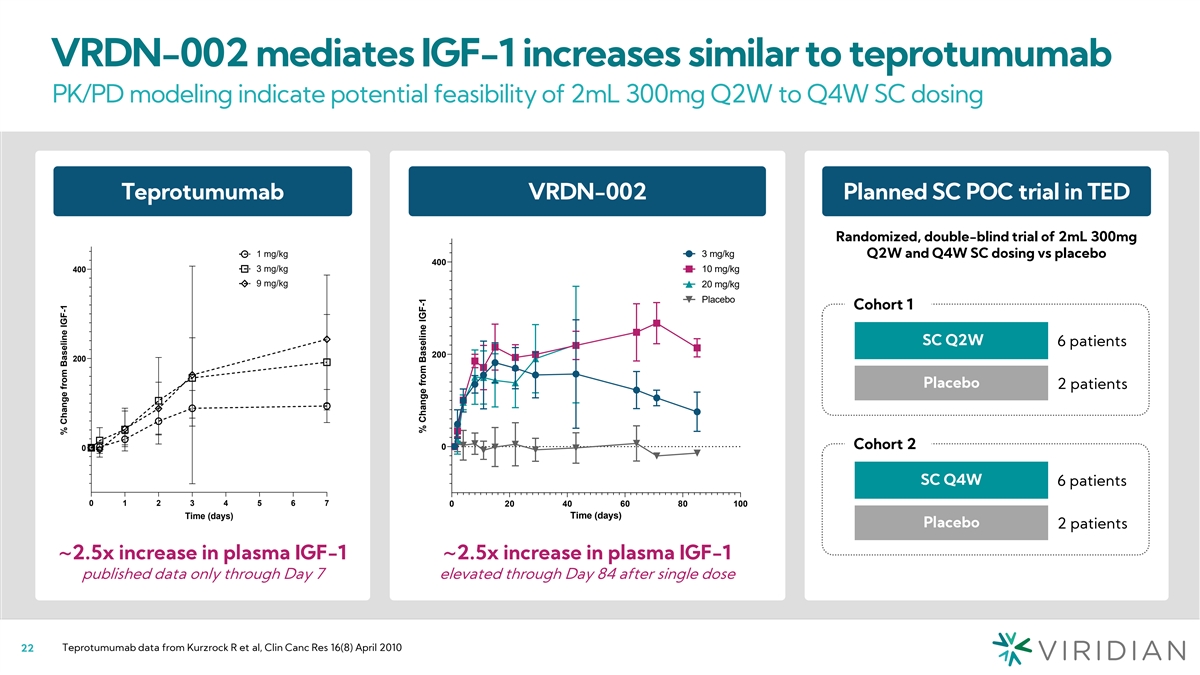
VRDN-002 mediates IGF-1 increases similar to teprotumumab PK/PD
modeling indicate potential feasibility of 2mL 300mg Q2W to Q4W SC dosing % Change from Baseline of IGF-1 in normal healthy volunteers Teprotumumab VRDN-002 Planned SC POC trial in TED Presumed Placebo Removed Randomized, double-blind trial of 2mL
300mg 1 mg/kg 3 mg/kg Q2W and Q4W SC dosing vs placebo 400 400 3 mg/kg 10 mg/kg 9 mg/kg 20 mg/kg Placebo Cohort 1 SC Q2W 6 patients 200 200 Placebo 2 patients Cohort 2 0 0 SC Q4W 6 patients 0 1 2 3 4 5 6 7 0 20 40 60 80 100 Time (days) Time (days)
Placebo 2 patients ~2.5x increase in plasma IGF-1 ~2.5x increase in plasma IGF-1 published data only through Day 7 elevated through Day 84 after single dose Teprotumumab data from Kurzrock R et al, Clin Canc Res 16(8) April 2010 22 % Change from
Baseline IGF-1 % Change from Baseline IGF-1

Global TED development plan To rapidly enter US and EU markets in both
active and chronic TED 23
Corporate objectives in TED: Build a market-leading franchise 2 1
Launch Rapidly follow potential best- IV launch with in-class IV TED potential best- therapy in US in-class SC TED and EU therapy 24
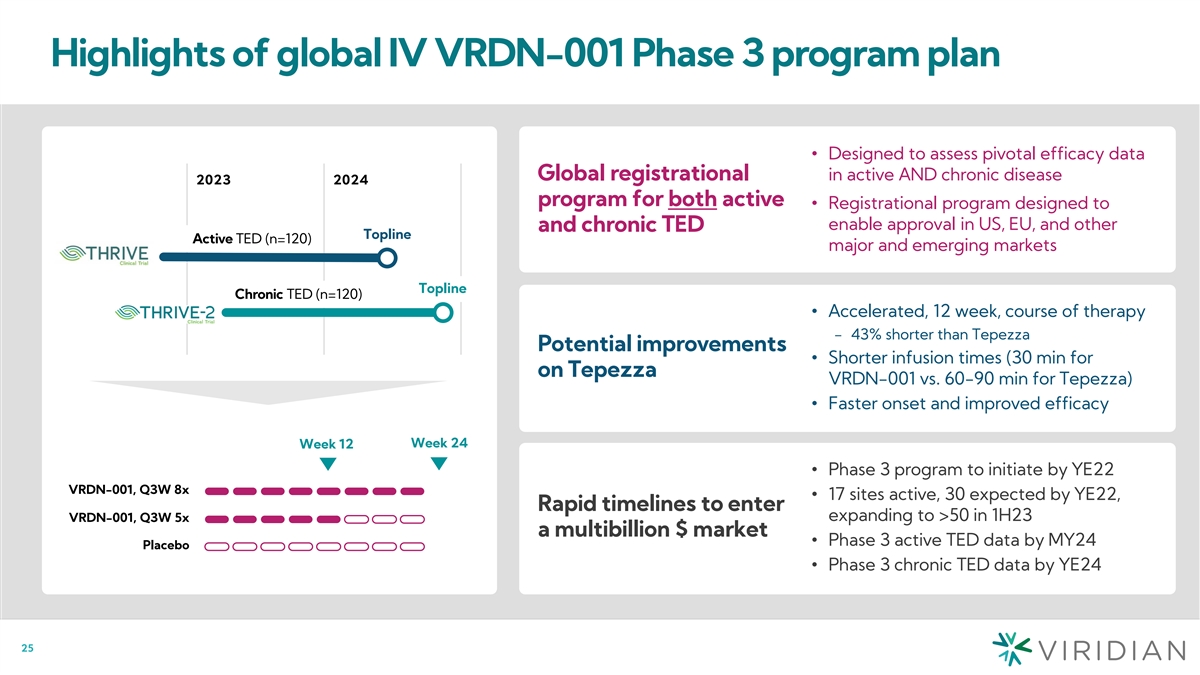
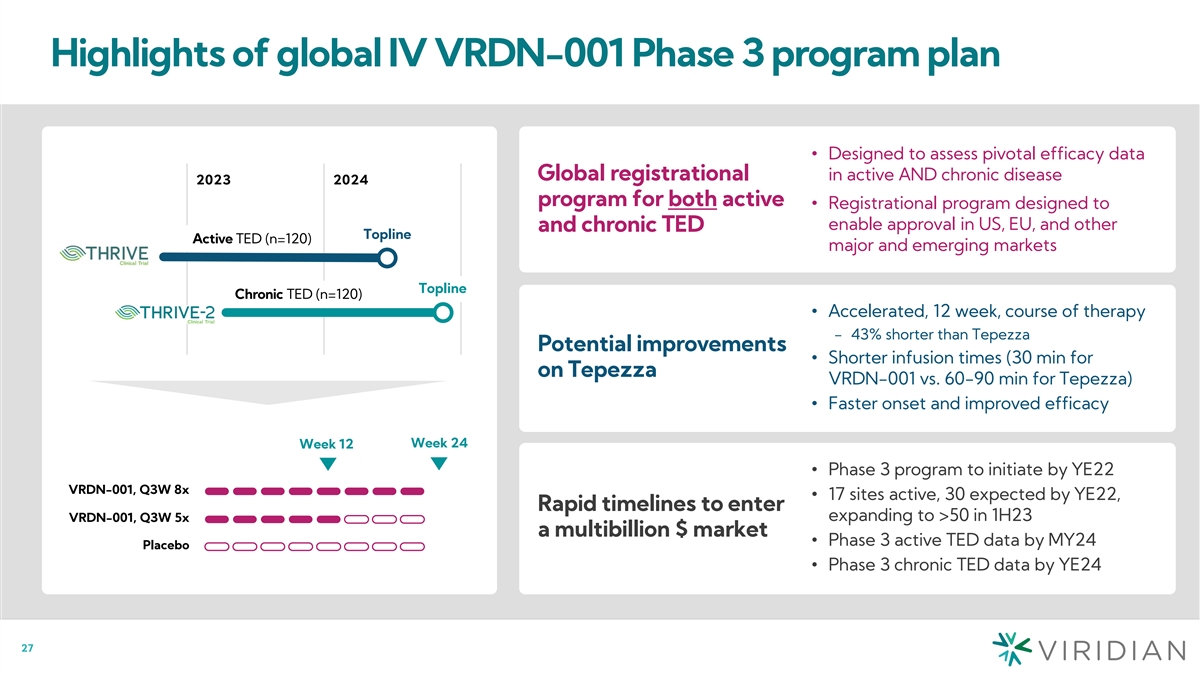
Highlights of global IV VRDN-001 Phase 3 program plan • Designed
to assess pivotal efficacy data Global registrational in active AND chronic disease 2023 2024 program for both active • Registrational program designed to enable approval in US, EU, and other and chronic TED Topline Active TED (n=120) major
and emerging markets Topline Chronic TED (n=120) • Accelerated, 12 week, course of therapy − 43% shorter than Tepezza Potential improvements • Shorter infusion times (30 min for on Tepezza VRDN-001 vs. 60-90 min for Tepezza)
• Faster onset and improved efficacy Week 24 Week 12 • Phase 3 program to initiate by YE22 VRDN-001, Q3W 8x • 17 sites active, 30 expected by YE22, Rapid timelines to enter expanding to >50 in 1H23 VRDN-001, Q3W 5x a
multibillion $ market • Phase 3 active TED data by MY24 Placebo • Phase 3 chronic TED data by YE24 25
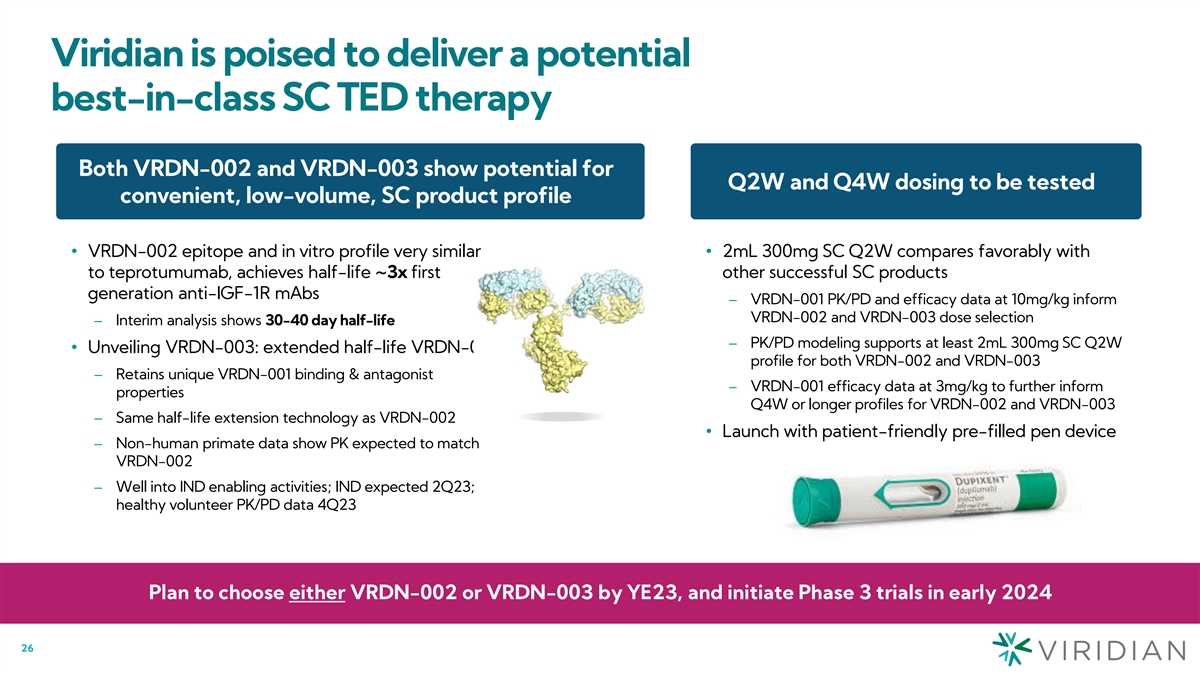
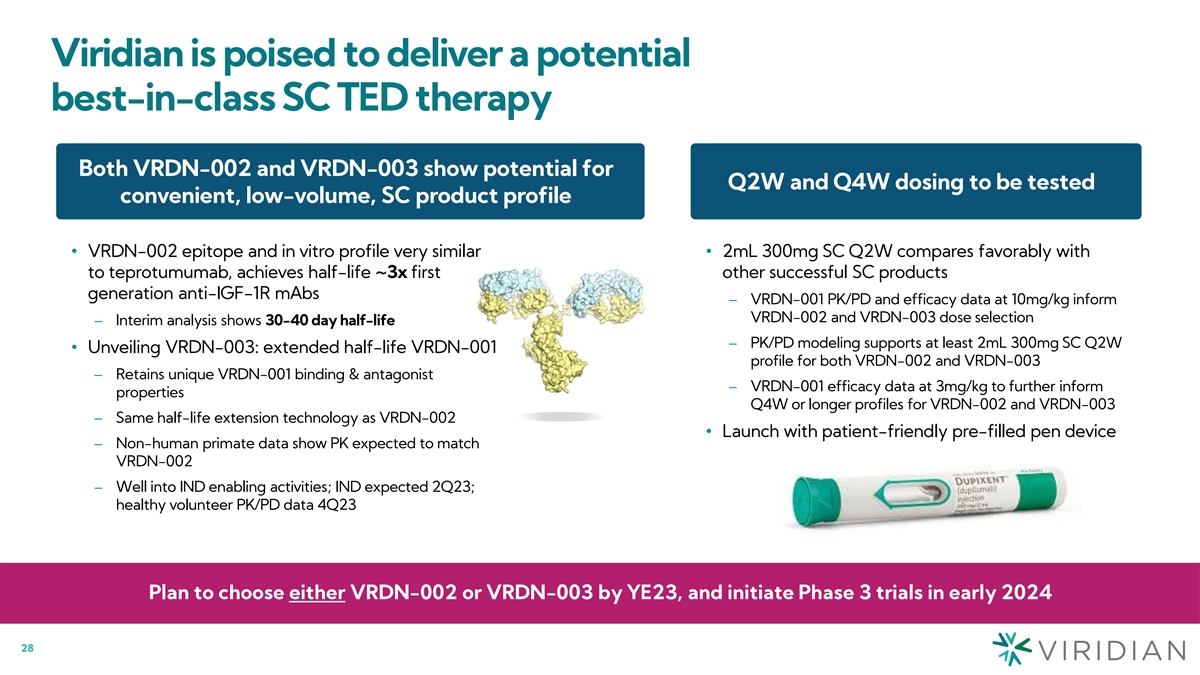
Viridian is poised to deliver a potential best-in-class SC TED therapy
Both VRDN-002 and VRDN-003 show potential for Q2W and Q4W dosing to be tested convenient, low-volume, SC product profile • VRDN-002 epitope and in vitro profile very similar • 2mL 300mg SC Q2W compares favorably with to teprotumumab,
achieves half-life ~3x first other successful SC products generation anti-IGF-1R mAbs – VRDN-001 PK/PD and efficacy data at 10mg/kg inform VRDN-002 and VRDN-003 dose selection – Interim analysis shows 30-40 day half-life – PK/PD
modeling supports at least 2mL 300mg SC Q2W • Unveiling VRDN-003: extended half-life VRDN-001 profile for both VRDN-002 and VRDN-003 – Retains unique VRDN-001 binding & antagonist – VRDN-001 efficacy data at 3mg/kg to further
inform properties Q4W or longer profiles for VRDN-002 and VRDN-003 – Same half-life extension technology as VRDN-002 • Launch with patient-friendly pre-filled pen device – Non-human primate data show PK expected to match VRDN-002
– Well into IND enabling activities; IND expected 2Q23; healthy volunteer PK/PD data 4Q23 Plan to choose either VRDN-002 or VRDN-003 by YE23, and initiate Phase 3 trials in early 2024 26
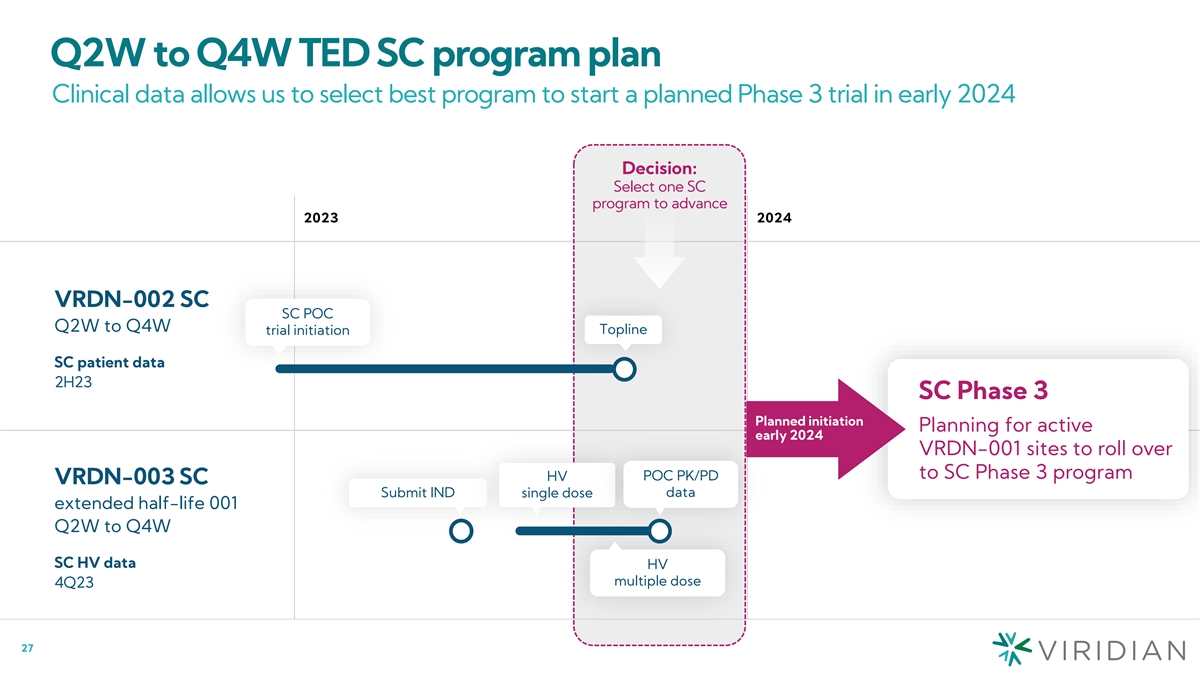
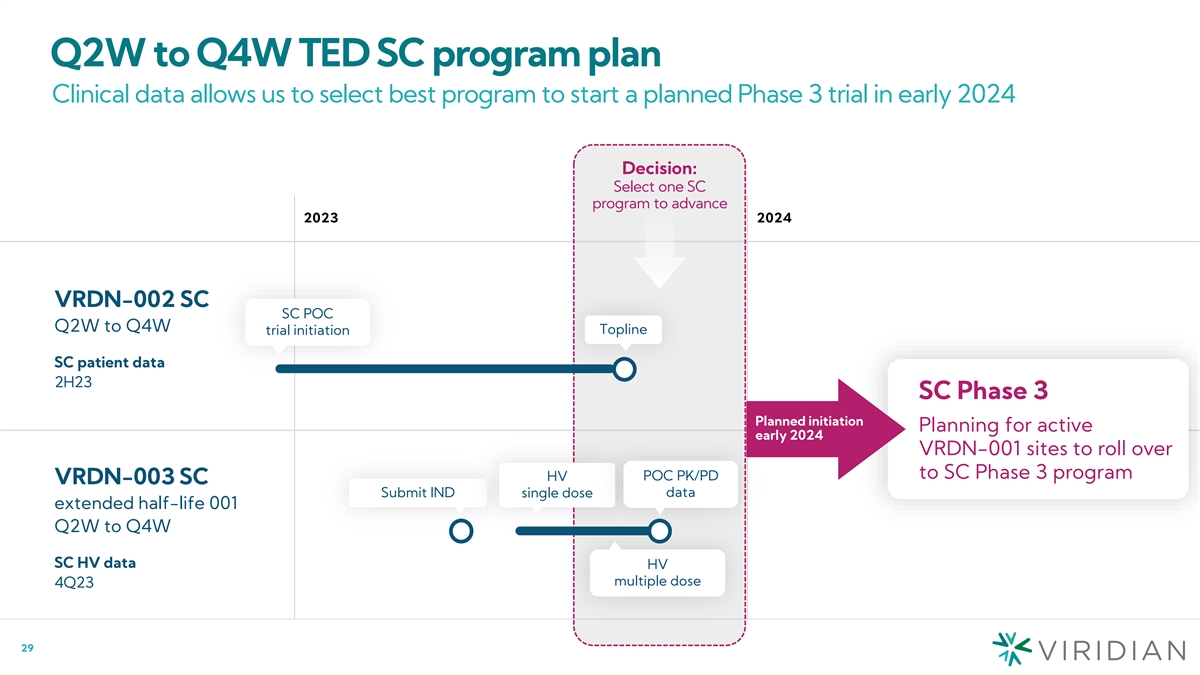
Q2W to Q4W TED SC program plan Clinical data allows us to select best
program to start a planned Phase 3 trial in early 2024 Decision: Select one SC program to advance 2023 2024 VRDN-002 SC SC POC Q2W to Q4W Topline trial initiation SC patient data 2H23 SC Phase 3 Planned initiation Planning for active early 2024
VRDN-001 sites to roll over to SC Phase 3 program POC PK/PD HV VRDN-003 SC Submit IND single dose data extended half-life 001 Q2W to Q4W SC HV data HV multiple dose 4Q23 27
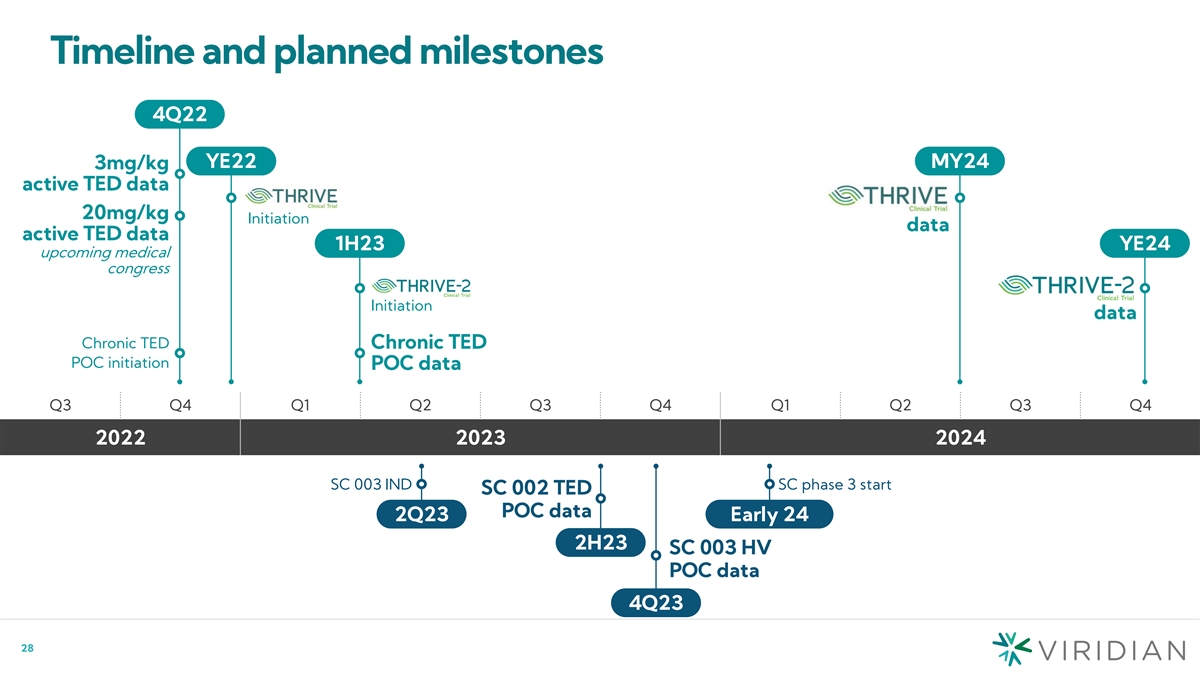
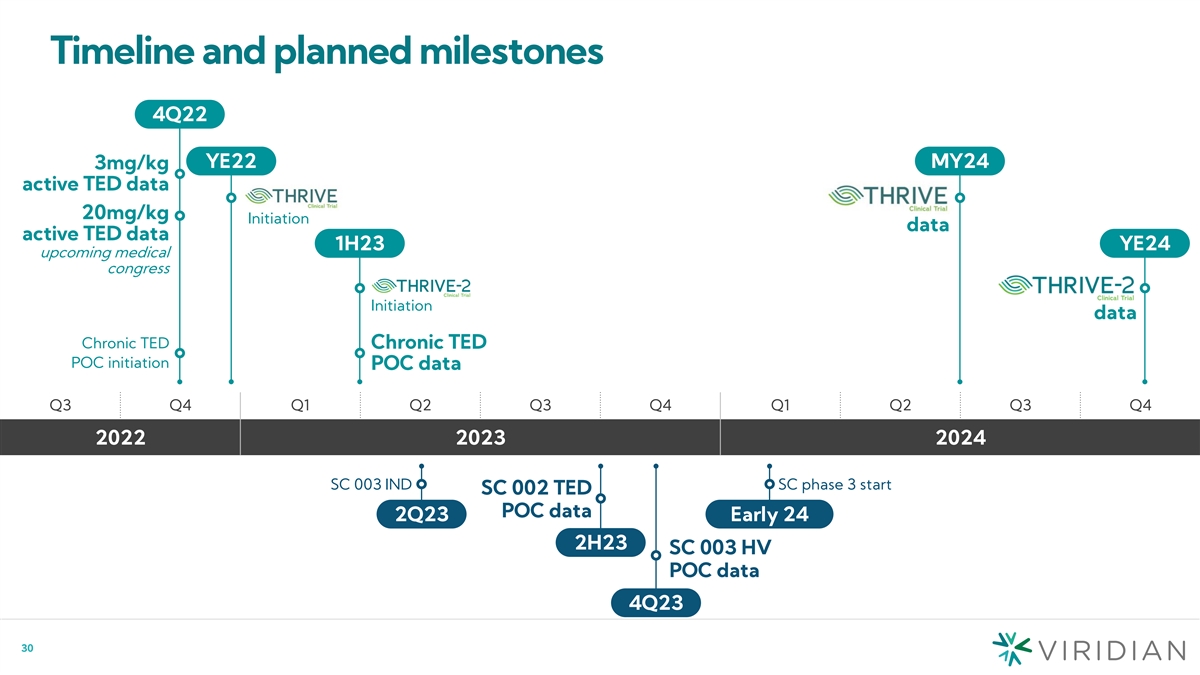
Timeline and planned milestones 4Q22 YE22 MY24 3mg/kg active TED data
20mg/kg Initiation data active TED data 1H23 YE24 upcoming medical congress Initiation data Chronic TED Chronic TED POC initiation POC data Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 2022 2023 2024 SC 003 IND SC phase 3 start SC 002 TED POC data 2Q23 Early 24
2H23 SC 003 HV POC data 4Q23 28

Management team Jonathan Violin, Ph.D. President & CEO Vahe Bedian,
Ph.D. Chief Scientist Kristian Humer Chief Financial & Business Officer Barrett Katz, M.D. Chief Medical Officer Carrie Melvin Chief Operating Officer Deepa Rajagopalan, M.D. SVP, New Product and Portfolio Development Janielle Newland SVP, Human
Resources Lara Meisner, J.D. SVP, General Counsel Angela She, Ph.D. VP, R&D Operations 29 29
Investment highlights 1) Large opportunity in TED and beyond •
Initial focus on thyroid eye disease (TED) – Global Phase 3 registrational program in active and chronic TED to launch by YE22 to support BLA and MAA • TED is a $3.5B+ market opportunity with Europe to provide additional upside •
Multiple assets for next wave of growth beyond TED 2) Best-in-class IGF-1R antibodies for TED • VRDN-001 (IV): Positive topline data from the 10mg/kg cohort in the ongoing Phase 1/2 clinical trial for TED • Phase 3 THRIVE registrational
program to launch by YE22, with topline data in MY24 • VRDN-002 (SC): Extended half-life of 30-40 days supports potential best-in-class low-volume Q2W or Q4W SC profile for TED 3) VRDN-001 shows significant improvement in signs & symptoms
of TED in just 6 weeks • 83% proptosis responder rate • 83% of patients achieved maximal or near-maximal therapeutic effect on the Clinical Activity Score (CAS) • 83% overall responder rate • 75% resolution of diplopia 4)
Strong financial position • Cash, cash equivalents and short-term investments were $161.2M as of June 30, 2022 • $75M credit facility ($5M drawn) • Cash runway into 2024 1 2 • 43M total common shares outstanding on an as
converted basis – implied market cap of $632M (1) As of July 1, 2022, Viridian had approximately 42,909,027 shares of common stock outstanding on an as-converted basis, which included 28,463,980 shares of common stock and approximately
14,445,047 shares of common stock issuable upon the conversion of 193,539 and 23,126 shares of Series A and Series B preferred stock respectively 30 (2) As of August 12, 2022, based on a stock price of $14.73

Corporate Presentation August 2022
Exhibit 99.3 VRDN-001 & VRDN-002 initial clinical data August 15,
2022
Cautionary note regarding forward-looking statements This presentation
contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. These statements may be identified by the use of words such as, but not limited to, anticipate, believe, continue, could, estimate,
expect, intend, may, might, plan, potential, predict, project, should, target, will, or would or other similar terms or expressions that concern our expectations, plans and intentions. Forward-looking statements include, without limitation,
statements regarding our expectations, strategies, plans and intentions. Forward-looking statements are neither historical facts nor assurances of future performance. Instead, they are based on our current beliefs, expectations, and assumptions. New
risks and uncertainties may emerge from time to time, and it is not possible to predict all risks and uncertainties. No representations or warranties (expressed or implied) are made about the accuracy of any such forward-looking statements. Such
forward-looking statements are subject to a number of material risks and uncertainties including but not limited to: the efficacy and safety of VRDN-001 and VRDN-002 for the treatment of TED; the relationship between the results from the positive
data from the ongoing Phase 1/2 clinical trial of VRDN-001 and the first-in-human Phase 1 clinical trial of VRDN-002 and results of future of ongoing clinical trials; the timing, progress and plans for our ongoing and future research and clinical
development programs; trial protocols for ongoing clinical trials, including the clinical trials for VRDN-001 and VRDN 002; expectations regarding the timing for data, including the expected timing of additional data from the ongoing Phase 1/2
clinical trial of VRDN-001 and the first-in-human Phase 1 clinical trial of VRDN-002; uncertainty and potential delays related to clinical drug development; the duration and impact of regulatory delays in our clinical programs; the timing of and our
ability to obtain and maintain regulatory approvals for our therapeutic candidates, including VRDN-001 and VRDN-002; manufacturing risks; competition from other therapies or products; other matters that could affect the sufficiency of existing cash,
cash equivalents and short-term investments to fund operations; our financial position and its projected cash runway; our future operating results and financial performance; the clinical utility of our therapeutic candidates and our intellectual
property position; the timing of pre-clinical and clinical trial activities and reporting results from same; the effects from the COVID-19 pandemic on our research, development and business activities and operating results, including those risks set
forth under the caption Risk Factors in our Annual Report on Form 10-K filed with the Securities and Exchange Commission (SEC) on March 11, 2022 and other subsequent disclosure documents filed with the SEC. The forward-looking statements in this
presentation represent our views as of the date of this presentation. Neither we, nor our affiliates, advisors, or representatives, undertake any obligation to publicly update or revise any forward-looking statement, whether as a result of new
information, future events or otherwise, except as required by law. These forward-looking statements should not be relied upon as representing our views as of any date subsequent to the date of this presentation. This presentation also contains
estimates and other statistical data made by independent parties and by us relating to market size and other data about our industry. This data involves a number of assumptions and limitations, and you are cautioned not to give undue weight to such
estimates. In addition, projections, assumptions and estimates of our future performance and the future performance of the markets in which we operate are necessarily subject to a high degree of uncertainty and risk. 2
INTRODUCTION 1 Jonathan Violin, Ph.D., President and Chief Executive
Officer Agenda 2 VRDN-001 PROOF OF CONCEPT RESULTS Barrett Katz, M.D., Chief Medical Officer Jonathan Violin, Ph.D. President and Chief Executive Officer Raymond Douglas, M.D., Ph.D., Director, Thyroid Eye Disease Program, Cedars-Sinai Medical
Center 3 Raymond Douglas, M.D., Ph.D. TAKEAWAYS FOR VRDN-001 AND VRDN-002 DATA; PHASE 3 AND SC PLANS Director, Thyroid Eye Disease Program, Cedars-Sinai Medical Center Jonathan Violin, Ph.D., President and Chief Executive Officer 4 Barrett Katz,
M.D. SECOND QUARTER FINANCIALS Chief Medical Officer Kristian Humer, Chief Financial and Business Officer Kristian Humer 5 Chief Financial and Business Officer Q&A Jonathan Violin, Ph.D., President and Chief Executive Officer Raymond Douglas,
M.D., Ph.D., Director, Thyroid Eye Disease Program, Cedars-Sinai Medical Center Barrett Katz, M.D., Chief Medical Officer Kristian Humer, Chief Financial and Business Officer 3 3
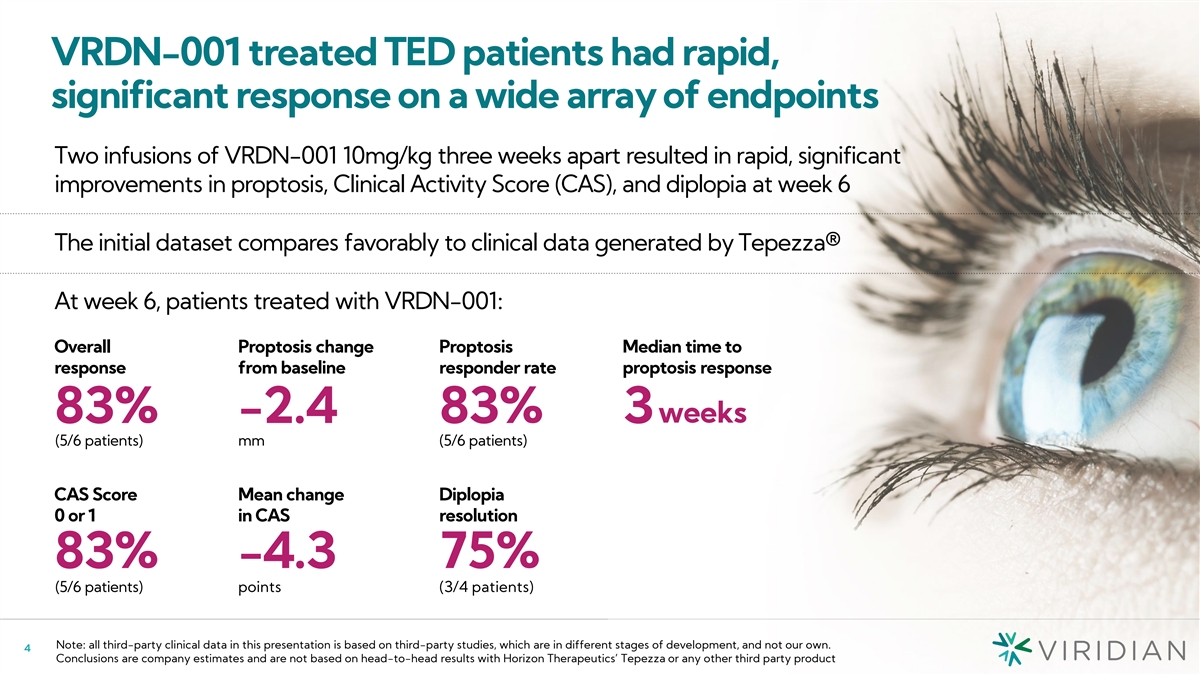
VRDN-001 treated TED patients had rapid, significant response on a wide
array of endpoints Two infusions of VRDN-001 10mg/kg three weeks apart resulted in rapid, significant improvements in proptosis, Clinical Activity Score (CAS), and diplopia at week 6 The initial dataset compares favorably to clinical data generated
by Tepezza® At week 6, patients treated with VRDN-001: Overall Proptosis change Proptosis Median time to response from baseline responder rate proptosis response weeks 83% -2.4 83% 3 (5/6 patients) mm (5/6 patients) CAS Score Mean change
Diplopia 0 or 1 in CAS resolution 83% -4.3 75% (5/6 patients) points (3/4 patients) Note: all third-party clinical data in this presentation is based on third-party studies, which are in different stages of development, and not our own. 4
Conclusions are company estimates and are not based on head-to-head results with Horizon Therapeutics’ Tepezza or any other third party product
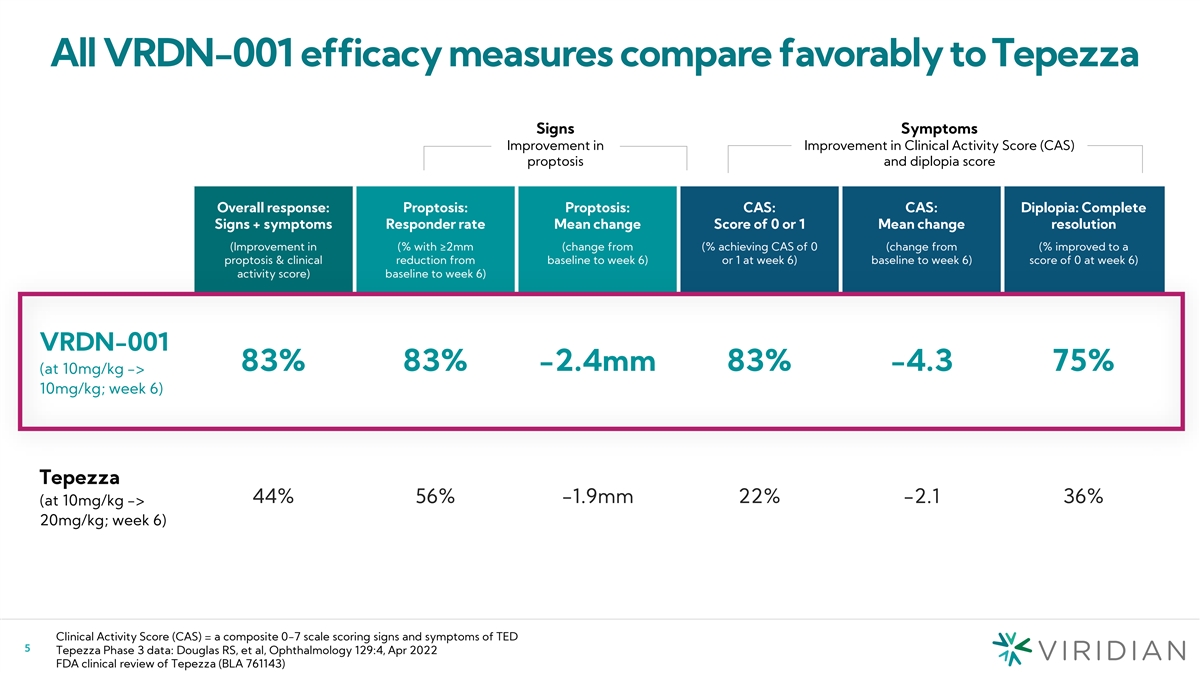
All VRDN-001 efficacy measures compare favorably to Tepezza Signs
Symptoms Improvement in Improvement in Clinical Activity Score (CAS) proptosis and diplopia score Overall response: Proptosis: Proptosis: CAS: CAS: Diplopia: Complete Signs + symptoms Responder rate Mean change Score of 0 or 1 Mean change resolution
(Improvement in (% with ≥2mm (change from (% achieving CAS of 0 (change from (% improved to a proptosis & clinical reduction from baseline to week 6) or 1 at week 6) baseline to week 6) score of 0 at week 6) activity score) baseline to
week 6) VRDN-001 83% 83% -2.4mm 83% -4.3 75% (at 10mg/kg -> 10mg/kg; week 6) Tepezza 44% 56% -1.9mm 22% -2.1 36% (at 10mg/kg -> 20mg/kg; week 6) Clinical Activity Score (CAS) = a composite 0-7 scale scoring signs and symptoms of TED 5 Tepezza
Phase 3 data: Douglas RS, et al, Ophthalmology 129:4, Apr 2022 FDA clinical review of Tepezza (BLA 761143)
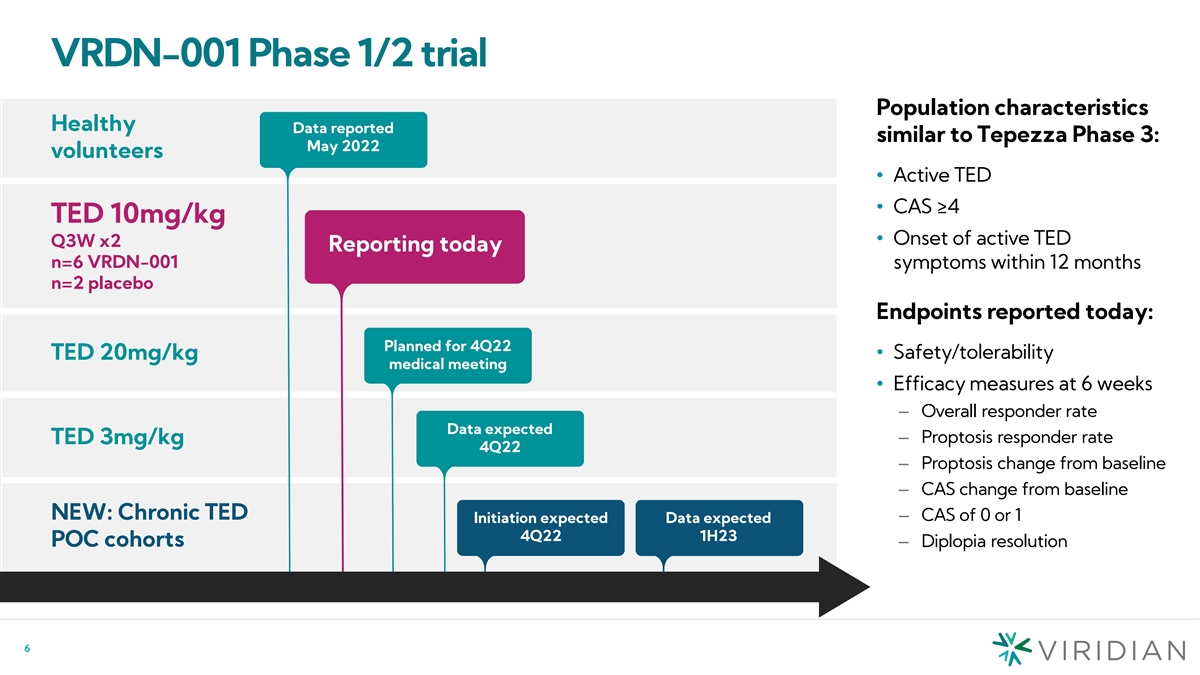
VRDN-001 Phase 1/2 trial Population characteristics Healthy Data
reported similar to Tepezza Phase 3: May 2022 volunteers • Active TED • CAS ≥4 TED 10mg/kg • Onset of active TED Q3W x2 Reporting today n=6 VRDN-001 symptoms within 12 months n=2 placebo Endpoints reported today: Planned for
4Q22 • Safety/tolerability TED 20mg/kg medical meeting • Efficacy measures at 6 weeks – Overall responder rate Data expected – Proptosis responder rate TED 3mg/kg 4Q22 – Proptosis change from baseline – CAS change
from baseline NEW: Chronic TED – CAS of 0 or 1 Initiation expected Data expected 4Q22 1H23 POC cohorts– Diplopia resolution 6
VRDN-001 proof of concept results Raymond Douglas, M.D., Ph.D.,
Director, Thyroid Eye Disease Program, Cedars-Sinai Medical Center 7
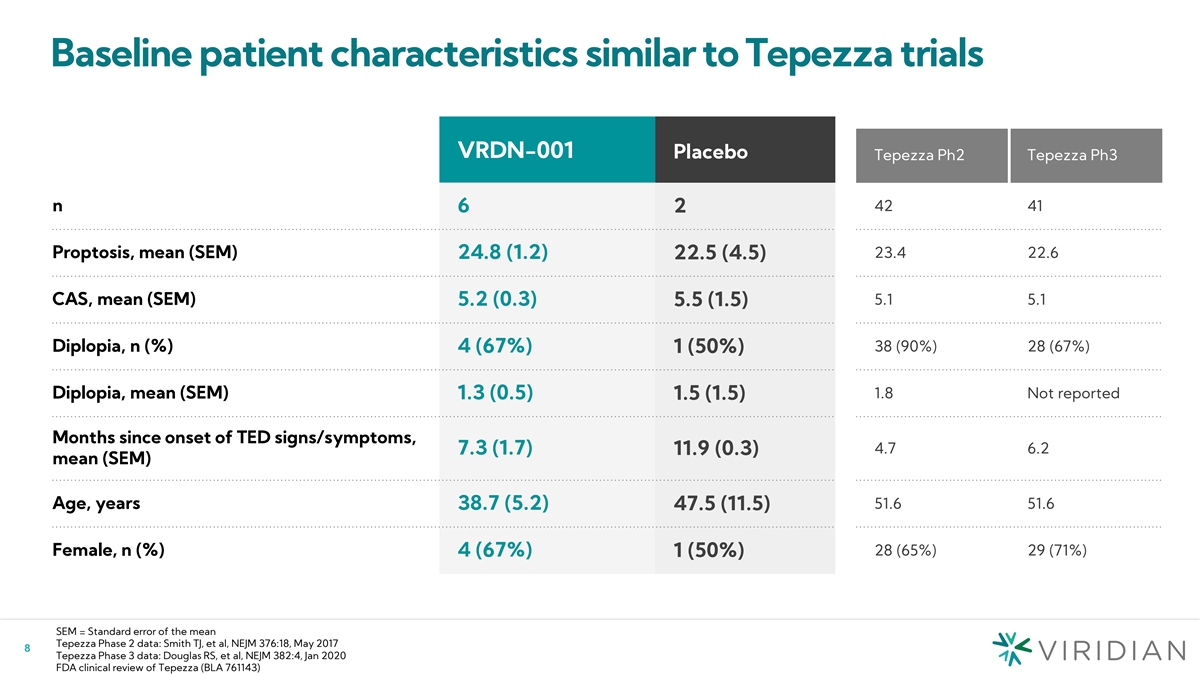
Baseline patient characteristics similar to Tepezza trials VRDN-001
Placebo Tepezza Ph2 Tepezza Ph3 n 42 41 6 2 23.4 22.6 Proptosis, mean (SEM) 24.8 (1.2) 22.5 (4.5) CAS, mean (SEM) 5.1 5.1 5.2 (0.3) 5.5 (1.5) 38 (90%) 28 (67%) Diplopia, n (%) 4 (67%) 1 (50%) Diplopia, mean (SEM) 1.8 Not reported 1.3 (0.5) 1.5 (1.5)
Months since onset of TED signs/symptoms, 4.7 6.2 7.3 (1.7) 11.9 (0.3) mean (SEM) Age, years 51.6 51.6 38.7 (5.2) 47.5 (11.5) Female, n (%) 4 (67%) 28 (65%) 29 (71%) 1 (50%) SEM = Standard error of the mean Tepezza Phase 2 data: Smith TJ, et al,
NEJM 376:18, May 2017 8 Tepezza Phase 3 data: Douglas RS, et al, NEJM 382:4, Jan 2020 FDA clinical review of Tepezza (BLA 761143)
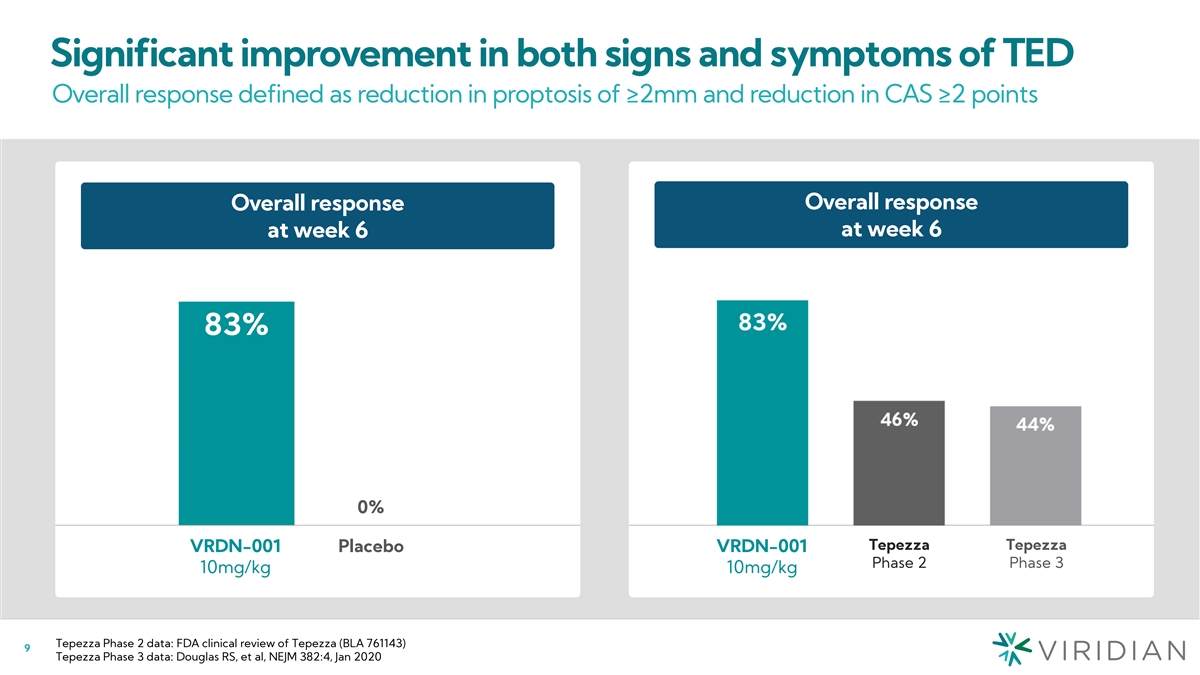
Significant improvement in both signs and symptoms of TED Overall
response defined as reduction in proptosis of ≥2mm and reduction in CAS ≥2 points Overall response Overall response Overall response at week 6 at week 6 at week 6 (% responder) 83% 83% 3 5/6 0% 0% Tepezza Tepezza VRDN-001 Placebo
VRDN-001 VRDN-001 Placebo Phase 2 Phase 3 10mg/kg 10mg/kg 10mg/kg Tepezza Phase 2 data: FDA clinical review of Tepezza (BLA 761143) 9 Tepezza Phase 3 data: Douglas RS, et al, NEJM 382:4, Jan 2020
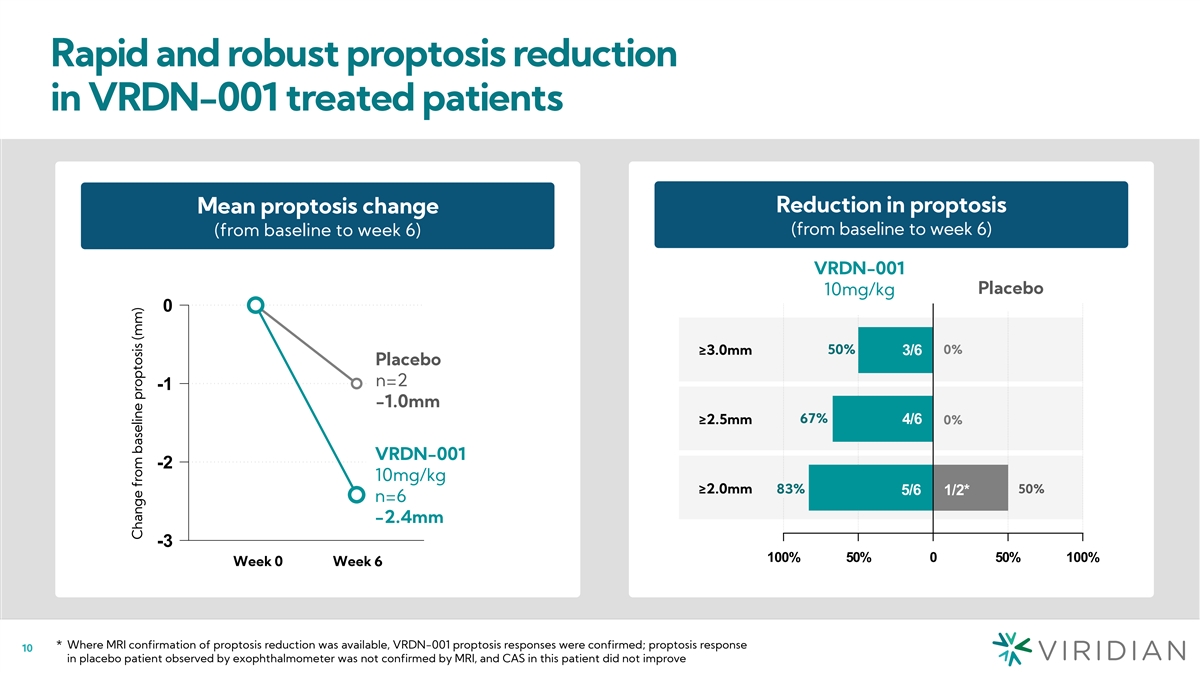
Rapid and robust proptosis reduction in VRDN-001 treated patients
Change in proptosis (mm) Reduction in proptosis Mean proptosis change Reduction in proptosis (from baseline to week 6) (from baseline to week 6) (from baseline to week 6) (from baseline to week 6) VRDN-001 Active Pla Plac cebo ebo 10mg/kg 0 50% 0%
≥3.0mm 3/6 ³ 3.0mm Placebo Placebo n=2 3 -1 n = 2 -1.0mm ≥2.5mm 67% 4/6 ³ 2.5mm 0% VRDN-001 VRDN-001 -2 10mg/kg 10mg/kg ³ 2.0mm ≥2.0mm 83% 50% 5/6 1/2* n = 6 n=6 -2.4mm -3 100% 50% 0 50% 100% W We ee ek k 0 0 W We ee
ek k 6 6 * Where MRI confirmation of proptosis reduction was available, VRDN-001 proptosis responses were confirmed; proptosis response 10 in placebo patient observed by exophthalmometer was not confirmed by MRI, and CAS in this patient did not
improve Change from baseline proptosis (mm)
Proptosis reduction compares favorably with Tepezza Mean proptosis
change Proptosis responder rate at week 6 Proptosis response rate at week 6 (from baseline to week 6) (Proptosis Responder ≥2mm change from baseline proptosis) 83% 83% Tepezza 56% 56% 55% 55% Tepezza Phase 2 VRDN-001 Phase 3 10mg/kg -1.8mm
-1.9mm -2.4mm VRDN-001 Tepezza Tepezza Tepezza Tepezza VRDN-001 10mg/kg Phas Phase e 2 2 Phas Phase e 3 3 10mg/kg Proptosis change from baseline presented as mean ± SEM Tepezza Phase 2 data: Smith TJ, et al, NEJM 376:18, May 2017, FDA clinical
review of Tepezza (BLA 761143) 11 Tepezza Phase 3 data: Douglas RS, et al, NEJM 382:4, Jan 2020, Douglas RS, et al, Ophthalmology 129:4, Apr 2022 Change from baseline proptosis (mm)
Significant improvement in symptoms as measured by CAS Clinical
Activity Score (CAS): a composite 0-7 scale scoring signs and symptoms of TED Change in CAS score Mean change in CAS Reduction in CAS CAS of 0 or 1 at week 6 (from baseline to week 6) Reduction in CAS score (from baseline to week 6) (from baseline
to week 6) (from baseline to week 6) VRDN-001 0 10mg/kg Placebo 83% -1 Placebo 4/6 ³5 67% 0% n=2 -2 -1.5 4/6 ³4 67% 0% -3 VRDN-001 10mg/kg ³3 6/6 1/2 50% 100% -4 n=6 0% -4.3 -5 VRDN-001 Placebo Week 0 Week 6 -100% -50% 0% 50% 100%
10mg/kg 12 Change from baseline score
Symptoms improvement compares favorably with Tepezza Clinical Activity
Score (CAS): a composite 0-7 scale scoring signs and symptoms of TED Mean CAS Change CAS of 0 or 1 at week 6 Mean CAS improvement at week 6 CAS of 0 or 1 at week 6 (to week 6) (Change from baseline score) Tepezza VRDN-001 Tepezza VRDN-001 Tepezza
Tepezza 83% Phase 2 10mg/kg Phase 3 83% 10mg/kg Phase 2 Phase 3 -4.3 -2.5 -2.1 -2.1 -2.5 22% 21% 22% 21% -4.3 Tepezza Tepezza VRD VRDN N -0 - 0001 1 Tepezza Tepezza Phase 2 Phase 3 10mg/kg Phase 2 Phase 3 10mg/kg Tepezza Phase 2 data: Smith TJ, et
al, NEJM 376:18, May 2017 13 Tepezza Phase 3 data: Douglas RS, et al, NEJM 382:4, Jan 2020 FDA clinical review of Tepezza (BLA 761143)
75% of VRDN-001 patients had complete diplopia resolution at week 6
Diplopia resolution rate defined as % of patients with diplopia at baseline that improved to a score of 0 Diplopia resolution vs. Tepezza Complete diplopia resolution at week 6 Complete dip( l% op rie as r pe os no de lu rs t)ion at week 6 *Diplopia
resolution (dg) 75% 75% 75% 75% 36% 36% 30% 29% 0% 0% 3/4 0/1 Tepezza Tepez Tepezzz aa V Tepez RDN-0z 01 a VRDN-001 VRDN-001 Placebo VRDN-001 Placebo Phase 2 Phase 3 10mg/kg Phase 2 Phase 3 10mg/kg 10mg/k 10mg/kg g For patients with diplopia at
baseline, complete diplopia resolution defined as Gorman subjective diplopia score of zero 14 FDA clinical review of Tepezza (BLA 761143)
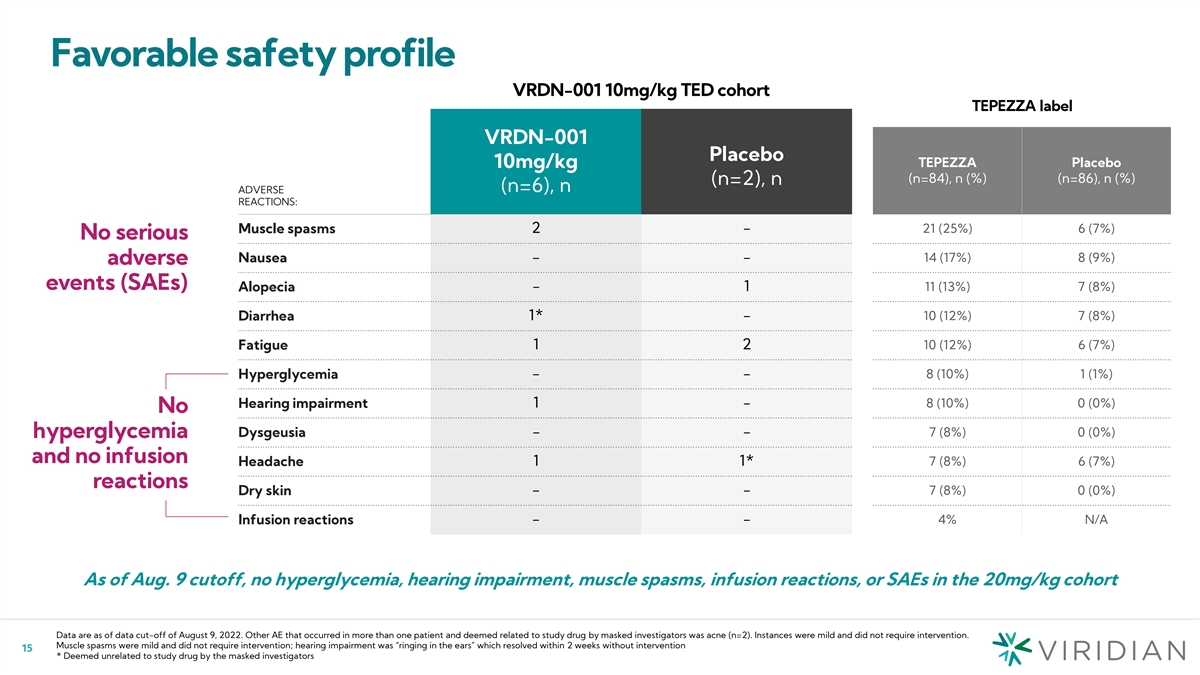
Favorable safety profile VRDN-001 10mg/kg TED cohort TEPEZZA label
VRDN-001 Placebo TEPEZZA Placebo 10mg/kg (n=84), n (%) (n=86), n (%) (n=2), n (n=6), n ADVERSE REACTIONS: 21 (25%) 6 (7%) Muscle spasms 2 - No serious Nausea - - 14 (17%) 8 (9%) adverse events (SAEs) Alopecia - 1 11 (13%) 7 (8%) 1* - 10 (12%) 7 (8%)
Diarrhea Fatigue 1 2 10 (12%) 6 (7%) Hyperglycemia - - 8 (10%) 1 (1%) Hearing impairment 1 - 8 (10%) 0 (0%) No 7 (8%) 0 (0%) Dysgeusia - - hyperglycemia and no infusion Headache 1 1* 7 (8%) 6 (7%) reactions Dry skin - - 7 (8%) 0 (0%) - - 4% N/A
Infusion reactions As of Aug. 9 cutoff, no hyperglycemia, hearing impairment, muscle spasms, infusion reactions, or SAEs in the 20mg/kg cohort Data are as of data cut-off of August 9, 2022. Other AE that occurred in more than one patient and deemed
related to study drug by masked investigators was acne (n=2). Instances were mild and did not require intervention. Muscle spasms were mild and did not require intervention; hearing impairment was “ringing in the ears” which resolved
within 2 weeks without intervention 15 * Deemed unrelated to study drug by the masked investigators
Takeaways for VRDN-001 and VRDN-002 Data Jonathan Violin, Ph.D.,
President and Chief Executive Officer 16
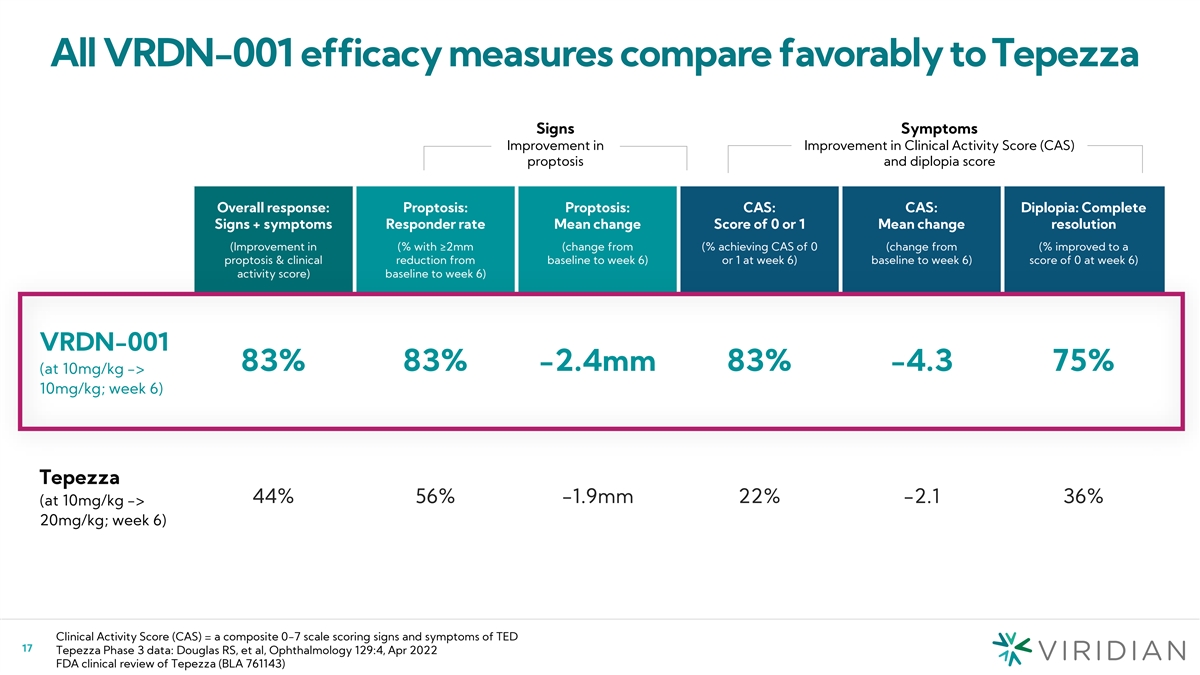
All VRDN-001 efficacy measures compare favorably to Tepezza Signs
Symptoms Improvement in Improvement in Clinical Activity Score (CAS) proptosis and diplopia score Overall response: Proptosis: Proptosis: CAS: CAS: Diplopia: Complete Signs + symptoms Responder rate Mean change Score of 0 or 1 Mean change resolution
(Improvement in (% with ≥2mm (change from (% achieving CAS of 0 (change from (% improved to a proptosis & clinical reduction from baseline to week 6) or 1 at week 6) baseline to week 6) score of 0 at week 6) activity score) baseline to
week 6) VRDN-001 83% 83% -2.4mm 83% -4.3 75% (at 10mg/kg -> 10mg/kg; week 6) Tepezza 44% 56% -1.9mm 22% -2.1 36% (at 10mg/kg -> 20mg/kg; week 6) Clinical Activity Score (CAS) = a composite 0-7 scale scoring signs and symptoms of TED 17 Tepezza
Phase 3 data: Douglas RS, et al, Ophthalmology 129:4, Apr 2022 FDA clinical review of Tepezza (BLA 761143)
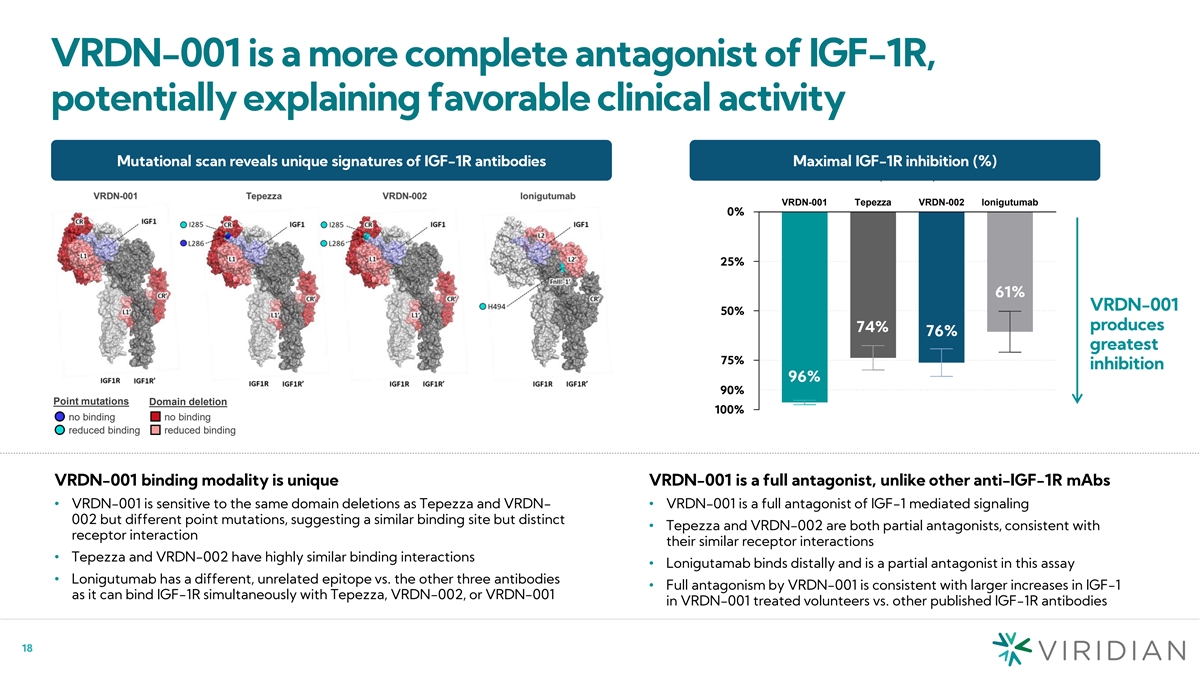
VRDN-001 is a more complete antagonist of IGF-1R, potentially
explaining favorable clinical activity Mutational scan reveals unique signatures of IGF-1R antibodies Maximal IGF-1R inhibition (%) Residual IGF-1R activity (% Inhibition) VRDN-001 Tepezza VRDN-002 lonigutumab 10% 00% 4% 26% 24% 39% 25 7% 5% 61%
VRDN-001 50 5% 0% produces 74% 76% greatest 75 2% 5% inhibition 96% 10% 90% Point mutations Domain deletion 100% 0% no binding no binding reduced binding reduced binding VRDN-001 binding modality is unique VRDN-001 is a full antagonist, unlike other
anti-IGF-1R mAbs • VRDN-001 is sensitive to the same domain deletions as Tepezza and VRDN-• VRDN-001 is a full antagonist of IGF-1 mediated signaling 002 but different point mutations, suggesting a similar binding site but distinct
• Tepezza and VRDN-002 are both partial antagonists, consistent with receptor interaction their similar receptor interactions • Tepezza and VRDN-002 have highly similar binding interactions • Lonigutamab binds distally and is a
partial antagonist in this assay • Lonigutumab has a different, unrelated epitope vs. the other three antibodies • Full antagonism by VRDN-001 is consistent with larger increases in IGF-1 as it can bind IGF-1R simultaneously with
Tepezza, VRDN-002, or VRDN-001 in VRDN-001 treated volunteers vs. other published IGF-1R antibodies 18
Responses occur rapidly and compare favorably to Tepezza Mean time to
response (weeks) Median time to proptosis response Mean time to overall response Mean time to response (weeks) VRDN-001 VRDN-001 VRDN-001 VRDN-001 3.0 4.8 3.0 4.8 10mg/kg 10mg/kg 10mg/kg 10mg/kg weeks weeks Tepez Tepezzz aa Tepezza Tepezza 6.4 11.2
6.4 11.2 Phase 3 Phase 2 Phase 3 Phase 2 weeks weeks Week 0 Week 3 Week 6 Week 9 Week 12 Week 0 Week 3 Week 6 Week 9 Week 12 Reported as median time to response to enable comparison to published Reported as mean time to response to enable comparison
to published Tepezza data. Tepezza reported median time to proptosis response in P3 NEJM Tepezza data. Tepezza reported mean time to overall response in P2 NEJM publication. P2 NEJM publication did not report any time to proptosis response.
publication. P3 NEJM publication did not report any time to overall response. Tepezza Phase 2 data: Smith TJ, et al, NEJM 376:18, May 2017 19 Tepezza Phase 3 data: Douglas RS, et al, NEJM 382:4, Jan 2020
VRDN-001 may offer a shorter treatment course Change in proptosis from
baseline Phase 3 program: standard and shortened treatment course in active and chronic TED 2023 2024 • THRIVE trial: placebo- Topline controlled, active TED Active TED (n=120) • THRIVE-2 trial: placebo- Topline controlled, chronic TED
Chronic TED (n=120) Last 2 doses offer limited additional benefit • Three arms per trial: Week 12 Week 24 − Standard 8 infusions − Accelerated 5 infusions VRDN-001, Q3W 8x − Placebo VRDN-001, Q3W 5x • 24 week primary
Tepezza Phase 3 data suggest limited endpoint Placebo treatment benefit after 18 weeks VRDN-001 Phase 3 will study both a standard 8 infusion course (same as Tepezza) and a shorter 5 infusion course Tepezza Phase 3 data: Douglas RS, et al, NEJM
382:4, Jan 2020 20
VRDN-002 has extended half-life of 30-40 days Non-human primate PK
VRDN-001 HV VRDN-002 HV Time (days) Time (days) Time (days) • VRDN-001 and Tepezza PK very similar in non-human primates: ~6 day half-life 1-6 • VRDN-001 and Tepezza PK very similar in oncology patients: ~10-11 day half-life across 6
clinical trials • VRDN-002 half-life ~3x VRDN-001 in healthy volunteers: interim analysis shows 30-40 day half-life • No SAEs, hearing impairment, hyperglycemia, muscle spasms, or infusion reactions reported as of last subject last visit
for VRDN-002 HV = healthy volunteers 3) Gore L et al, Mol Cancer Ther, 8(12 Suppl), 2009 * Historical data from AVE-1642 IND 4) Faivre SJ et al, J Clin Onc, 29 (4 Suppl), February 2011 21 1) Rodon J et al, J Clin Onc, 2518 Suppl), June 2007 5) Soria
JC et al, Eur J Cancer, 49 (8), 2013 2) Kurzrock R et al, Clin Cancer Res, 16(8), April 2010 6) Moreau P et al, Leukemia 25 (5), February 2011
VRDN-002 mediates IGF-1 increases similar to teprotumumab PK/PD
modeling indicate potential feasibility of 2mL 300mg Q2W to Q4W SC dosing % Change from Baseline of IGF-1 in normal healthy volunteers Teprotumumab VRDN-002 Planned SC POC trial in TED Presumed Placebo Removed Randomized, double-blind trial of 2mL
300mg 1 mg/kg 3 mg/kg Q2W and Q4W SC dosing vs placebo 400 400 3 mg/kg 10 mg/kg 9 mg/kg 20 mg/kg Placebo Cohort 1 SC Q2W 6 patients 200 200 Placebo 2 patients Cohort 2 0 0 SC Q4W 6 patients 0 1 2 3 4 5 6 7 0 20 40 60 80 100 Time (days) Time (days)
Placebo 2 patients ~2.5x increase in plasma IGF-1 ~2.5x increase in plasma IGF-1 published data only through Day 7 elevated through Day 84 after single dose Teprotumumab data from Kurzrock R et al, Clin Canc Res 16(8) April 2010 22 % Change from
Baseline IGF-1 % Change from Baseline IGF-1
VRDN-001 demonstrated rapid, significant Key improvement across all
efficacy measures in takeaways TED at week 6, surpassing prior TED trials from today’s VRDN-001 produces more complete IGF-1R data inhibition via unique receptor interaction VRDN-001 was well tolerated with favorable safety profile VRDN-002
triples half-life with strong PD, potentially enabling Q2W to Q4W low volume SC dosing 23 23
Phase 3 and SC Plans Jonathan Violin, Ph.D., President and Chief
Executive Officer 24
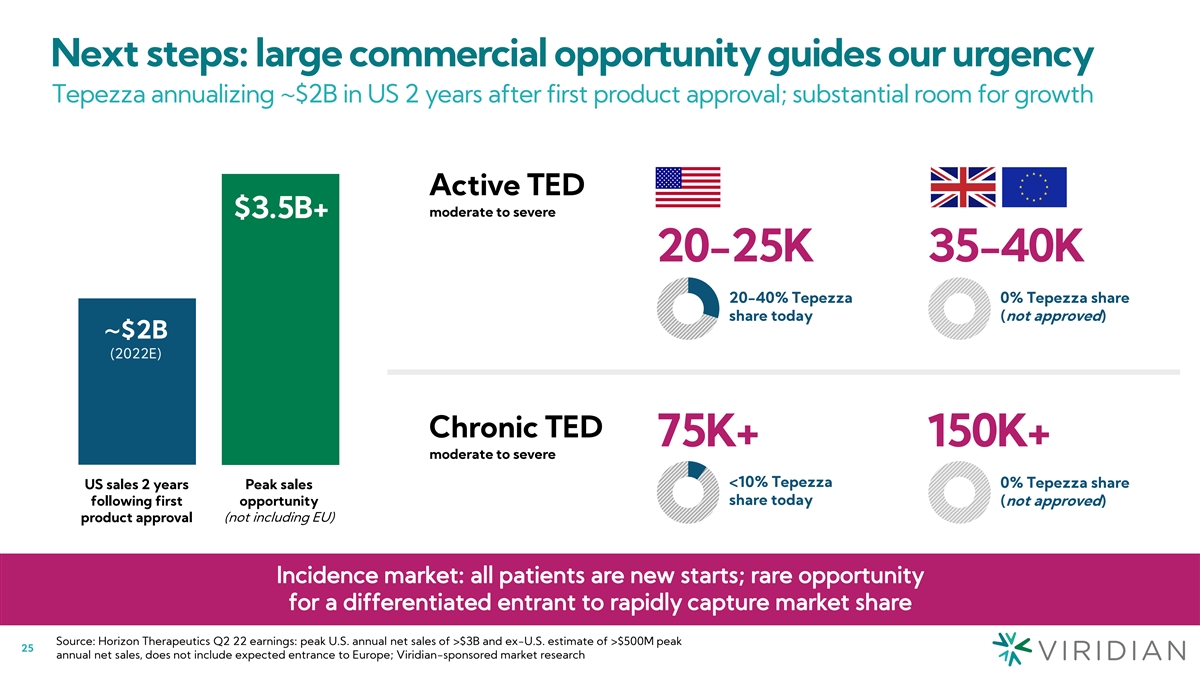
Next steps: large commercial opportunity guides our urgency Tepezza
annualizing ~$2B in US 2 years after first product approval; substantial room for growth Active TED moderate to severe $3.5B+ 20-25K 35-40K 20-40% Tepezza 0% Tepezza share share today (not approved) ~$2B (2022E) Chronic TED 75K+ 150K+ moderate to
severe <10% Tepezza 0% Tepezza share US sales 2 years Peak sales share today following first opportunity (not approved) product approval (not including EU) Source: Horizon Therapeutics Q2 22 earnings: peak U.S. annual net sales of >$3B and
ex-U.S. estimate of >$500M peak 25 annual net sales, does not include expected entrance to Europe; Viridian-sponsored market research
Corporate objectives in TED: Build a market-leading franchise 2 1
Launch Rapidly follow potential best- IV launch with in-class IV TED potential best- therapy in US in-class SC TED and EU therapy 26
Highlights of global IV VRDN-001 Phase 3 program plan • Designed
to assess pivotal efficacy data Global registrational in active AND chronic disease 2023 2024 program for both active • Registrational program designed to enable approval in US, EU, and other and chronic TED Topline Active TED (n=120) major
and emerging markets Topline Chronic TED (n=120) • Accelerated, 12 week, course of therapy − 43% shorter than Tepezza Potential improvements • Shorter infusion times (30 min for on Tepezza VRDN-001 vs. 60-90 min for Tepezza)
• Faster onset and improved efficacy Week 24 Week 12 • Phase 3 program to initiate by YE22 VRDN-001, Q3W 8x • 17 sites active, 30 expected by YE22, Rapid timelines to enter expanding to >50 in 1H23 VRDN-001, Q3W 5x a
multibillion $ market • Phase 3 active TED data by MY24 Placebo • Phase 3 chronic TED data by YE24 27
Viridian is poised to deliver a potential best-in-class SC TED therapy
Both VRDN-002 and VRDN-003 show potential for Q2W and Q4W dosing to be tested convenient, low-volume, SC product profile • VRDN-002 epitope and in vitro profile very similar • 2mL 300mg SC Q2W compares favorably with to teprotumumab,
achieves half-life ~3x first other successful SC products generation anti-IGF-1R mAbs – VRDN-001 PK/PD and efficacy data at 10mg/kg inform VRDN-002 and VRDN-003 dose selection – Interim analysis shows 30-40 day half-life – PK/PD
modeling supports at least 2mL 300mg SC Q2W • Unveiling VRDN-003: extended half-life VRDN-001 profile for both VRDN-002 and VRDN-003 – Retains unique VRDN-001 binding & antagonist – VRDN-001 efficacy data at 3mg/kg to further
inform properties Q4W or longer profiles for VRDN-002 and VRDN-003 – Same half-life extension technology as VRDN-002 • Launch with patient-friendly pre-filled pen device – Non-human primate data show PK expected to match VRDN-002
– Well into IND enabling activities; IND expected 2Q23; healthy volunteer PK/PD data 4Q23 Plan to choose either VRDN-002 or VRDN-003 by YE23, and initiate Phase 3 trials in early 2024 28
Q2W to Q4W TED SC program plan Clinical data allows us to select best
program to start a planned Phase 3 trial in early 2024 Decision: Select one SC program to advance 2023 2024 VRDN-002 SC SC POC Q2W to Q4W Topline trial initiation SC patient data 2H23 SC Phase 3 Planned initiation Planning for active early 2024
VRDN-001 sites to roll over to SC Phase 3 program POC PK/PD HV VRDN-003 SC Submit IND single dose data extended half-life 001 Q2W to Q4W SC HV data HV multiple dose 4Q23 29
Timeline and planned milestones 4Q22 YE22 MY24 3mg/kg active TED data
20mg/kg Initiation data active TED data 1H23 YE24 upcoming medical congress Initiation data Chronic TED Chronic TED POC initiation POC data Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 2022 2023 2024 SC 003 IND SC phase 3 start SC 002 TED POC data 2Q23 Early 24
2H23 SC 003 HV POC data 4Q23 30

Second Quarter Financials Kristian Humer, Chief Financial and Business
Officer 31
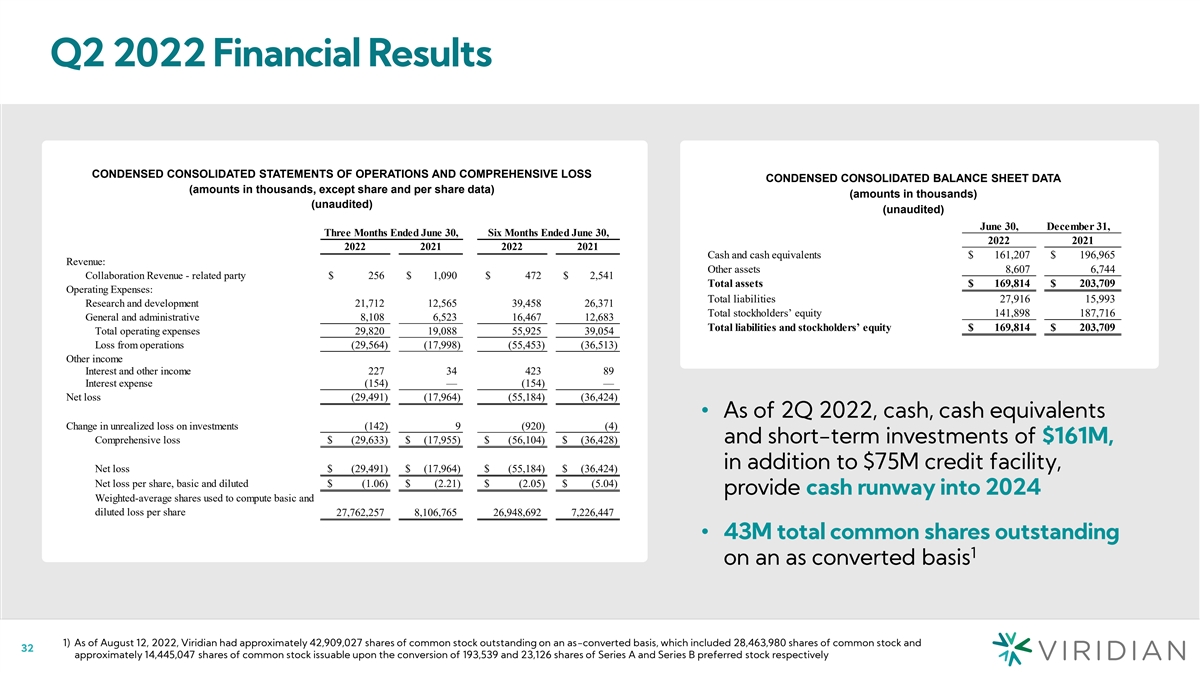
Q2 2022 Financial Results CONDENSED CONSOLIDATED STATEMENTS OF
OPERATIONS AND COMPREHENSIVE LOSS CONDENSED CONSOLIDATED BALANCE SHEET DATA (amounts in thousands, except share and per share data) (amounts in thousands) (unaudited) (unaudited) June 30, December 31, Three Months Ended June 30, Six Months Ended
June 30, 2022 2021 2022 2021 2022 2021 Cash and cash equivalents $ 161,207 $ 196,965 Revenue: Other assets 8,607 6,744 Collaboration Revenue - related party $ 256 $ 1,090 $ 472 $ 2,541 Total assets $ 169,814 $ 203,709 Operating Expenses: Total
liabilities 27,916 15,993 Research and development 21,712 12,565 39,458 26,371 Total stockholders’ equity 141,898 187,716 General and administrative 8,108 6,523 16,467 12,683 Total liabilities and stockholders’ equity $ 169,814 $ 203,709
Total operating expenses 29,820 19,088 55,925 39,054 Loss from operations (29,564) (17,998) ( 55,453) (36,513) Other income Interest and other income 227 34 423 89 Interest expense ( 154) — (154) — Net loss (29,491) (17,964) ( 55,184)
(36,424) • As of 2Q 2022, cash, cash equivalents Change in unrealized loss on investments (142) 9 (920) ( 4) Comprehensive loss $ (29,633) $ ( 17,955) $ ( 56,104) $ ( 36,428) and short-term investments of $161M, in addition to $75M credit
facility, Net loss $ (29,491) $ (17,964) $ ( 55,184) $ (36,424) Net loss per share, basic and diluted $ ( 1.06) $ (2.21) $ ( 2.05) $ (5.04) provide cash runway into 2024 Weighted-average shares used to compute basic and diluted loss per share
27,762,257 8,106,765 26,948,692 7,226,447 • 43M total common shares outstanding 1 on an as converted basis 1) As of August 12, 2022, Viridian had approximately 42,909,027 shares of common stock outstanding on an as-converted basis, which
included 28,463,980 shares of common stock and 32 approximately 14,445,047 shares of common stock issuable upon the conversion of 193,539 and 23,126 shares of Series A and Series B preferred stock respectively

Q&A 33

Thank you! 34


