Call highlights
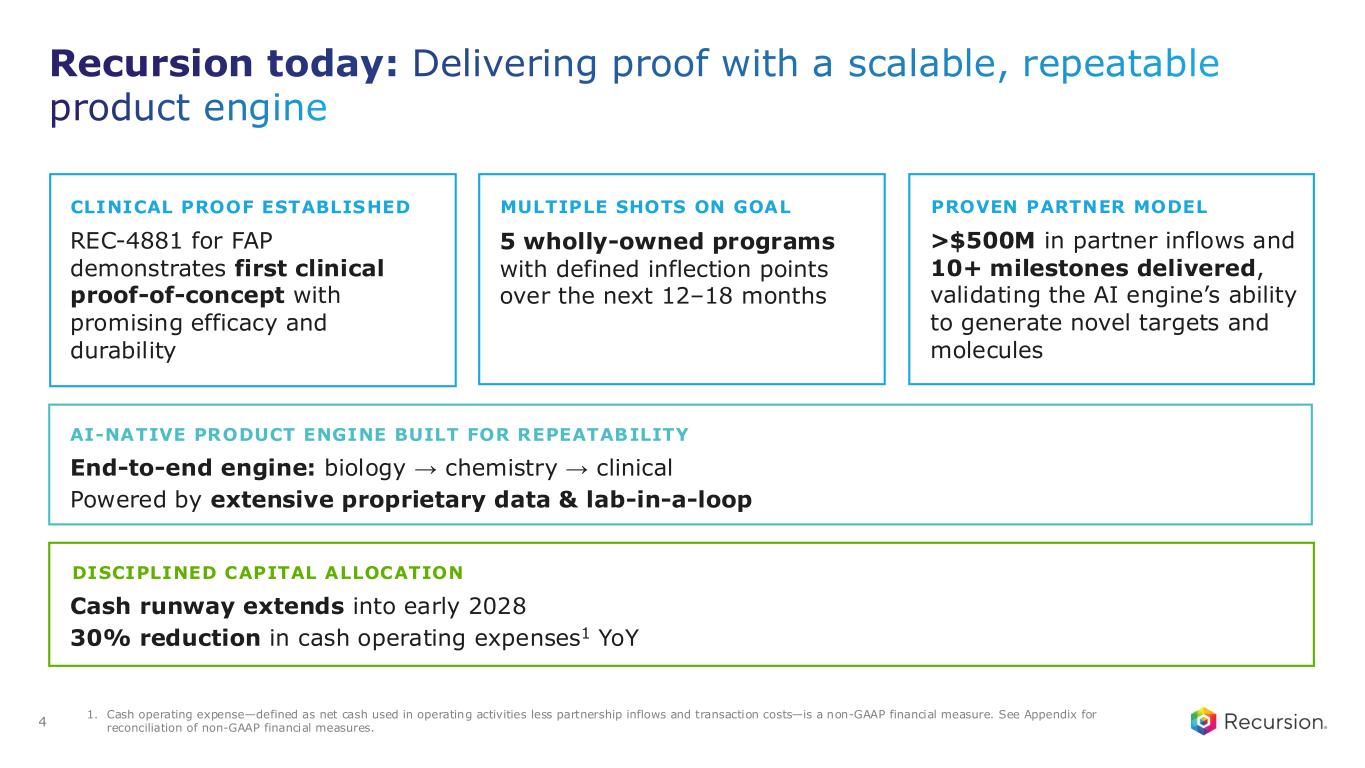
Recursion reported Q1 2026 progress across its wholly owned and partnered pipelines, including early clinical data for REC-1245, continued momentum on REC-4881 in FAP, and first-patient-dosed for REC-4539, while reiterating <$390M 2026 cash burn guidance and runway into early 2028 with operating expenses reduced 30% year-over-year.
“Financially, we have extended our runway into early 2028 while reducing operating expenses by 30% year-over-year. This is how we are moving from promise to proof.”
“We now have five wholly owned programs, each with clear inflection points over the next 12 to 18 months, creating a consistent cadence of catalysts and opportunities to test, learn, and be disciplined about where we invest.”
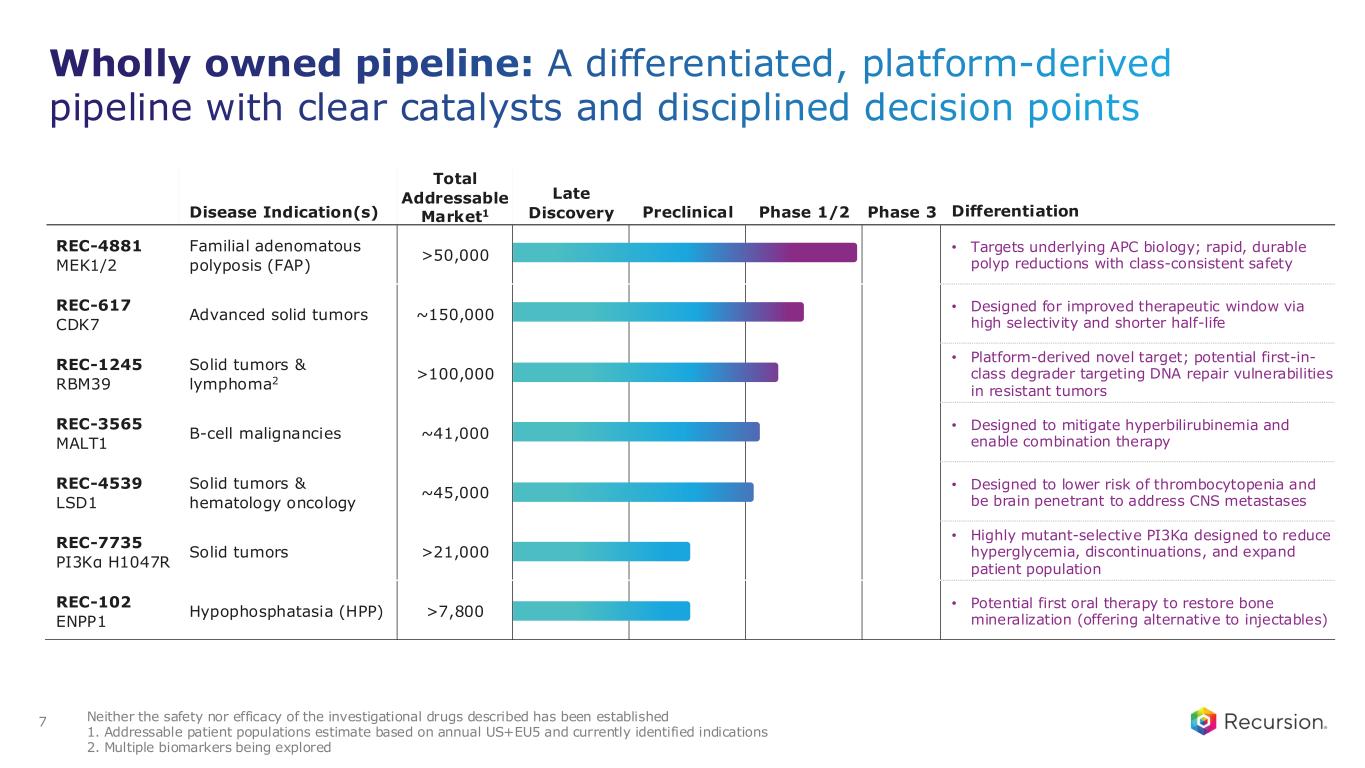
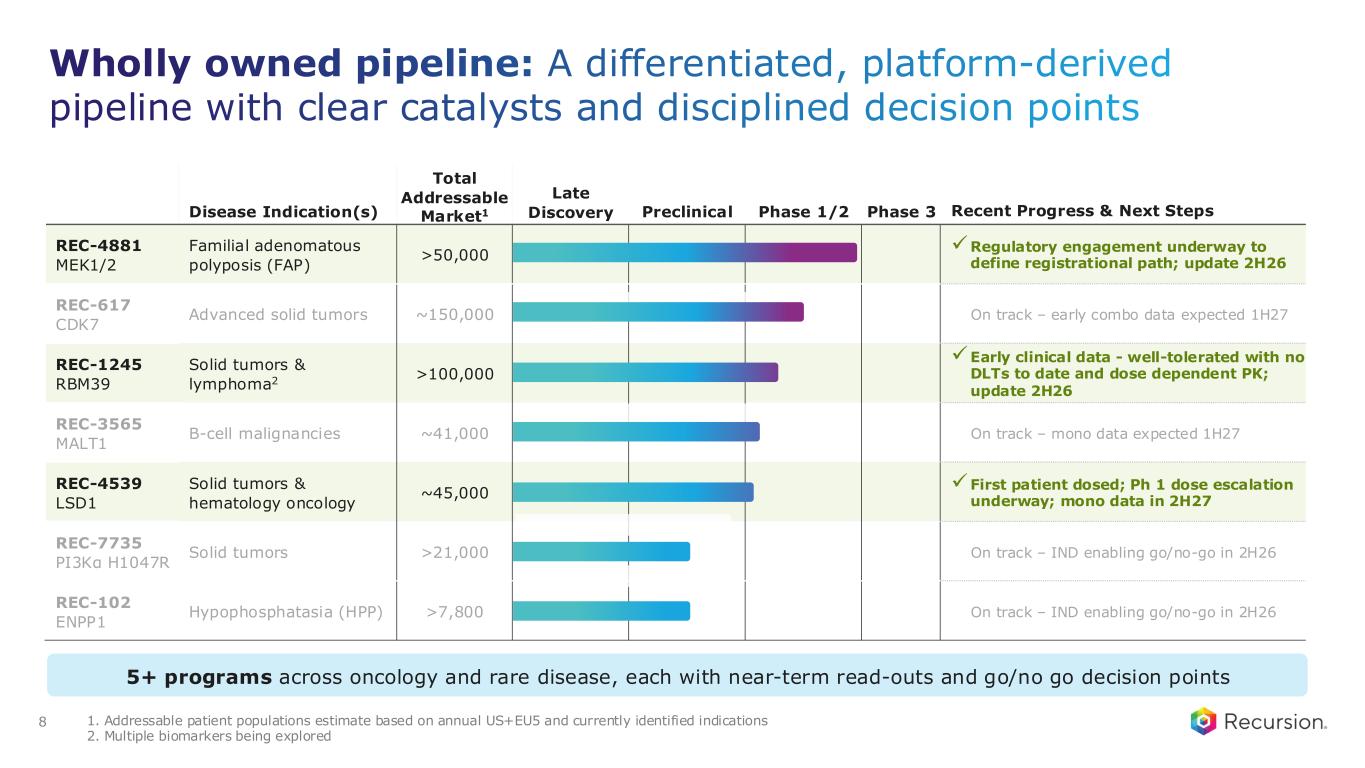
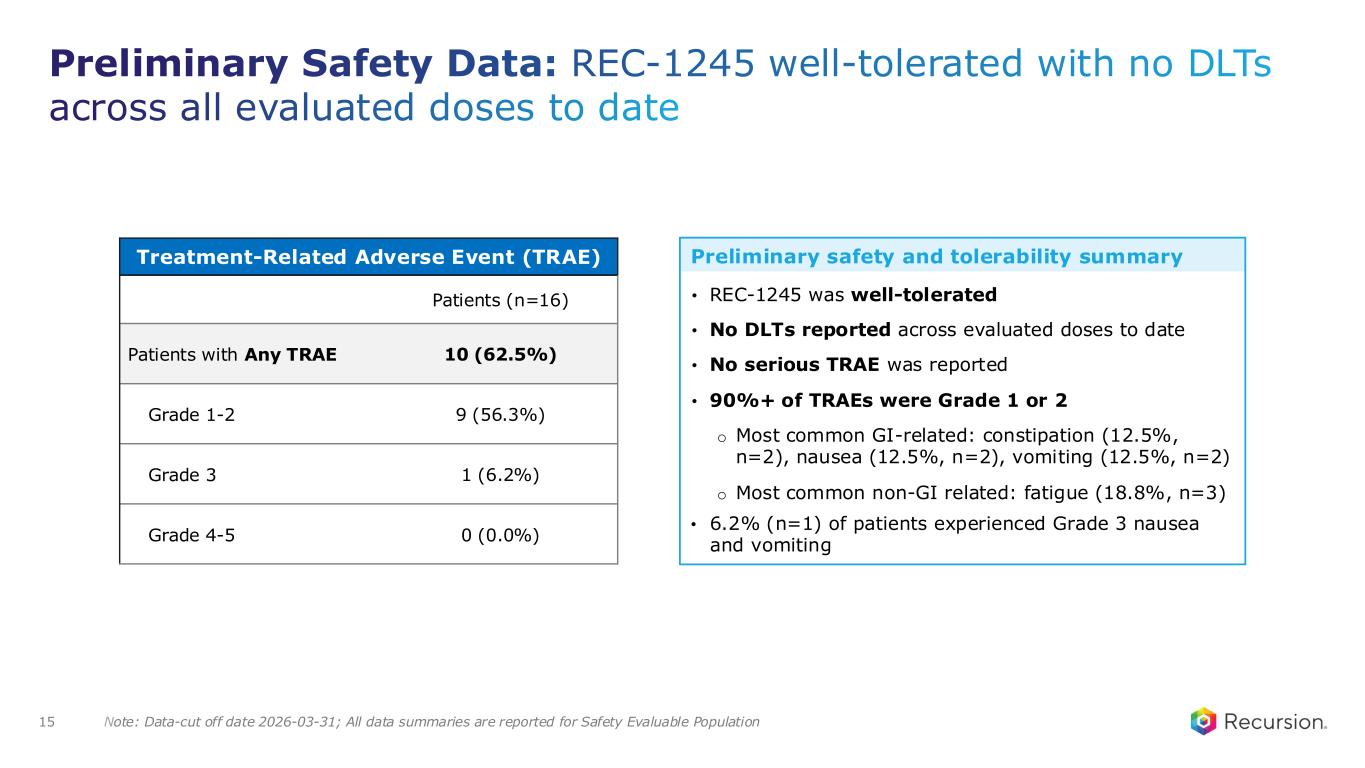
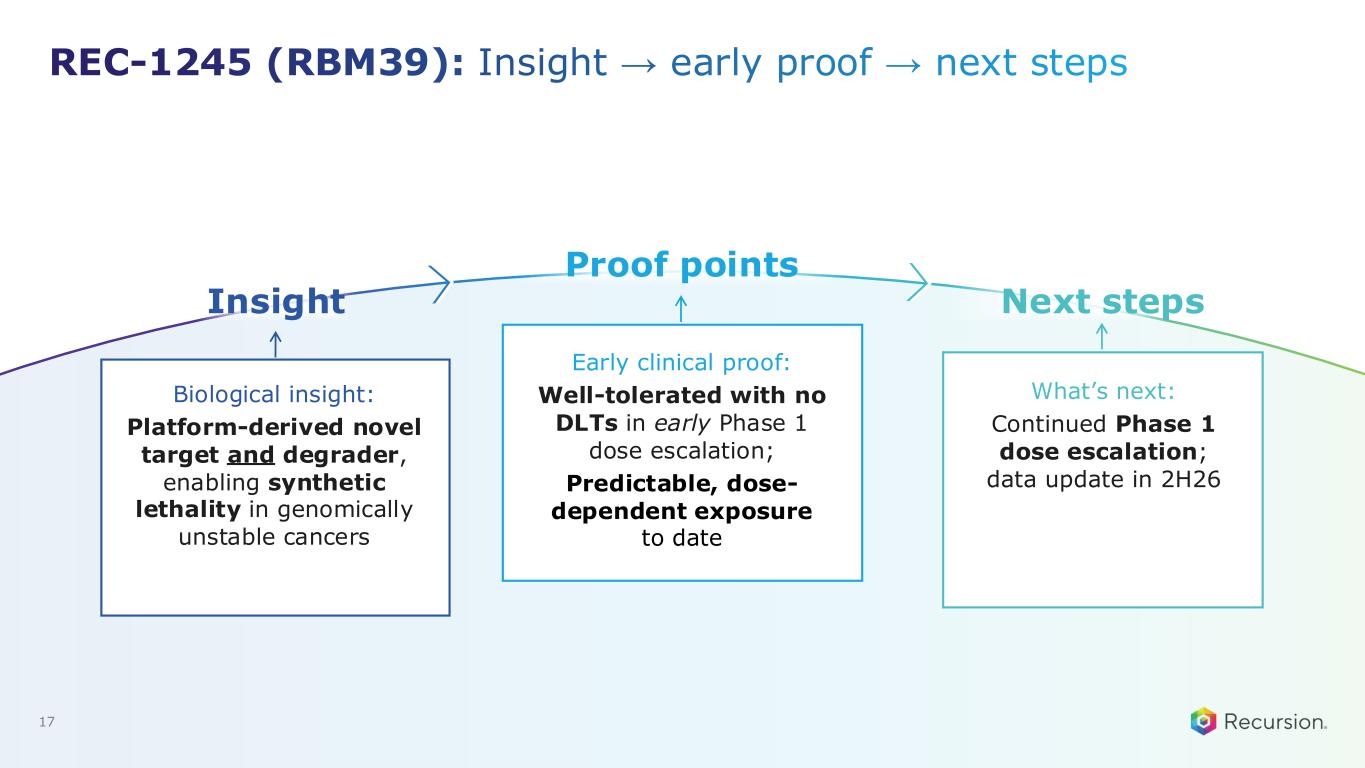
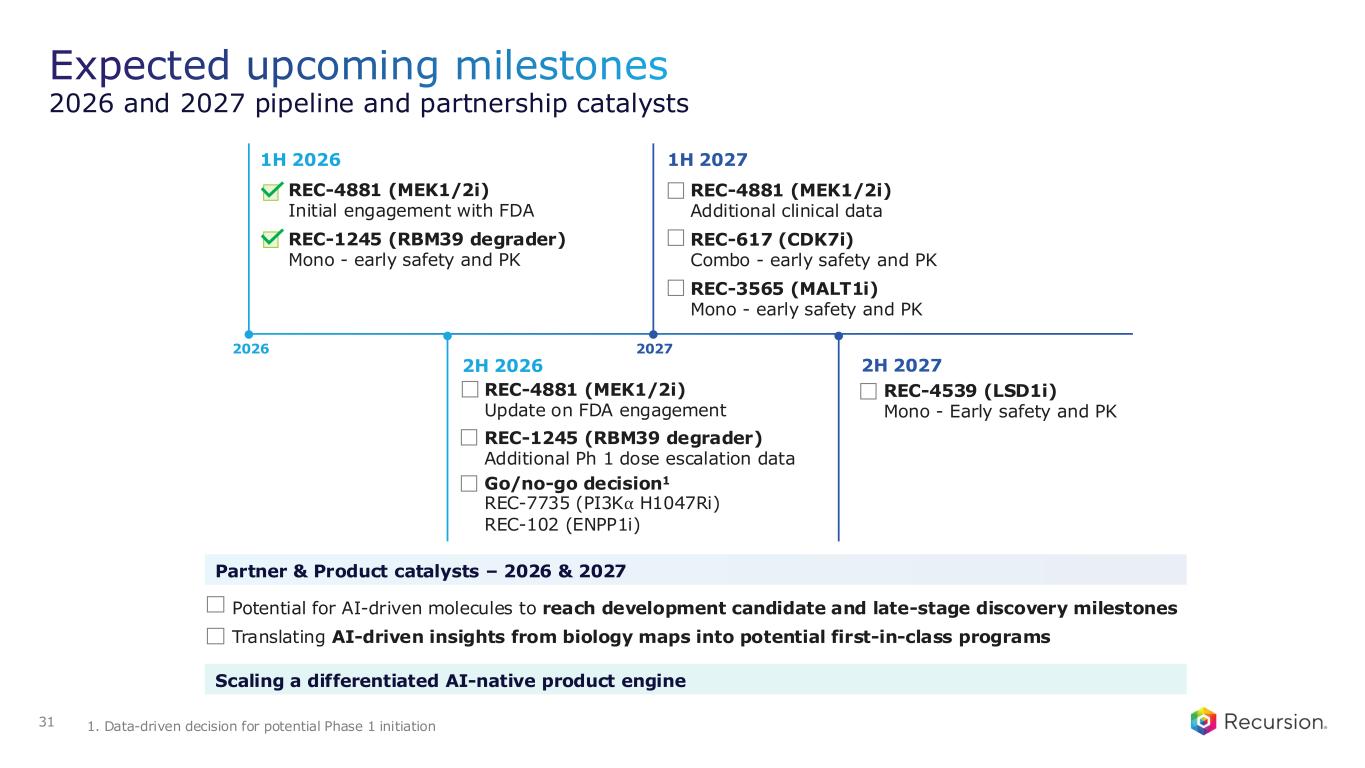
- REC-1245 (RBM39 degrader): early clinical data in solid tumors showed well-tolerated safety, predictable dose-dependent PK, and no dose-limiting toxicities observed to date, supporting ongoing dose escalation.
- REC-4881 (allosteric MEK1/2 inhibitor in FAP): Phase 2 proof of concept showed significant reduction in precancerous polyps with durability, and FDA engagement has been initiated to define a potential registrational path; updates expected in 2H26.
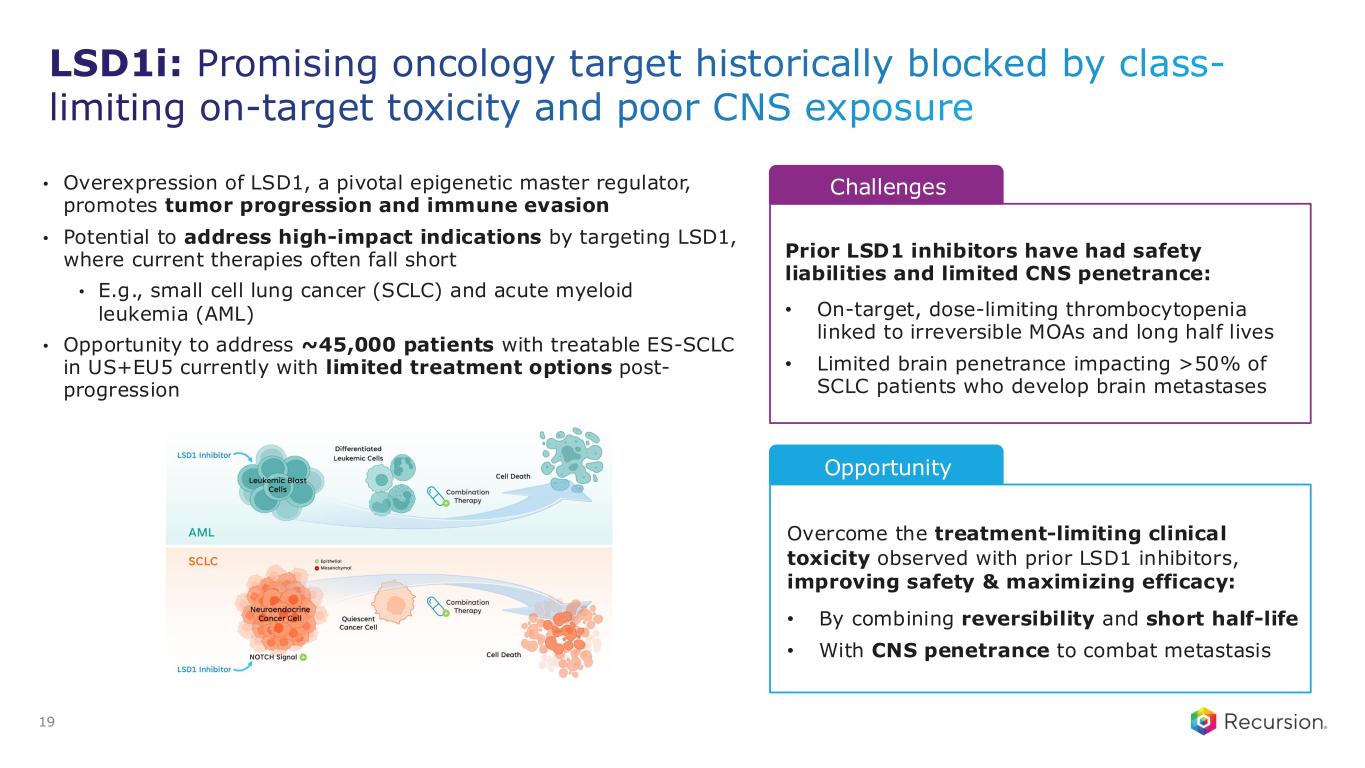
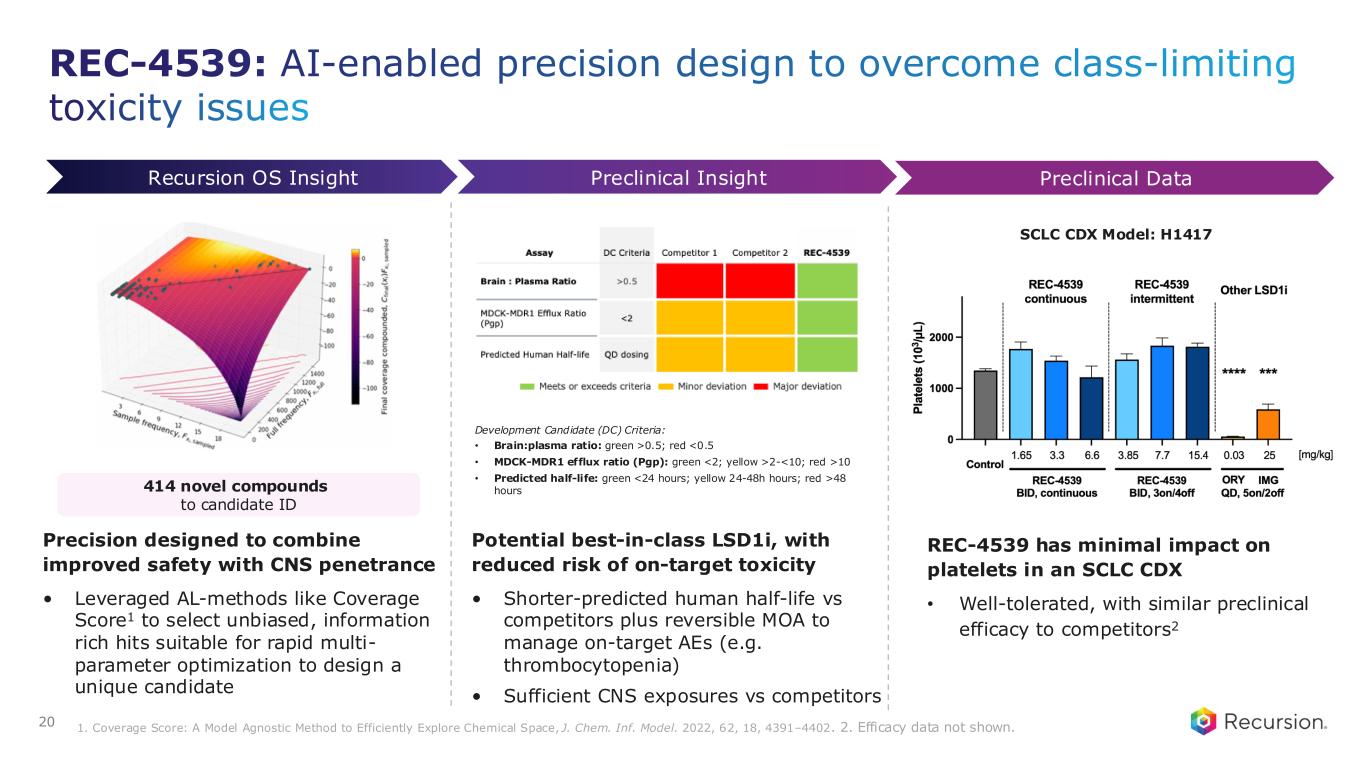
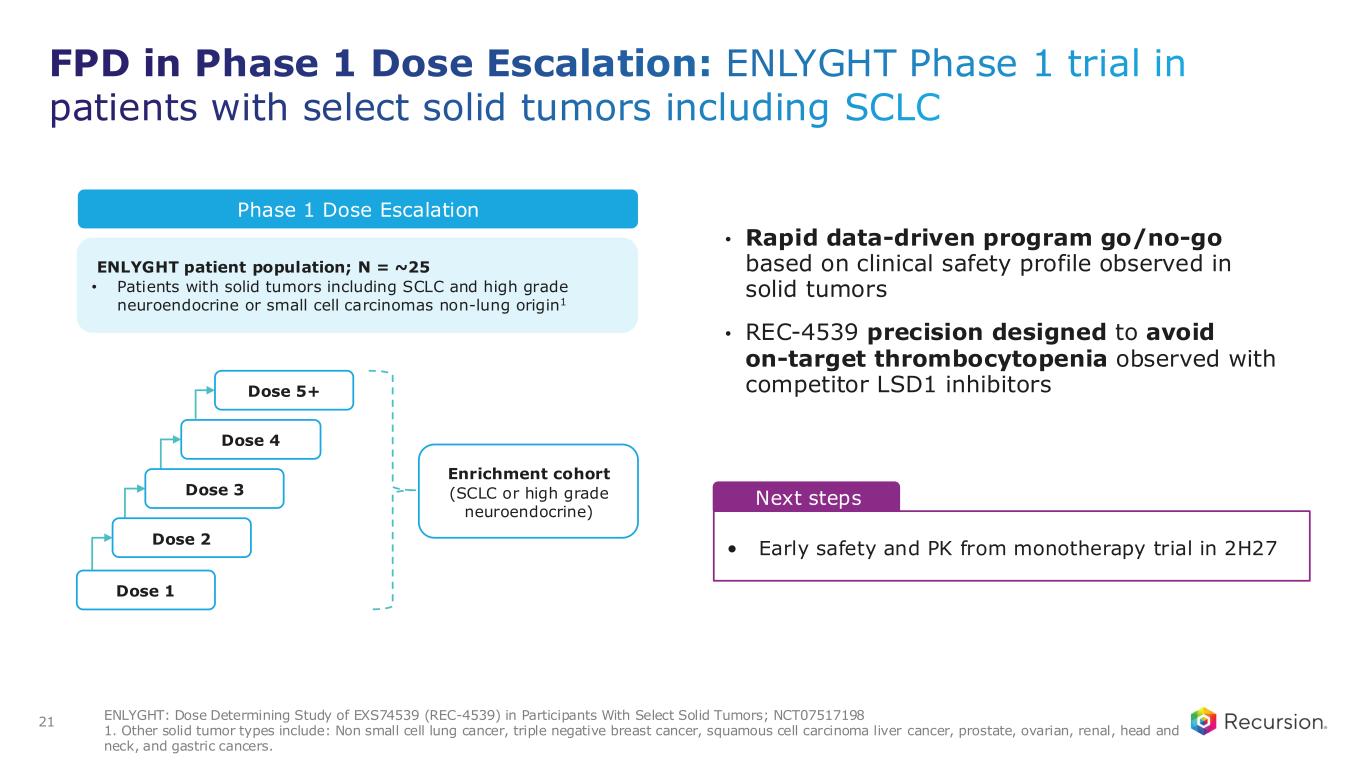
- REC-4539 (LSD1 inhibitor): first patient dosed in Phase 1 with a platform-derived, brain-penetrant profile designed to reduce on-target platelet toxicity.
- Five wholly owned programs with clear inflection points over the next 12–18 months, creating a consistent catalyst cadence.
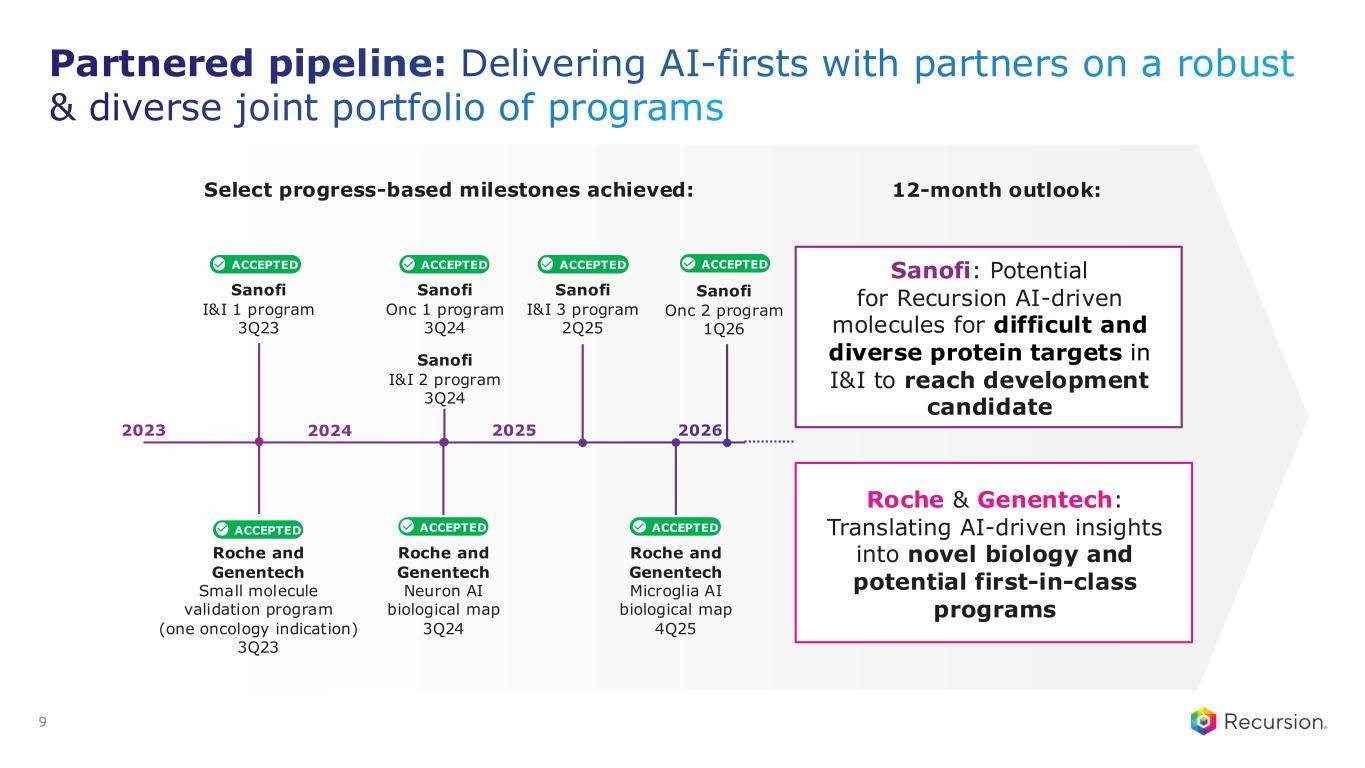
- Partnered portfolio: over $500 million in inflows and 10 milestones delivered to date, including advancing five programs that have hit early discovery milestones toward potential opt-in with Sanofi and Roche/Genenteche.
- Financial discipline: operating expenses reduced 30% year-over-year, cash runway extended into early 2028, and 2026 operational cash burn guidance reiterated at <$390 million without additional financing.
- REC-4539 additional updates are not expected until the second half of 2027, indicating a long wait for further clinical validation.
- Platform monetization relies on uncertain future milestones and potential partner opt-ins, with the balance between near-term milestones and retained long-term economics explicitly described as an open trade-off.
- Most partnered programs (e.g., Sanofi, Roche/Genenteche) remain in early design/discovery stages, meaning meaningful opt-in economics are not yet realized.
- No revenue-generating medicines yet; strategy remains focused on translating proof to products rather than commercial sales.
Guidance
from the 8-K filed May 6, 2026| Metric | Period | Guided | Basis |
|---|---|---|---|
| Operational cash burn Initiated | 2026 | $0 – $390M | — |
Transcript
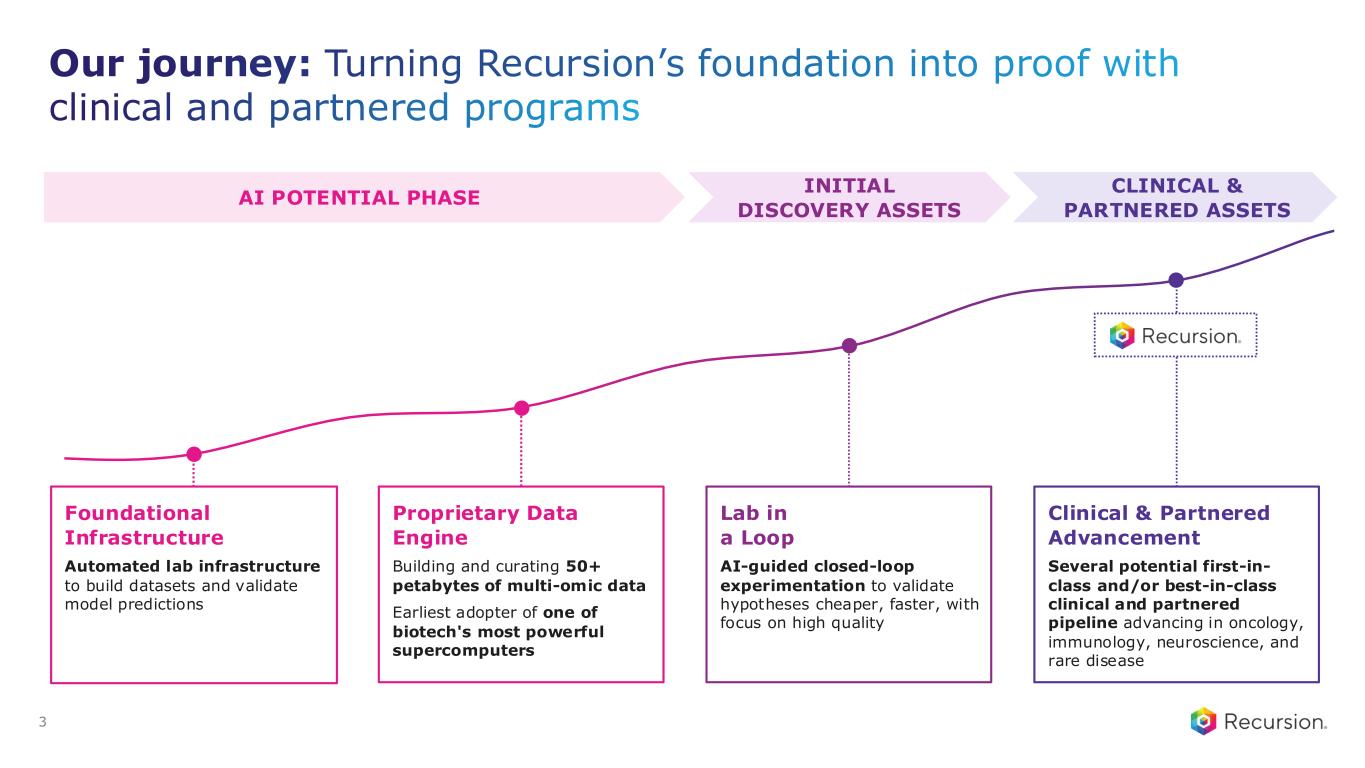
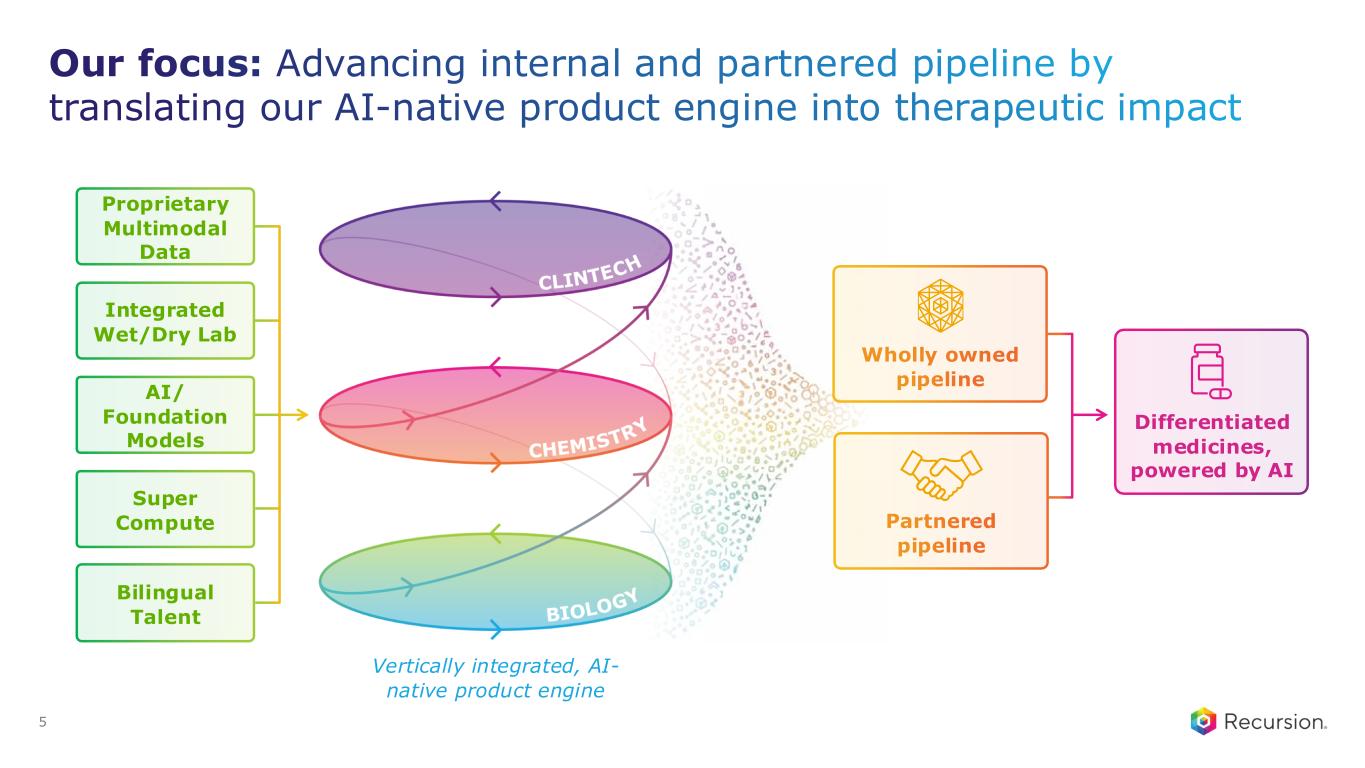
Good morning, everyone, and thank you for joining us. Since stepping into this role, I've been focused on one question: how do we harness the full power of AI to urgently and consistently create better medicines for patients? That requires bold ambition, focus, and discipline to create value for patients and shareholders, so our approach has been deliberate. First, we're prioritizing signal over noise, generating proof and proof points across our wholly owned and partner programs to show where AI can truly create value. Second, we are evolving our platform into a repeatable, AI-driven product engine—technology not for its own sake, but to build valuable products. Third, underpinning everything is financial discipline and thoughtful capital allocation, ensuring we use data to prioritize and invest in our highest-conviction opportunities to deliver durable value. Today I'm excited to share updates. We are making meaningful progress across these fronts, which Vicki, Ben, and I will outline. Before we dive in, note that we'll be making forward-looking statements on this call; please refer to our SEC filings for more information. To put our progress in context, it helps to step back to how we built the foundation that enables it. Recursion has been on an intentional, pioneering journey. Early on we recognized both the immense potential of AI in drug discovery and the reality that the foundational elements—data, compute, biology, and the broader scientific infrastructure—are still being built. That changed how we apply AI. We deliberately invested ahead of the curve to generate and curate proprietary data, build scaled compute infrastructure, integrate automation, and, importantly, develop purposeful models in a true lab-in-a-loop system designed to predict, test, validate, and continuously learn. That has produced a differentiated foundation that we continue to expand and refine. Equally important now is translating that foundation into tangible proof: advancing programs, producing high-quality candidates, and demonstrating repeatability as we evolve into a product-focused AI engine. So where are we today? First, we have established our first clinical proof of concept with REC-4881, an allosteric MEK1/2 inhibitor focused on FAP. We showed a significant reduction in the precancerous polyps that drive disease progression and demonstrated durability, which is unique in the data we've shared. These are patients with no therapeutic solutions today who often require life-altering surgeries and face near-inevitable colorectal cancer risk. This is a clear example of translating AI-directed insights into real outcomes. We will share more on the latest soon. This is not a single-asset story. We now have five wholly owned programs, each with clear inflection points over the next 12 to 18 months, creating a consistent cadence of catalysts and opportunities to test, learn, and be disciplined about where we invest. We will share more data from REC-1245, our RBM39 degrader. Momentum also extends across our partnered portfolio: we have received over $500 million in inflows and, importantly, have delivered 10 milestones to date. Announcing partnerships is one thing; delivering value from them is another, and many of these are first-in-industry achievements. We are grateful to our partners for close collaboration. At the core of everything is our platform: an end-to-end, AI-native product engine spanning biology, chemistry, and clinical development, powered by proprietary data and a lab-in-a-loop system and designed for repeatability. I will share some platform metrics later. Financially, we have extended our runway into early 2028 while reducing operating expenses by 30% year-over-year. This is how we are moving from promise to proof. How does it all come together? At the foundation is an AI-native product engine that combines proprietary multimodal data, integrated wet and dry labs, purpose-built models, and scale compute. What differentiates us is integration: not a single model, datum, or program, but the combination of tools, technologies, and teams. Our proprietary multimodal data, generated internally and integrated with public data, gives us the best of both worlds. Our automated wet labs in Salt Lake City and Milton Park, Oxford are interconnected with purpose-built AI models, and we have in-house supercompute to rapidly build and learn from those algorithms. Spanning everything is our greatest resource: bilingual talent—AI researchers who respect the humility of making medicines and drug developers who bring hands-on experience and openness to AI. Culture, talent, and integration are among the hardest things to achieve in this space, and we've made substantial progress. These ingredients create a vertically integrated platform starting with biology so we can simulate and understand biology more effectively. We want to move away from the statistic that the industry only understands about 10% of biology; this enables identification of novel targets and deeper insight into root causes of disease. Next, through integration with Exscientia and generative chemistry, active learning, and other approaches, we design precisely created, differentiated molecules that can be first-in-class for novel targets or best-in-class for known targets by optimizing therapeutic index. Third, over the last year we've applied our data and insights to design a smarter, more effective, patient-centric clinical development path—choosing the right patients, protocols, and execution strategies. Taken together, this lets us build a broad, diversified portfolio internally and with partners to develop differentiated medicines for patients with significant unmet needs, faster and better. Our strategy remains clear: be focused, disciplined, and ambitious. First, translate proof to products by advancing pipeline learnings toward revenue-generating medicines, using rigorous, data-driven prioritization to invest only in the highest-confidence opportunities. Second, scale a differentiated AI-native product engine where each prediction and experiment compounds learning and drives repeatability in creating better products. Third, pair ambition with disciplined execution through rigorous capital allocation, operational focus, and measurable milestones to sustain long-term value creation. Now, on our wholly owned pipeline: we are starting to translate strategy into early signals of progress. Our portfolio is broad and increasingly diverse, built on two key principles: clear platform-derived rationale for differentiation and a rapid, defined path to upcoming milestones and decision points. Differentiation comes from novel biological targets, differentiated molecular design, and, more recently, our clinical development AI platform that informs patient selection and protocol design. Highlights from the last quarter show strong and accelerating clinical momentum. REC-4881, our allosteric MEK1/2 inhibitor rooted in a novel mechanistic insight, has potential to be the first precision therapy for FAP. We have compelling proof of concept and are advancing the program with urgency, including initiating FDA engagement to define a potential registrational path. We expect updates in the second half of this year. REC-1245 is our platform-derived, first-in-class target and degrader with potential in multiple solid tumors and lymphoma. Today we shared early clinical data on safety, tolerability, and PK. To date, it has been well tolerated with no dose-limiting toxicities, and we expect additional data later this year. Dr. Vicki Goodman, our Chief Medical Officer, will go into more detail shortly. REC-4539 is our LSD1 inhibitor for potential treatment of solid tumors, including small cell lung cancer, and AML. This molecule was designed with our generative platform to overcome treatment-limiting on-target toxicity seen in earlier LSD1 inhibitors. We have initiated a Phase I clinical trial and dosed the first patient, with additional updates expected in the second half of 2027. I'll discuss the program biology, unmet need, and platform insights shortly. All other programs remain on track. We are also seeing consistent execution across our partner pipeline, where our platform is applied with partners whose expertise and capabilities we value deeply. Two potential unlocks are emerging: with Sanofi, the unlock is AI-driven chemistry design to drug historically challenging, diverse protein targets in immunology and oncology, progressing toward key inflection points over the next 12 months, including potential development candidates. With Roche and Genentech, the unlock is on the biology side—leveraging biology perturbation at scale to translate large multimodal maps into actionable, validated targets and potential first-in-class programs. We aim to have a first on track within the next 12 months or so. Talent is the secret sauce. Building a strong, experienced, ambitious, and humble team is essential to driving value. With that, I’m pleased to introduce our newest executive team member, Dr. Vicki Goodman, our new Chief Medical Officer. Vicki brings a strong track record of delivering transformational medicines across the FDA, large pharma, and biotech. She is the right person to lead Recursion’s clinical development in this next chapter, with the skill set and perseverance required for drug discovery and development. Vicki, why don’t you say a few words about joining Recursion and then share more details about REC-1245?
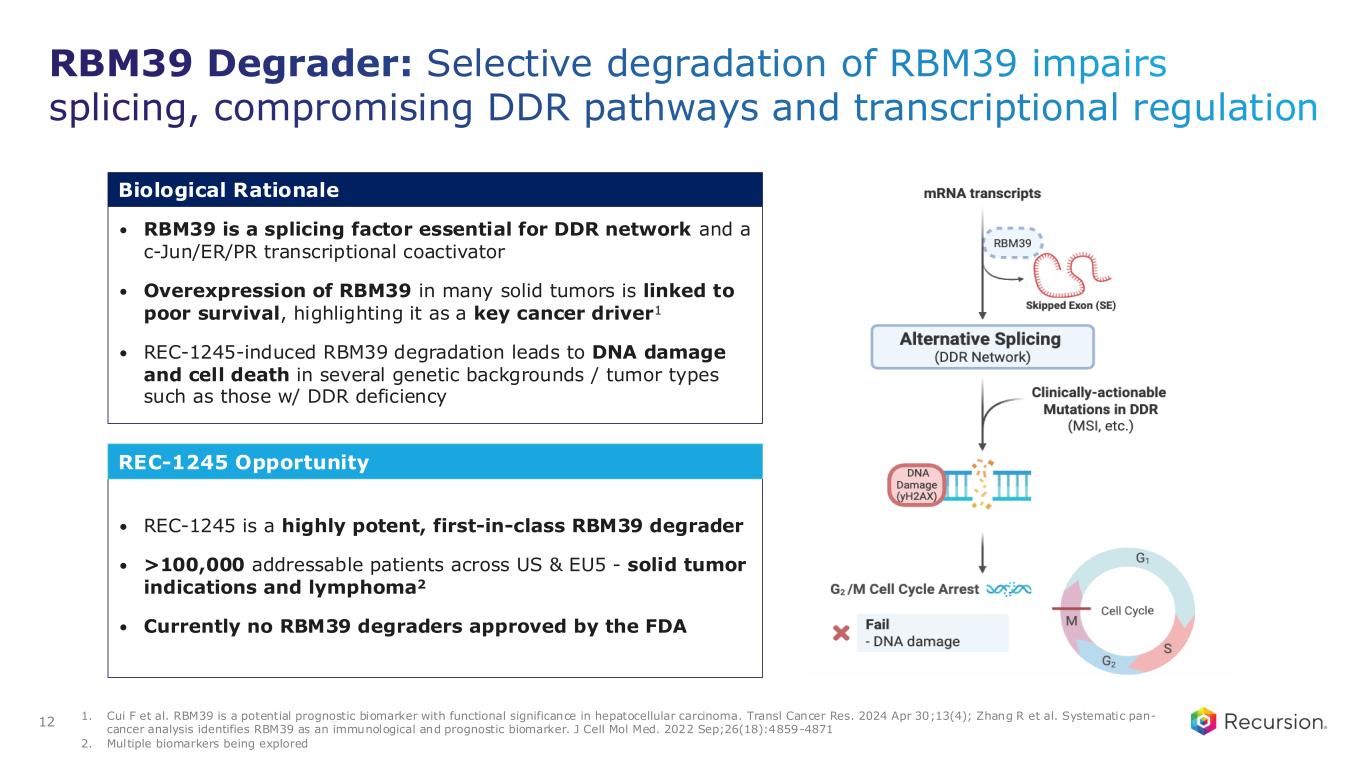
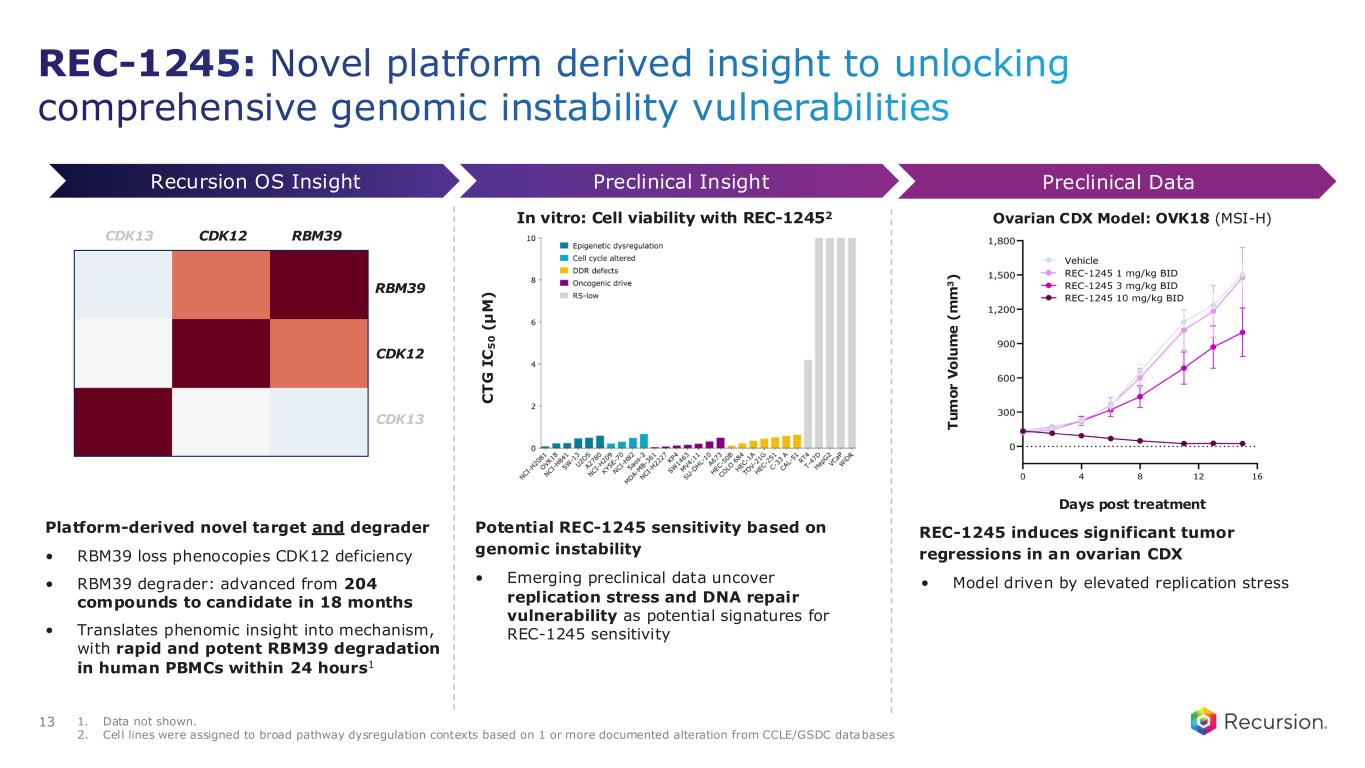
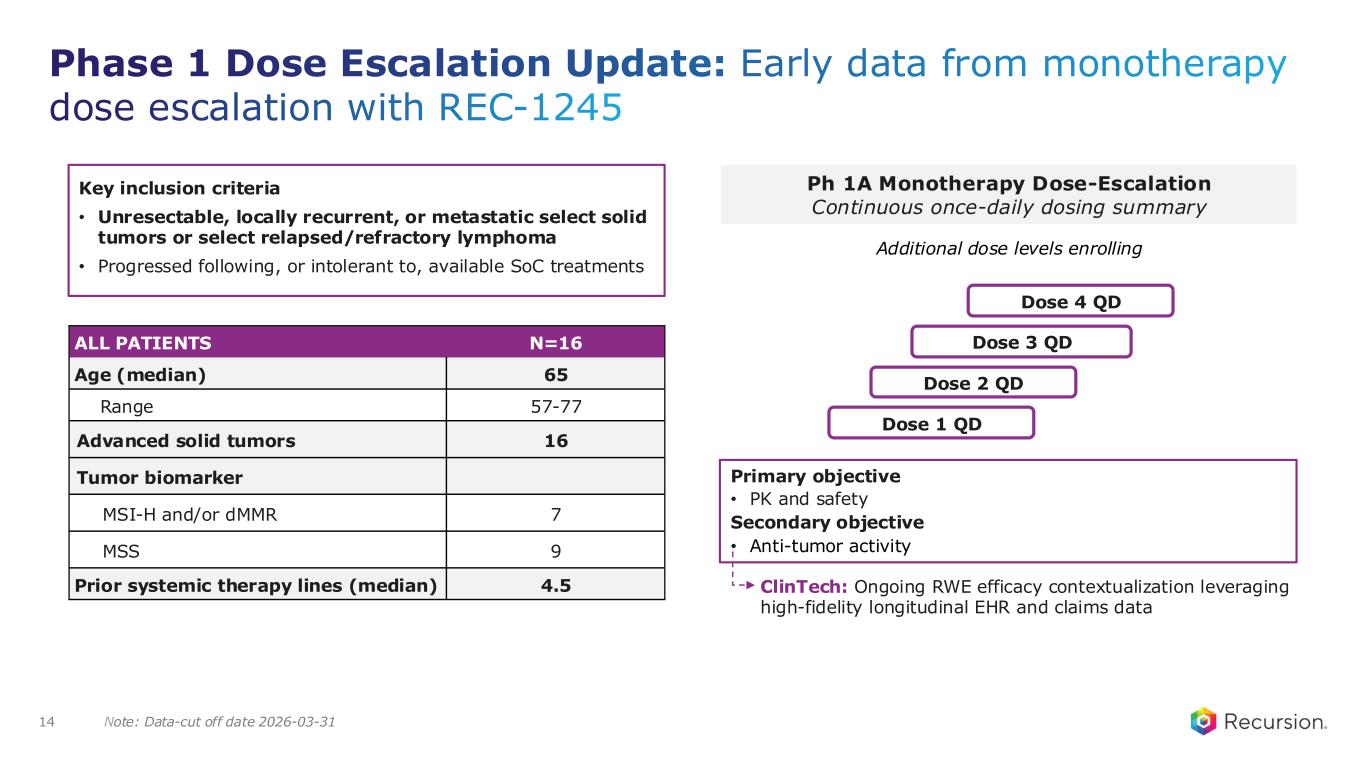
Thank you, Najat, for the kind introduction and for the opportunity to work with you and the rest of the Recursion team. One of the reasons I joined Recursion is because the breadth and differentiation of our pipeline represents one of the most exciting opportunities to translate AI advances into meaningful therapies for patients. Today marks exactly 1 month since I joined. And even in that short time, I've found Recursion to be a place where scientific rigor, intellectual curiosity, and a deep spirit of innovation are brought to bear on the creation of new medicines that matter. It's wonderful to be part of the team, and I look forward to continuing this important work. Today, I have the privilege of presenting an exciting clinical update for REC-1245 from the ongoing DAHLIA Phase I study, including preliminary safety and pharmacokinetics. REC-1245 is an RBM39 degrader currently in Phase I for the treatment of patients with solid tumors and lymphomas. RBM39 is a novel target, which plays a central role in splicing fidelity. When RBM39 is degraded, it induces widespread splicing defects to which tumors that are already under stress, such as those with DNA damage repair deficiencies, global genomic instability, or replication stress, may be particularly sensitive. Additionally, RBM39 is highly expressed in certain tumors and is associated with disease progression and poor survival. The relevant patient population is estimated to be over 100,000 patients in the U.S. and EU5. So that's why RBM39 is an interesting target. The how we came to be working on RBM39 is a story we've touched on before. It's an example of how the biology element of our AI-driven platform enables the identification of novel therapeutic targets. Using genome-scale phenomic mapping, our maps of biology, RBM39 emerged as a functional analog of CDK12. This novel relationship, which came from an unbiased platform insight, was not obvious from sequence homology or traditional pathway analysis. CDK12 is a well-known oncology target for its role in DNA damage response modulation, but it has generally suffered from challenges in selectivity because of how homologous to CDK13 it is. Following our insight, we developed molecular glues and degraders for RBM39, and we showed that these phenotypically mimic CDK12 loss but not CDK13. This provides a druggable potential analog for CDK12 without the CDK13-driven toxicity. We progressed from target ID to IND-enabling studies with roughly 200 compounds synthesized in 18 months, which is significantly faster than traditional approaches. We then needed to correlate our insights with the mechanism of action for RBM39 to translate them into clinically actionable hypotheses. We confirmed through in vitro studies that there is a greater sensitivity to REC-1245 in cell lines that have higher replication stress and DNA repair vulnerability versus cell lines that don't have higher replication stress. And in the panel on the right, you can also see that in vivo tumor regression in an MSI-high ovarian CDX model was also demonstrated. We've carried these insights forward into the design of our DAHLIA Phase I/II clinical trial. Our early clinical strategy focuses on tumor types with those same characteristics that suggested sensitivity in our preclinical experiments. The safety and PK data we are sharing today is from 16 patients enrolled across the first 4 dose levels. All patients have advanced solid tumors, and 7 of the 16 have MSI-high or mismatch repair deficient tumors. Importantly, REC-1245 is well-tolerated. Across the dose levels evaluated to date, there have been no dose-limiting toxicities reported. The most common treatment-related adverse events that have been observed are GI-related: constipation, nausea, and vomiting. As you can see, these are generally low grade with one grade 3 event of nausea and vomiting reported. There have been no treatment-related serious adverse events. Dose escalation is ongoing and recruitment is on track. We have an early PK/PD summary from the evaluated patients to date, and we'll have more dose escalation data and a fuller PK/PD update in the second half of the year. So far, we are seeing predictable dose-dependent exposure with exposures continuing to increase as we move through the dose levels and PK data that are supportive of daily dosing. Our initial PD data also confirm target engagement. We expect, as we move through the next 2 dose levels, to see exposures that are correlated with tumor regressions in mice. Overall, RBM39 represents an end-to-end example of how we're using AI to translate a novel insight into a potential medicine, not just identifying a target, but building a coherent biological hypothesis that informs clinical strategy. I look forward to sharing more data with you later this year. And with that, I'll turn it back to Najat.
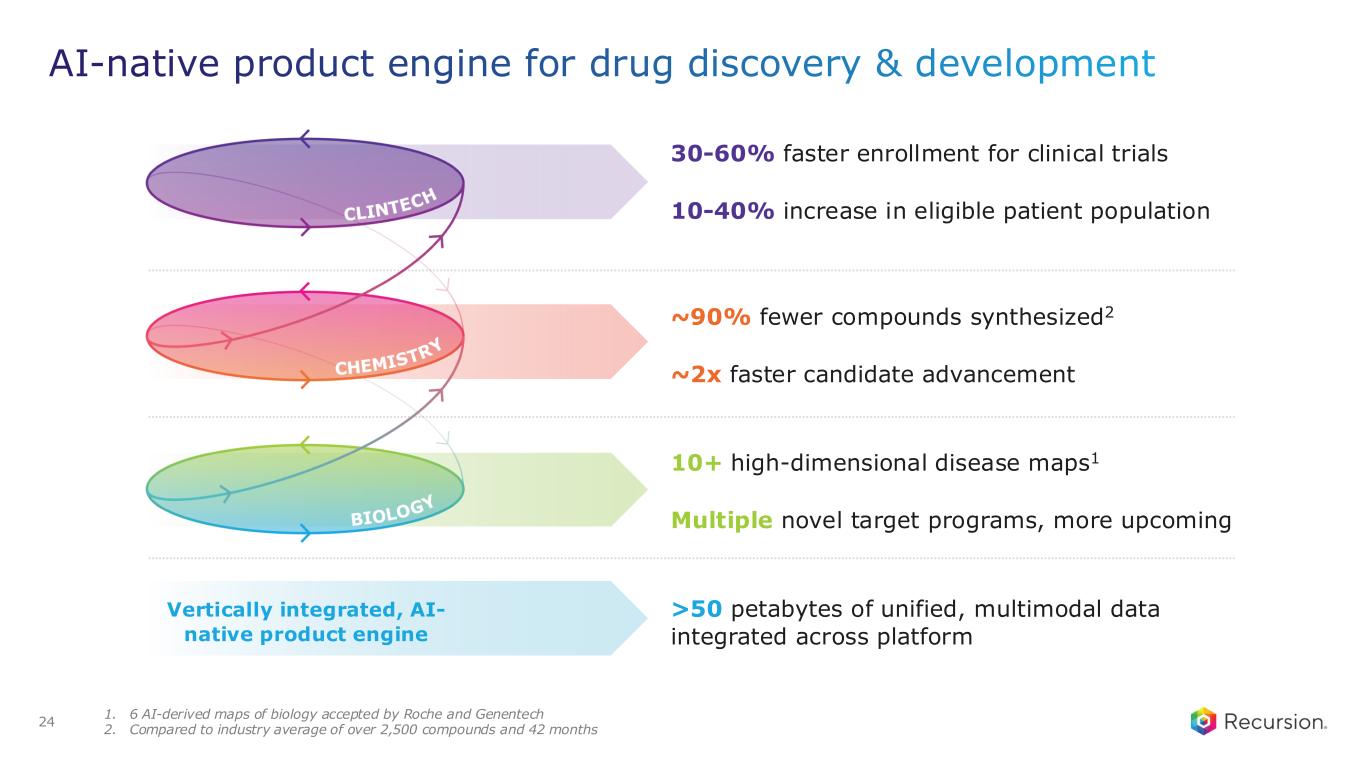
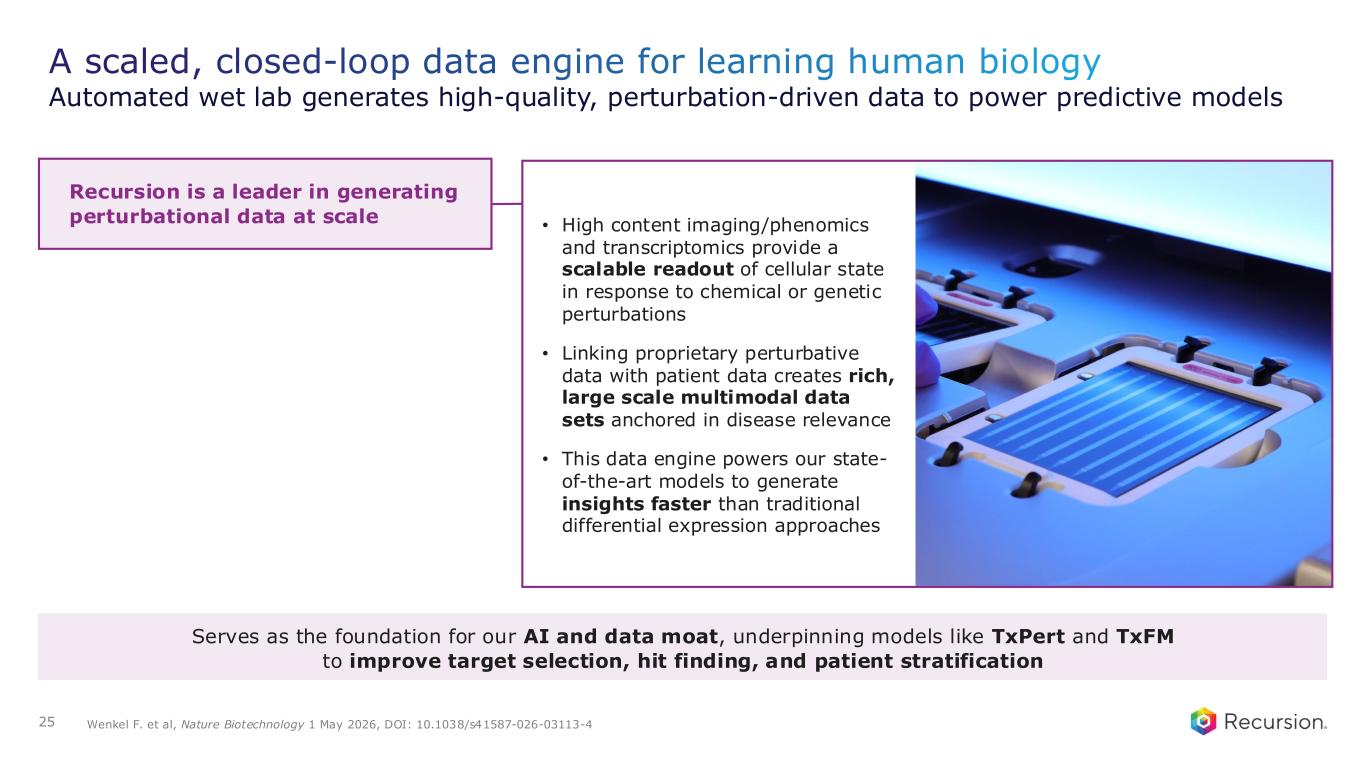
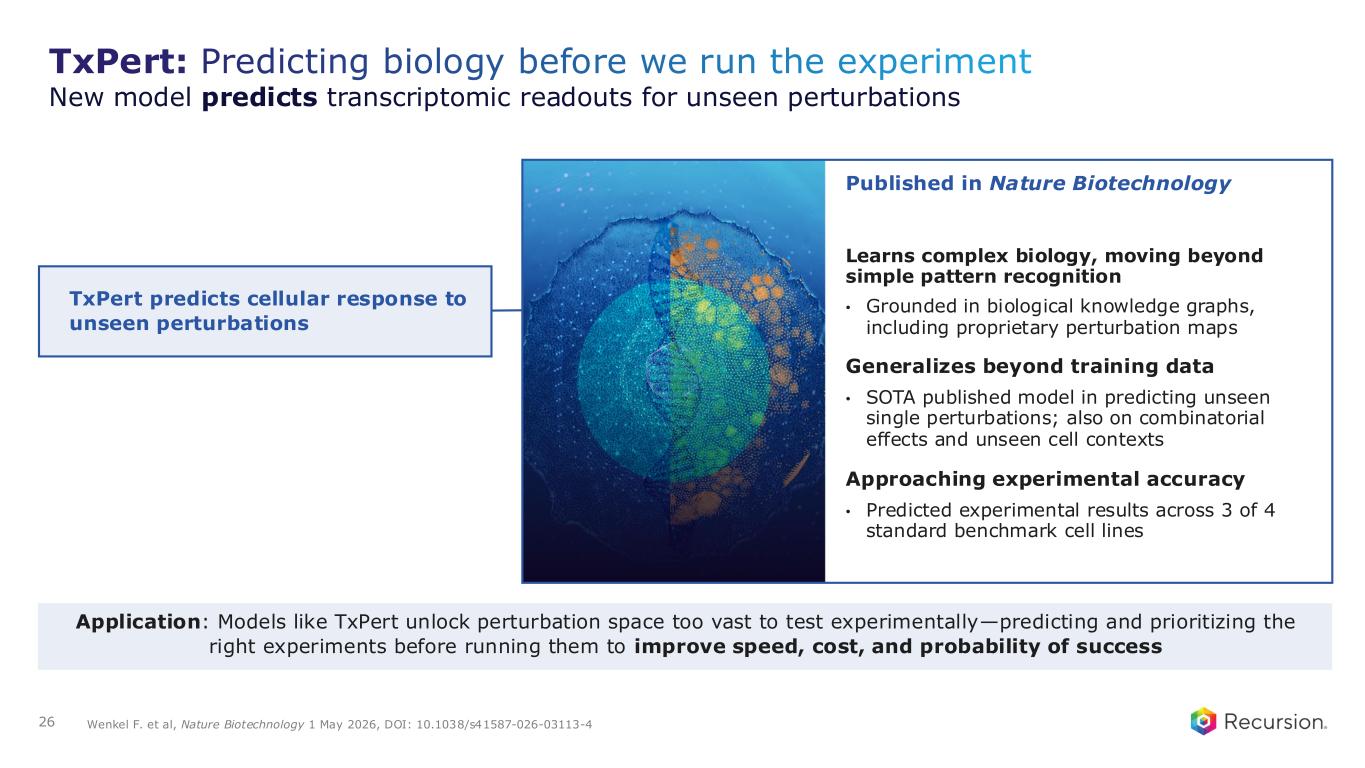
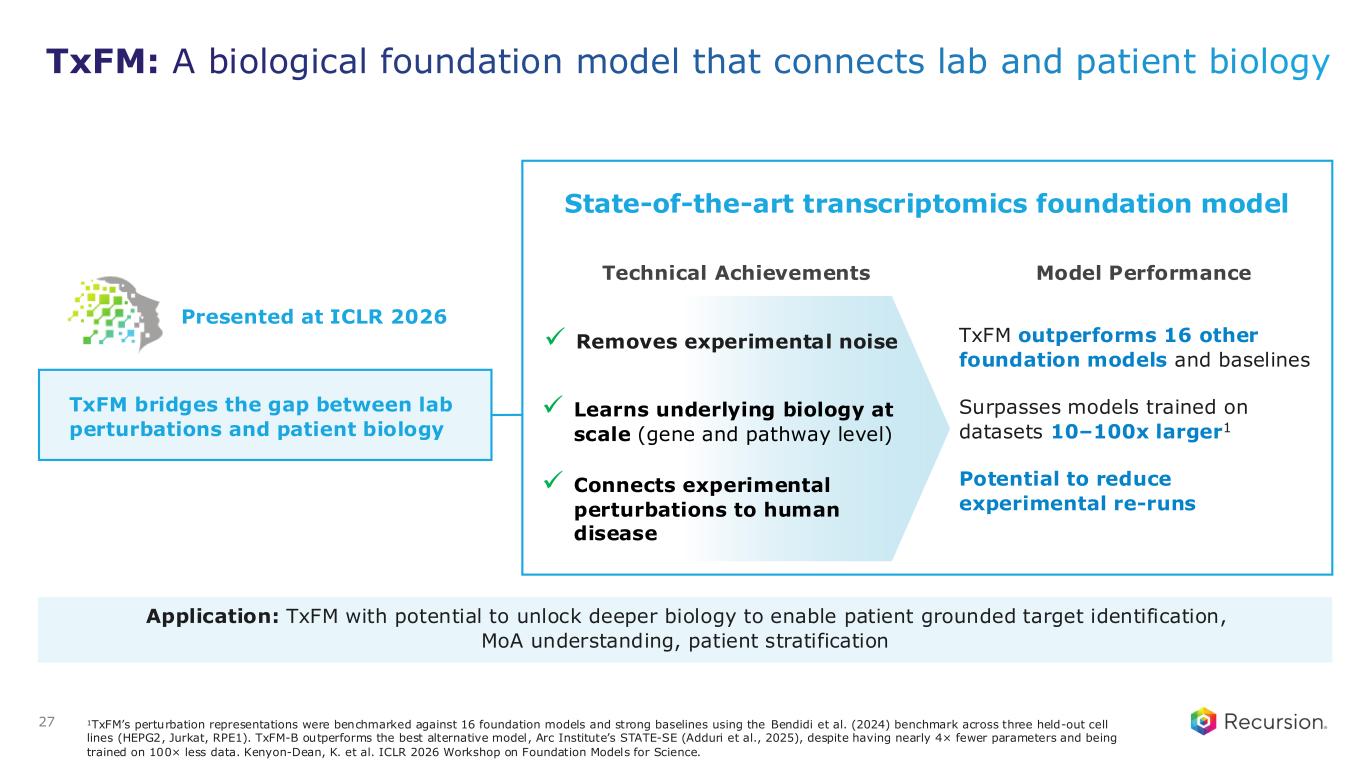
Thank you, Vicki. Now moving on to LSD1, REC-4539. First, I'm pleased to share and announce that we have dosed the first patient in our Phase I clinical trial. But taking a step back, let's discuss a little bit as to why we think that LSD1 is an interesting target for Recursion. As many of you know, LSD1 is an epigenetic regulator with a range of cellular functions and a promising oncology target across multiple cancer types. However, so far, clinically, the potential of LSD1 inhibitors has not been fully met. Previous clinical attempts to drug LSD1 have shown some efficacy, but have been limited by on-target and dose-limiting thrombocytopenia. So while the biology is understood, the challenge has been at the level of the molecule. And therefore, we believe this has the potential to unlock a meaningful therapeutic opportunity, particularly in settings like extensive stage small cell lung cancer, where there are approximately 45,000 patients in the U.S. and EU5 with emerging but still limited treatment options after progression on first-line therapy. For this program, the starting point was our chemistry AI part of the platform really shining. We intentionally moved away from traditional biased chemical space, and instead used a blank white sheet, active learning to explore a broader, information-rich space, which allowed us to identify novel starting points that wouldn't typically be pursued. What that led us to is identifying a new scaffold. We iteratively refined it, ultimately arriving at the compound REC-4539 in approximately 20 months in just over 400 synthesized compounds, much faster and fewer than what is industry standard. Compare that also to what Vicki had mentioned with RBM39, 18 months and about 209 compounds synthesized to date. So you're starting to see these, as I like to call them, green shoots in terms of the number of compounds synthesized, the speed, and also the efficiency, and how we're generating compounds. The focus here, though, was designing a molecule with properties that directly address the limitations we've seen in this class to date, specifically reversibility and a shorter predicted human half-life to potentially reduce the risk of cytopenias that have been one of the dose-limiting factors for prior LSD1 inhibitors. We're also sharing some preclinical data in small cell lung cancer that demonstrate that this compound had a more minimal impact on platelets while maintaining efficacy, which is not shown here, but we've seen that data as well, being comparable in efficacy to other agents in the class but having less impact on platelets. In addition, another feature of this compound is that it's brain penetrant, which may be particularly relevant for patients with small cell lung cancer where up to 50% develop brain metastases. This differentiation and the potential to improve tolerability has encouraged us to advance the compound into Phase I. We had our first patient dosed in April. This is a dose escalation study in select solid tumors, including small cell lung cancer, with expansion cohorts planned following the initial escalation phase. I want to make one thing really clear. Vicki and team are structuring these programs to enable rapid data-driven decision-making. This is how we really manage our capital allocation, specifically to address rapidly whether the emerging clinical profile really supports the hypothesis of mitigating or reducing the risk of thrombocytopenia. We expect to share initial PK and safety data in the second half of 2027. I think I've covered most of this, but similar to what Vicki shared, here's another example where we use our AI platform to solve for design challenges around a biology that's more validated, optimizing molecules where we believe there's been limitations to date. And recall, there are no FDA-approved LSD1 inhibitors to date, despite a well-defined patient population and significant unmet need that remains for patients. We look forward to sharing more clinical data for this program next year. Now let's go to our second pillar, which is incredibly important. Beyond our portfolio, underpinning a lot of what we're doing is continuing to advance our end-to-end AI product engine, pushing the boundaries. So we continue to remain at the forefront of AI-driven innovation. Let me walk you through the platform and also some of the facts and the stats around how we're doing. We built the Recursion platform specifically to address the most persistent bottlenecks in drug discovery and development. And so we're always looking at how we're doing versus industry. So let's start with biology. We have generated more than 10 high-dimensional maps of disease biology. More than half of them have been in partnership with Roche and Genentech. These are already driving multiple novel programs that will target programs in our internal pipeline and we're also working actively with our partners at Roche and Genentech to translate these maps into novel targets and first-in-class programs. Why are these maps important? Biology is a systems-level approach. We need to understand the interconnected circuits. Enhancing our ability to identify and prioritize targets with better confidence and better understanding of the underlying biology is critical to determining the root causes. We are also synthesizing, as you heard me share briefly, more and more compounds where we are designing and synthesizing 90% fewer compounds than the industry benchmark, so about 330 compounds on average versus 2,500 to 5,000 compounds, which is the industry standard today, while also advancing these programs to development candidates roughly twice as fast. This is a meaningful step change in both efficiency and cycle time, and something that we watch very carefully on an ongoing basis. The next point is ClinTech capabilities. Where we have deployed it, we're already seeing about 30% to 60% faster trial enrollment. This is very important for us, both for rare diseases and competitive areas such as oncology, while increasing the eligible patient population for some of these programs from 10% to 40%. This directly impacts our timelines and the speed at which we can generate high-quality clinical data. The underpinning of it all is an integrated platform with more than 50 petabytes of proprietary multimodal data. This is incredibly critical not just for building purposeful models, but ensuring that we have our data moat that we not just invest in, but continue to expand. These are not theoretical or isolated improvements. These are real, tangible gains that we keep measuring and focusing on to reinforce how our platform is changing the way we are discovering and developing our medicines. Again, I always like to say there are green shoots, but this is how we are pushing the frontier of what's possible with our platform. Now let me double-click on a couple of recent examples in the biology layer where we're really pushing the next generation of our models that were recently published. Big picture, one area of focus for us in our biology platform is learning the language of biology. Sounds simple, not easy, incredibly important. We do it across many data layers by generating perturbations at scale, whether genetic, chemical, and so forth. Why is that important? What is our goal? Our goal is to, a, understand biology more comprehensively; b, be able to predict and simulate perturbations before we are even running a single experiment; and c, actually generalize beyond the data that we've already seen. That's really important with these foundation models. You want to predict responses in new, out-of-distribution contexts, such as novel targets, combinations, and cell types. Given the vastness of the biological space and how little best in industry know, this has the potential to unlock areas that remain intractable today. That becomes even more powerful when we connect different data layers—high-content cell imaging, transcriptomics, proteomics, patient data, and more—to really have a more unified view of biology. This is not just theoretical. We're making progress here already. Step one is to develop a new generation of models. Let me share with you two recent advances in transcriptomics foundation models that we published in the last month. The first is TxPert, which we recently published in Nature Biotechnology. TxPert is a model designed to predict how gene expression changes in response to different perturbations, essentially helping us to understand biology and how it will respond before we run the experiments. Similar to what you saw in chemistry, the reason we can reduce the number of compounds we synthesize is because we predict and simulate more, and then we make less. How can you do that more in biology? It's important for us to understand the systems approach across different data layers and be able to predict well so that we can do less experimentation and only do the experimentation that really matters. What's particularly exciting about this model is that it's learning patterns in biology. It's not just memorizing; it's actually learning the underlying patterns. The second is generalizing beyond the data it was trained on. This is an important start to predicting responses to new perturbations, new combinations, and even new cell types. Watch this area. I think this is going to be really important in biology and foundation models given the vastness of what we're working with. It's an important first step towards how we think about building a virtual cell, a term that is overused, but the importance is being able to simulate and explore biology more comprehensively and computationally before moving into the lab. This is incredibly important so that we can be more effective and efficient and ultimately improve the probability of the targets that we could put into our programs. Next is another model, which is complementary: TxFM, our transcriptomics foundation model, which represents a significant step in actually connecting lab biology to patient biology. I won't go into the details here, but want to highlight a couple of things. First, it is built on a highly curated combination of both proprietary and public data, bringing together diverse datasets into a shared representation space. Why is this important? There's a lot of conversation about whether quantity or quality matters. Both matter. From some of the early insights here, the quality and the model architecture were really important to ensure great model performance. So what's exciting is the following: number one, the result is a model that surfaces a much richer understanding of biology and reduces experimental noise, including batch effects; number two, it outperforms a lot of leading foundation models, and more importantly, it outperforms models that are trained on 100 times larger datasets, demonstrating the advantage of our data curation approach and model architecture. I also like the interpretability. That's where we're starting to go, and again it's early days. It doesn't just rank genes; it reveals gene networks, circuits, and patient subtypes from RNA data, so that transcriptomics can become a more systematic engine for understanding the mechanistic and target hypotheses that underpin one-off analyses. There is so much rich data, and we're driving to understand that even better. Practically, it's about how we get more efficient in the experiments we run, do fewer reruns, do better cross-study comparison, and use our resources more efficiently. Today, both these models are starting to be deployed in our platform. For TxFM, we're starting to leverage it for target identification, better mechanistic understanding, and patient stratification. We'll, as always, in the months and years to come, share how this is truly impacting our platform. That's what we care about: how we take data models to show the translation of proof into our programs, into our partner programs, and progress better medicines for patients. With that, I'm going to turn over for our third pillar, which is how do we drive all of this important work with good discipline and good ambition. Ben?
Thank you, Najat. Our core focus from a financial perspective is ensuring we have adequate runway to achieve multiple upcoming milestones. We continued our trend of operating discipline with a 30% year-over-year reduction in cash operating expenses. We were able to achieve these savings while also growing our pipeline, partnerships, and platform by focusing only on those operations that had clear and measurable impact. In addition to our operational discipline and infrastructure simplification, we also expect ongoing efficiency gains from our technology advancements and the adoption of agents. During the quarter, we received our fifth milestone from Sanofi, advancing a potential first-in-class program for a novel biological target. We closed the quarter with $665 million in cash and equivalents, which we believe provides operating runway through early 2028 without additional financing. For 2026, we are maintaining our cash operating expense guidance of less than $390 million, which fully funds our expected milestones and partnerships during the period. And to take you through those milestones, I'll turn it back over to Najat.
Thank you so much, Ben. And look, I'm going to close by saying we have a lot of important work ahead of us and very exciting work ahead of us. As we look ahead, we have a clear and consistent cadence of milestones, both across our wholly owned pipeline and our partner portfolio. In our wholly owned pipeline, we expect multiple clinical readouts over the next 12 to 18 months; in fact, for every single one of our clinical stage programs. Continuing to build on clinical evidence and test the hypothesis underlying our platform. In parallel, we're seeing continued progress across our partnered portfolio. I'll recap the 2 potential unlocks I mentioned: one, looking at the use of AI to develop novel compounds for difficult-to-drug targets. We're excited about our work with Sanofi here and some of the development candidate decisions coming up in the next 12 to 18 months. And with Roche and Genentech, to take all of these large, multimodal maps that's helping us understand biology better and really translating that to novel targets and first-in-class programs. Taken together, this creates a diversified sets of catalysts and also the increasing momentum, as you're seeing, month-over-month, week-over-week, as we look to take and harness all of what AI and our dramatically excellent team can do to turn that into meaningful outcomes. I'll just close by saying we are focused on building an increasing body of evidence that this approach can translate, advancing differentiated programs, unlocking new biology, and doing that work with improved speed and efficiency. And that's what gives us confidence in the path forward. The momentum you see, the work that the teams are doing, but also the system behind it and its potential to generate outcomes over time in a repeatable fashion for patients, our partners, and our shareholders. Thank you again for your time and attention, and we will open it up now for questions. Great. So let's dive in. I have Vicki and Ben, who will help me cover some of these questions. So the first question is from Dennis at Jefferies and Priyanka at JPM on the REC-1245 program. Can you talk about the level of target engagement that you feel is needed to drive efficacy and where you are relative to those levels? What are common on-target safety and tolerability issues that you're hoping to avoid with your approach? And how are you thinking about biomarkers being explored? Well, maybe I'll just kick it off and then I'll hand it over to Vicki to also share additional details. I'll go in order of second, third, and first. So what are common on-target safety tolerability issues that you're hoping to avoid? Look, first of all, we are encouraged by the favorable safety and tolerability profile that we see to date. As you saw, 90% of what we see so far are grade 1 and 2, mostly GI, and no DLTs to date. In terms of RBM39, there are areas that we would usually keep an eye on in terms of potential toxicities, specifically hematologic toxicity (heme tox). And to date, we have not seen any grade 3 hematologic toxicity at all. So that is encouraging. But again, we're in the middle of dose escalation. So more to come, as Vicki mentioned, second half of 2027. And in terms of target engagement, we already have some PD data that we shared, and Vicki can share more about that. But we're seeing good target engagement. We've confirmed that to date. As we have more dose escalation, what we've seen preclinically is about 70% to 80% degradation was sufficient at efficacious doses, but we'll be tracking that as we continue further. Vicki, did you want to add anything more to those two questions?
So coming back to the safety and tolerability issues, again, what we've seen so far is mostly low-grade GI toxicity. We'll certainly continue to monitor that as we move forward. Hematologic toxicity, which is a concern here, is something we're really not seeing at this point. Again, we'll continue to monitor as we continue to increase the dose, and we'll have more data for you there in the second half of this year. Relative to target engagement, I think the estimates are spot on. I'll add that we are coming close now within the next 2 dose levels to being at the exposure levels where we saw tumor regressions in mice. So I think that's an important point as well. Obviously, we'll continue to monitor the target engagement in terms of RBM39 degradation and, again, have a more fulsome update in the second half of the year.
Thank you, Vicki. And just the last question was, how are you thinking about biomarkers being explored? As Vicki mentioned during the presentation, we're looking across select biomarkers. And, of course, as the data matures, we will look at relative benefits across those biomarkers. More to come second half of 2026. Thank you for the great question. All right, next question from Gil at Needham, Alec from Bank of America, Sean from Morgan Stanley, Brendan from Cowen, and others on REC-4881. Given the encouraging Phase II data for REC-4881 in FAP and ongoing FDA engagements, what are the key uncertainties around the registrational pathway? We have 3 questions here. I'll just start one at a time, so we can keep track. I'll kick it off, but Vicki, it would be great to get your thoughts. We're very excited about the data that we see with FAP. And with every day that goes by, we engage with more FAP patients; really not just the unmet need, but how underserved these patients are is becoming even more and more apparent. We have a significant polyp burden reduction and durability that we've seen to date. I would say the main areas of focus with the FDA is what would be for any asset that's a first-in-disease. We have other assets in our portfolio that are best-in-class, where the regulatory approach is already very defined. For a first-in-disease, it's really around patient population, endpoint that has clinically meaningful benefit, and then, of course, dose and dose escalation. But those are the conversations. And as Vicki mentioned and I mentioned, we've already started that engagement. Anything to add?
Yes. Because there really is a lack of regulatory precedent, it's important for us to work closely with the FDA in terms of defining the registrational path. To that end, we've already initiated that engagement within the oncology review division, and we've also requested input from the GI division. And certainly, as we go about these discussions, we're thinking about leveraging the rare disease framework as well. So we can derisk this program by really closely aligning with FDA on what are clinically meaningful endpoints for patients that will help us define the primary endpoint for our pivotal study.
The next question is still on REC-4881. Has there been any shift to timing for FAP regulatory? And when will we see additional data? So a couple of things. We're on track with it. We had planned to initiate FDA engagement first half of 2026 and we're actually a bit ahead of schedule. We have initiated FDA engagement. And as Vicki mentioned, we expect us to be working with the FDA very closely, given it's a first-in-disease on our potential registrational study. And then when will we see additional data? In terms of additional data, we have already initiated 18 and over patients. We're already recruiting those patients. And we'll also have potentially additional data from our Phase II that we will share either here or at a forum going forward. But we're on track. Have you leveraged any Clinical Development capabilities from your platform in assembling the proposed pivotal study design? Great question. A couple of areas. Number one, if you recall, the natural history that we did in parallel with our clinical program has been really important for a few reasons. This is a rare disease with limited literature. The natural history work has allowed us to not just understand patient trajectory, but also helped us as we think about how to power the study, what endpoints are important, and so forth. So it gives us a much richer contextual understanding, and then also incorporating that in terms of our study design as well. In addition to that, for our 18 and over cohort plus our potential registrational study, we are also going to be using our clinical development AI capabilities for recruitment. This is a rare disease. We want to be much more efficient and use these approaches to go to where patients are and recruit with speed and rigor. Great. Next question from Bruce, Philip, Rishabh, and others on the platform. How does Recursion evaluate whether its platform is improving its ability to identify and eliminate lower-quality candidates earlier in the discovery process compared with prior years? Let me answer that one first. So as I shared earlier today, we look at every segment of our platform, and we're really looking at how is it that we can design better molecules faster. One of the things is you asked about lower-quality candidates. This is where if you can actually simulate more, predict which compounds would actually have better versus worse ADMET properties. But this is where active learning and multiparameter optimization, complexity that the industry can do in a very sequential way, we do in a much more efficient way. We simulate online and only synthesize the compounds that we have confidence in. That's where you see some of the numbers shifting pretty dramatically, cycle times becoming half and also 90% fewer compounds synthesized. So that's just one example as to how we track it. The other thing I would say on the biology side, the maps of biology give you a lot of hypotheses in terms of potential novel targets. But we pair that with really robust experimental validation. I think that is incredibly important to do both. That allows us to look at targets that no one has looked at before. This is where novel biology is coming from. But we always pair that with rigorous experimentation. And that's where the lab, the wet and dry lab, is incredibly important for us because we can do it at speed, we can learn fast, and all that data is captured to make our models better. So we are a continuous and rapid learning organization. And I will say the integration with Exscientia has really helped there, because now you have both the biology and the chemistry side sitting side by side. And we iterate and learn from that. Okay. What are the investments you're looking to make on the platform? Compute, data generation, models? Look, our strategy is we invest in our programs with our platform, and that platform needs to remain differentiated. So we surgically invest in areas that matter. As an example, on the clinical development side, you've seen the investment we have made, but there's a reason: it's to make a better product. So how do we recruit faster, how do we pick the right patients. In our chemistry and design platform, we're continuously evolving and iterating on our models, and we'll share more in due time. And then in our biology platform, you've seen the investments we're making in state-of-the-art transcriptomics models. But again, they're all with a purpose. How do we improve the targets that we're putting into our programs, the compounds that are high quality, and ensuring that we execute our programs with flawless clinical execution, but also pick the right patients and increase our signal to noise. Maybe I'll take one more question. I want to take as many. I know we're a little bit over time. From Gil and Sean on partnership strategy. Any expected guidance for a potential clinical opt-in from partners? Will we receive an update on this? Ben, do you want to share on that one?
Sure. Happy to. So as we continue to advance the programs along with Sanofi and begin to move different programs from Roche into the design phase, we absolutely expect to see some of those five programs that have hit their early discovery milestones move into the opt-in, and we're working very closely with Sanofi to make that happen as quickly as possible. I think there's also a broader point that's really important around the partnerships. If you take a step back, and we get a lot of questions on what's our partnership strategy, where do we plan to go in the future, if you take a step back to what we do, part of our mandate is how do you create a risk-diversified model for being able to be an investor in the biotech space. And so we obviously have transformative potential medicines that are coming up through our internal pipeline. But you also have to look at our partnership business and see how we've been able to advance programs and do it in a capital-efficient way and really diversify that risk and diversify what the long-term benefits of that are. So we will absolutely continue to drive that partnership forward along with our internal pipeline, and we'll balance out how we're getting the upfront payments while also still maintaining a lot of that downstream economics.
But suffice to say, we're working actively on this, and, of course, we'll share updates in the next two months. Last question. You've generated over $500 million in partner-related payments to date. How should we think about the forward trajectory of platform monetization, particularly the balance between near-term milestones and retaining long-term economics and wholly-owned programs? I think it's very similar to what Ben said. Our platform is focused on generating better products. That's what we focus on, whether we do it internally or with partners. And we create optionality in terms of our wholly owned programs. Some of the programs, again, we're data-driven in our approaches in terms of could be wholly owned, could be partnered, could be outlicensed, and same goes for some of our partnered programs as well. So with that, I'll just close by saying thank you so much for your time and attention. Thank you for all of the questions. We have a lot of momentum, a lot of important work ahead, and we continue to move that forward and excited to share more updates in the coming months and years as well. Thank you again.